
Abstract
Proliferative retinopathies, such as neovascular age–related macular degeneration and proliferative diabetic retinopathy, are a special health issue due to their contribution to irreversible blindness. Although the promoting conditions and physiopathology of proliferative retinopathies are different, these feature a highly detrimental angiogenesis driven by the overproduction of vascular endothelial growth factor (VEGF). This article describes the mechanism of action of ocular antiangiogenic therapies currently found in clinical development. Systems classify accordingly as (a) novel anti-VEGF systems, (b) molecules targeting non-VEGF pathways, and (c) gene therapies. Whereas most therapies are designed to neutralize VEGF, there is a significant set of products with diverse complexity and mechanism of action. Anti-VEGF therapies are still the most studied approach to tackle angiogenesis. Therapies targeting non-VEGF pathways, however, are highlighted because they could be an option for patients nonresponsive to anti-VEGF therapies. Finally, gene therapy is a promissory technology platform but still is subject to demonstrate safety and efficacy.
Keywords
Introduction
Proliferative retinopathies are severe sight-threatening pathologies that feature uncontrolled angiogenesis. Diseases displaying this feature, such as neovascular age–related macular degeneration (wet AMD) and proliferative diabetic retinopathy (PDR), are leading causes of irreversible blindness in adults. Given their relevance, the World Health Organization (WHO) has an active agenda to develop strategies for avoiding and treating these diseases. 1 Neovascularization in wet AMD occurs from the choroid into the subretinal space and characterizes by a rapid progression and severity. Current estimations of incidence indicate that AMD affects 0.5 per 1000 individuals <70 years old, and 6.7 per 1000 individuals >70 years old. 2 On the contrary, diabetic retinopathy (DR) is an ocular condition triggered by diabetes mellitus. The persistent damage on the retinal microvasculature due to sustained hyperglycemia leads to local ischemia (i.e. hypoxia). This upregulates the production of pro-angiogenic factors that increase vascular permeability, producing the presence of blood and fluid that can cause mild vision changes. DR can evolve into PDR when neovascularization is produced, which can produce vitreous hemorrhage, retinal detachment, neovascular glaucoma, and vision loss.3–5 Probability of evolution from PD into PDR is about 17.6% within 5 years in patients diagnosed with moderate diabetic retinopathy. 6
Although proliferative retinopathies are caused by different factors, angiogenesis is their most detrimental manifestation. Seminal paper of Miller et al. 7 demonstrated the key role played by the vascular endothelial growth factor (VEGF) in ocular angiogenesis (growth of new capillaries from preexisting blood vessels). VEGF family is glycoproteins that bind to specific membrane receptors, termed VEGFRs. The formation of the VEGF/VEGFR complex is paramount for different signaling processes involved in the formation of new blood vessels, such as the modulation of vascular permeability, cellular migration, proliferation, and cellular survival. Actually, this system is considered the master regulator of angiogenesis and lymphangiogenesis.8,9 VEGF family is composed of five members, namely, VEGF-A, VEGF-B, VEGF-C, VEGF-D, and placental growth factor (PlGF). These molecules bind with corresponding membrane-bound receptors, namely, VEGFR-1, VEGFR-2, and VEGFR-3. Figure 1 shows the binding specificities of VEGF members toward corresponding receptors. VEGF-A, VEGF-C, and VEGF-D can bind and activate VEGFR-2, the main signaling receptor for angiogenesis and vascular permeability. On the contrary, VEGF-C and VEGF-D are the only known ligands for VEGFR-3, which also is an important driver of angiogenesis and lymphangiogenesis.10,11 VEGF-A is, however, highlighted due to its major role in pathological neovascularization. 12
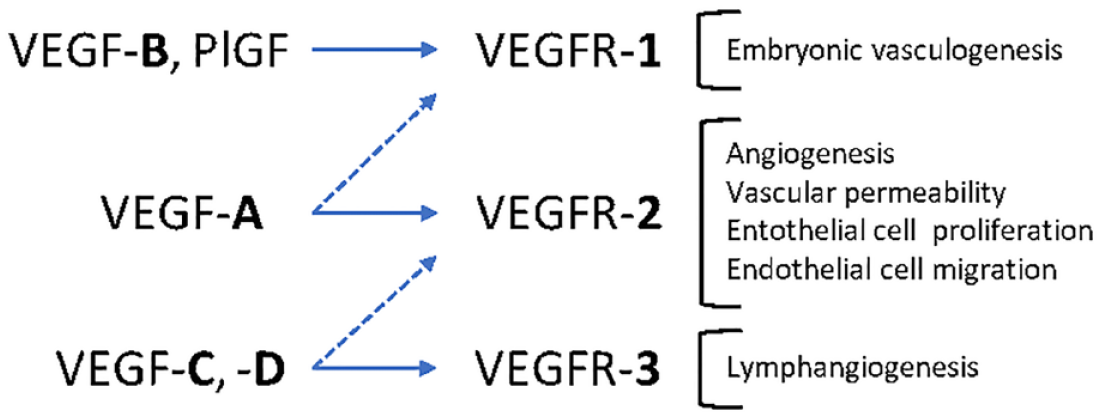
Selectivity of vascular endothelial growth factor (VEGF) toward its three major types of receptors (VEGFRs). VEGF-A and B activate VEGFR-1 to promote embryonic vasculogenesis. VEGF-A acts on VEGFR-2 to promote angiogenesis in many physiological and pathological conditions. VEGF-C and D act on VEGFR-3 in the lymphatic vasculature to promote lymphangiogenesis.
Prior to the anti-VEGF era, Verteporfin (VP) was the most used therapy to inhibit angiogenesis. VP is a small molecule that produces upon local photo-stimulation short-lasting free radicals that damage the endothelium, occluding the newly formed vessels. The use of VP, however, has declined due to its unspecific mechanism of action, side effects, and inefficacy in the long term. 13 Other therapies available to control angiogenesis are through intravitreal implants loaded with corticosteroids, which have shown acceptable long-term safety and efficacy.14,15 Most used strategy today toward ocular angiogenesis, however, is via neutralization of VEGF. 5 Commercially available options include to pegaptanib (Macugen®), ranibizumab (Lucentis®), bevacizumab (Avastin®), aflibercept (Eylea®), conbercept (Lumitin®), and brolucizumab (Beovu®). These are biopharmaceuticals that differ in size, intravitreal half-life, and selectivity toward VEGF protein family and isoforms. Briefly, first anti-VEGF therapy approved by US Food and Drug Administration (FDA) was pegaptanib (Macugen®). This is an aptamer designed to bind specifically VEGF165. 16 On the contrary, Bevacuzimab (BCZ) is a full-length antibody that binds all VEGF-A isoforms. BCZ was approved in 2004 for advanced colon cancer but used off-label for proliferative retinopathies. 17 Ranibizumab is Fab fragment that derives from BCZ. It was developed under the idea that size of BCZ could compromise its diffusion through retina and, therefore, efficacy.17,18 It was approved by FDA in 2006 for wet AMD. As regard to aflibercept, this is a fusion protein containing binding elements of the VEGFR-1 and VEGFR-2 fused to the Fc portion of IgG1. This endows the ability to bind VEGF-A, VEGF-B, and PlGF. 19 Aflibercept was approved by FDA in 2011. In the case of Conbercept, this is also a fusion protein with similar characteristics than aflibercept, which was approved in 2013 by the National Medical Products Administration of China (NMPA). 20 Brolucizumab is a single-chain antibody fragment with affinity to all VEGF-A isoforms. 21 It was approved by FDA in 2019. Anti-VEGF therapies are administered as intravitreal injections to override the physiological barriers that limit topical bioavailability, to achieve therapeutic levels of drug molecules within the retinal space, and to avoid toxicities associated with their systemic administration.22–24 Therapy, however, requires repeated and long-term injections to halt disease and improve vision. 25 Furthermore, even though intravitreal anti-VEGF doses are small, these molecules display high potencies. Hence, intravitreal clearance toward systemic circulation can suppress the circulating VEGF and produce adverse effects 26 In the case of brolucizumab, some patients have reported retinal vasculitis and intraocular inflammation after intravitreal injection. 27 Furthermore, the price and need of continuous administrations and monitoring, and the reluctance of patients toward intravitreal administration can contribute to lack of treatment adherence. 28
This short review provides a comprehensive analysis of therapies found in clinical trials designed to treat proliferative retinopathies. The aim is to generate a clear understanding of their mechanism of action, differences among them, and the potential benefits that these therapies could represent for clinicians and patients.
Materials and methods
An extensive search in intellectual property files was conducted by Observatorio Tecnologico (Zapopan, Jal, MX, https://www.observatoriotecnologico.org.mx/). Collection of data was performed using a software-based IA analysis as well as individual searches in databases such as in USPTO, Espacenet, PubMed, and ClinicalTrials. Keywords utilized to identify relevant documents included ‘proliferative retinopathy’ or ‘macular degeneration’ or ‘proliferative diabetic retinopathy’ or ‘diabetic macular edema’ or ‘DME’ or ‘macular degeneration retinal’, or ‘age-related’, or ‘AMD’, or ‘wet AMD’ or ‘exudative AMD’ or ‘treatment’ and their possible combination. The analysis resulted in 309 patents. Data were analyzed in accordance with their innovation areas, and further clustered as cell therapy, early detection methods of retinal diseases, therapies and molecules, and drug targets. Findings were further delimited to developments in clinical trials designed to tackle angiogenesis.
Results
As described above, proliferative retinopathies feature an uncontrolled neovascularization triggered by an overexpression of VEGF. Developments found in clinical trials classify in accordance with their pharmacological targets as follows: (a) antiedematous therapies that block the formation of the VEGF–VEGFR complex, (b) compounds that modulate inflammation or oxidative stress, and (c) gene therapies. These are described in the following sections.
Antiedematous therapies
Developments found in this category aim to block the interaction of VEGF with VEGFR, which inhibits the triggering point of the angiogenesis cascade. Many therapies in this section are biopharmaceuticals that neutralize VEGF molecules. 22 Therefore, their mechanism of action occurs at the extracellular domain. A significative set of therapies in development, however, target an intracellular mechanism of action (see Figure 2). Active pharmaceutical ingredients (APIs) in these systems are small molecules from the tyrosine kinase inhibitors (TKIs) family. TKI molecules interfere competitively with the ATP-binding site of receptors, avoiding thus their activation upon VEGF stimulus. TKIs display different selectivity and potency toward VEGFR-1, VEGFR-2, and VEGFR-3.29,30 Relevant characteristics antiedematous systems approved and in development are described in Table 1 (commercially available therapies are also included for comparison purposes).

Schematic representation of the mechanism of action of anti-VEGF therapies.
Relevant characteristics of anti-VEGF molecules commercially available and in clinical trials.

NMPA, National Medical Products Administration of China; NR, not reported; TKI, tyrosine kinase inhibitors.
Antiedematous biopharmaceuticals
Faricimab. Phase III. Roche/Genentech
Faricimab (previously RG7716) is a novel monoclonal antibody designed to inhibit simultaneously and independently two ligands involved in angiogenesis: VEGF-A and angiopoietin-2 (Ang-2). 39 As previously described, neutralization of VEGF-A has shown to suppress efficiently neovascularization. Approved biopharmaceuticals (e.g. ranibizumab, aflibercept, and brolucizumab) follow this mechanism of action (see Table 1). On the contrary, angiopoietins (Ang-1 and Ang-2) are growth factors that interact competitively toward endothelium-specific receptor tyrosine kinase Tie-2. This pathway plays an important and complementary role alongside VEGF to regulate vascular homeostasis, vessel permeability, inflammation, and angiogenic responses. Ang-1/Tie-2 signaling is involved in inflammation prevention and vessel maturation (particularly after angiogenesis). On the contrary, Ang-2/Tie-2 system increases vascular instability, endothelial activation, and remodeling. Due to their antagonist properties, the Ang-1:Ang-2 ratio is paramount for vascular homeostasis. 40 However, conditions such as hypoxia, hyperglycemia, and/or oxidative stress, can upregulate the formation of Ang-2, which prone to endothelial activation. Dual mechanism of Faricimab highlights because blockage of VEGF-A halt angiogenesis, whereas neutralization of Ang-2 favors the Ang-1/Tie-2 complexation to stabilize vasculature. Faricimab equilibrium dissociation constant (KD) for Ang-2 is 22 nM and about 3 nM for VEGF-A (comparable with the KD of ranibizumab).39–41 Clinical trials have been performed with intravitreal doses of 6 mg, showing an enhanced treatment durability (up to 24 weeks).31,39
OPT-302. Phase III. Opthea
OPT-302 is a novel fusion protein that displays a high affinity toward VEGF-C and VEGF-D (KD is about 5 pM and 0.5 nM, respectively). Although the angiogenic effect of VEGF-A has demonstrated to be higher than other member of the VEGF family, the concentration and activity of the VEGF-C and VEGF-D have been found increased in patients receiving anti-VEGF-A treatments (e.g. BCZ). Consequently, these patients undergo suboptimal response to treatment because VEGF-C and VEGF-D can also activate VEGFR-2 (Figure 1). 42 It is plausible that upregulation of VEGF-C and VEGF-D is a physiological response driven by the fact that factors that induce the overproduction of VEGF-A, such as hypoxia, remain unresolved. 10 Data from clinical trials have shown that combining OPT-302 (2 mg) with ranibizumab (0.5 mg) provide an additive effect in comparison with monotherapy, which is relevant to design better responsive and longer lasting therapies. 10
KSI-301. Phase II. Kodiak
This system is a novel full-length antibody covalently bonded to an optically clear high molecular weight phosphorylcholine biopolymer. Due to this design characteristics, its molecular size is significantly larger than conventional anti-VEGF molecules (950 kDa, see Table 1). 43 Size and structure of KSI-301 serve two purposes. On one hand, conjugated antibody has activity toward all isoforms of VEGF-A, as other primary anti-VEGF agents. The large size of KSI-301, however, limits its intravitreal diffusion. This decreases its ocular clearance, providing a long-lasting action. Therefore, KSI-301 aims to increase the time required for reinjection. Clinical studies were performed using a dose of 5 mg and were compared with 2 mg dose of aflibercept.44,45 Preliminary results showed significant outcomes for patients with wet AMD in terms of efficacy and durability.
Inhibitors of VEGFR
GB-102. Phase II. Graybug vision
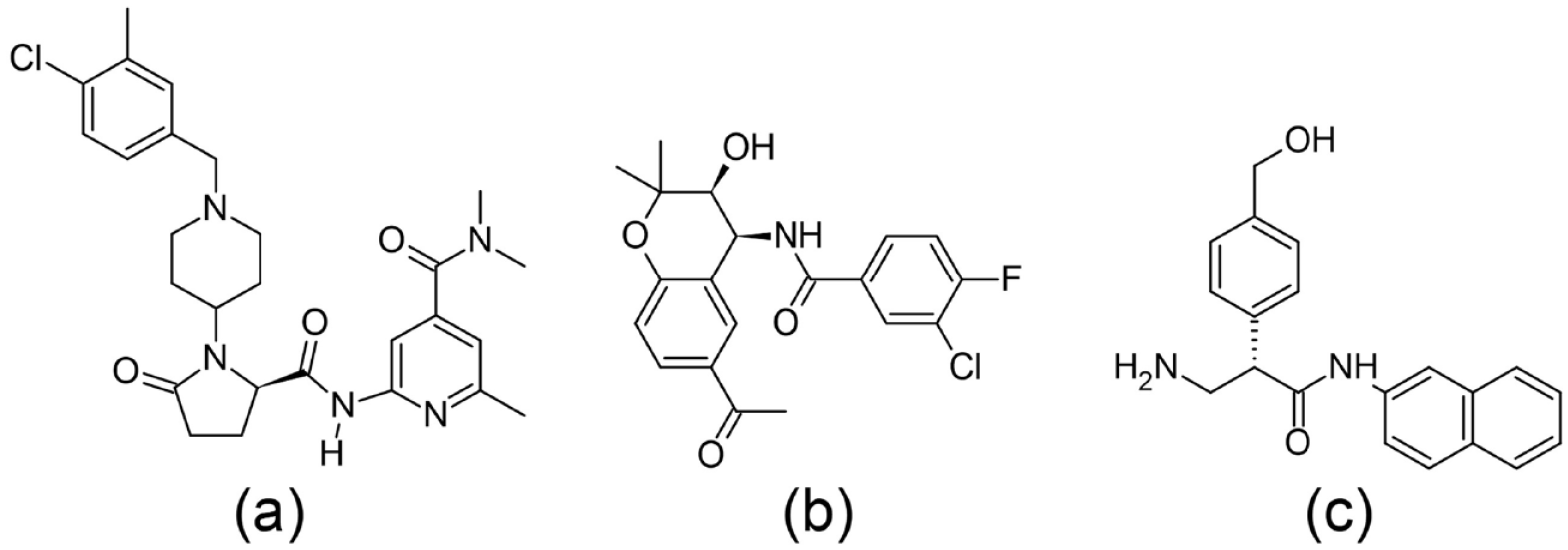
API used in this formulation is sunitinib maleate [Figure 3(a)], a TKI with activity toward VEGFR-1, VEGFR-2, and VEGFR-3. This development is formulated as a solid intravitreal dosage form that endows a long-lasting release of the API. For this aim, 1–2 mg of sunitinib maleate is encapsulated within a biodegradable and biocompatible polymer that degrades slowly over time. This permits to reduce the intravitreal dosing interval to twice per year. Results obtained in ALTISSIMO trial indicate that formulation does not induce inflammatory response and stays in the injection site to avoid clouding the visual axis.41,46,47
PAN-90806. Phase II. Pan Optica
PAN-90806 [Figure 3(b)] is a formulation containing a very potent TKI drug, which displays an VEGFR IC50 of 11 nm. This affinity is in the same order of magnitude than the displayed by VEGF (IC50 = 6 nM). 48 Preclinical data showed that retinal concentrations achieved after administration of PAN-90806 were suitable to decrease leakage and bleeding from choroidal neovascular membranes, producing a comparable effect with the observed with intravitreal ranibizumab. 49 One of the main characteristics of this system is that it is formulated as a topical eye-drop suspension, which could enhance patient adherence and compliance. Results of the phase I/II trials showed that 51% of patients with wet AMD who applied once daily for 12 weeks eye drops of PAN-90806 did not need a rescue injection during trial or 1 month post-treatment.34,50
OTX-TKI. Phase I. Ocular therapeutix
This formulation is based on axitinib [Figure 3(c)], a TKI drug that block VEGFR-1, VEGFR-2, VEGFR-3, and the platelet-derived growth factor receptors. OTX-TKI is formulated as a bioresorbable intracameral implant composed of a polyethylene glycol–based hydrogel fiber, wherein drug microcrystals are homogeneously dispersed. This configuration permits to achieve long-lasting release of axitinib because drug delivery is limited by diffusion from the gel and dissolution of the microcrystals. 51 A phase I trial is ongoing testing drug doses of 200, 400, and 600 µg, with preliminary favorable results.38,52

Molecular structure of TKI salts used in the formulation of (a) GB 102; (b) PAN-90806; (c) OTX-TKI. Counterions are not depicted for clarity.
Non-antiedematous systems
Therapies found in this category target mechanisms not primary related to the VEGF/VEGFR pathway. These developments are based on compelling evidence connecting the onset and severity of neovascularization with preceding and/or concomitant processes involving oxidative stress and inflammation. 53 For instance, patients with diabetic macular edema (DME) have shown elevated concentrations of different pro-angiogenic factors besides VEGF-A (e.g. Ang2, erythropoietin, and soluble matrix metalloproteinase-2 and soluble matrix metalloproteinase-9), but also inflammation molecules [e.g. interleukin-37 (IL-37), IL-1β, IL-6, IL-8, IL-10, IL-18, tumor necrosis factor-α, inflammasomes] and lymphangiogenic factors (i.e. VEGF-C and VEGF-D).54,55 These set of therapies not only represent an option to current anti-VEGF therapies, but also these could be an important option for nonresponsive patients. 56 The chemical structure of some molecules found in this category is depicted in Figure 4.
Chemical diagrams of small molecules found in (a) AKS4290; (b) HCB1019; (c) AR-13503.
Luminate® – Risuteganib. Phase II. Allegro/Senju/Hanmi
Risuteganib is a synthetic oligopeptide that regulates integrins. These are membrane receptors that enable cell–cell and cell–extracellular matrix adhesion. Some integrins (e.g. αvβ3, αvβ5, and α5β1), however, has been associated with pathological neovascularization. Detrimental changes on integrins have been attributed to mitochondrial mutations triggered by oxidative stress. 57 Preclinical studies showed that intravitreal administration of risuteganib protected retinal cells against cytotoxic promoters. The mechanism of action of risuteganib is still under discussion, but it is plausible that this molecule upregulates the mitochondrial metabolic/redox function and activation of oxidases. 57 Trials on risuteganib showed a decrease in the expression of several integrins associated with retinal diseases.44,57 The protecting mechanism of risuteganib highlights the relevance of oxidative stress on retinal disfunctions, in particular because the retinal pigment epithelium (RPE) cells contain a large mitochondria number to meet the RPE energetic needs. 58 A phase II clinical trial in comparison with BCZ for the treatment of diabetic macular edema has been concluded. 59
ICON-1. Phase II. Roche/Iconic
Tissue Factor (TF) is expressed in pathological angiogenesis and in macrophage-associated human diseases, but not expressed in normal vasculature. Hence, overexpression of TF is a specific and accessible target for diseases featuring angiogenesis.60,61 ICON-1 is a chimeric antibody-like homodimer of 210 kDa formed by the crystallizable region of an immunoglobulin G1 conjugated with the factor VII (the natural ligand of TF). Given this configuration, ICON-1 displays a higher ligand affinity than other anti-TF antibodies (up to 1 pM versus 1 nM, respectively). Clinical results showed that intravitreal administration of ICON-1 in combination with ranibizumab provided significant improvements for proliferative AMD, which could enable a more durable improvement following anti-VEGF administration.62,63
AKST4290. Phase II. Alkahest
C-C chemokine receptor type 3 (CCR3) is normally found on the surface of certain immune cells, such as eosinophils, basophils, and Th2 lymphocytes. Its ligand, termed eotaxin, is an immunomodulatory chemokine overexpressed in different age-related diseases, such as wet AMD. The formation of the CCR3–eotaxin complex increases the permeability and degradation of the vascularity, recruits immune cells, and disturbs the homeostasis regulation. 64 AKST4290 is a system based on lazucirnon, a small molecule with affinity toward CCR3. Therefore, its administration creates a competitive interaction toward CCR3, which inhibits the formation of eotaxin–CCR3 complex. This has shown to reduce eosinophils accumulation and eosinophil-mediated tissue damage. One advantage of this therapy is that it is intended for oral administration. Preclinical data showed that choroidal neovascularization was inhibited more efficiently with lazucirnon than with anti-VEGF molecules tested. 65 This observation highlighted its potential toward proliferative AMD. Further studies are expected to provide greater insights on the mechanism of action and efficacy. 53 Phase II clinical trials have been performed in patients with wet AMD refractory to anti-VEGF therapy, showing promising results.66,67
AR-13503. Phase I. Aerie pharmaceuticals
AR-13503 is a formulation based on the active form of netarsudil, the last a pro-drug with anti-glaucomatous activity. AR-13503 targets the upregulation of the Rho/Rho kinase (ROCK) pathway, which can be mediated by VEGF-A. ROCK pathway is involved in different angiogenic processes, including changes in permeability, migration of endothelial cells, and survival. Furthermore, the ROCK pathway has shown to be a key factor in the angiogenesis of wet AMD and DR.8,68 AR-13503 is designed as a biodegradable sustained-release implant that undergoes hydrolysis and/or enzymatic degradation. This enables a zero-order release over a period of 4–6 months. 69 It is administered intravitreally in 10.6 μg doses throughout a single-use applicator.8,68 Phase I trial (NCT03835884) in patients with wet AMD and diabetic macular edema is undergoing.
HCB1019. InflammX therapeutics
HCB1019 treatment targets connexin 43 (Cx43), a hemichannel which is ubiquitously found on the membrane of different cells lines. Cx43 is an important protein of gap junctions and highly important for the normal physiological function of the cell. However, in pathological conditions, Cx43 can increase the secretion of proinflammatory cytokines from inflammatory cells. Inhibition of the Cx43 opening has shown to reduce inflammatory conditions, especially those involving the inflammasome pathway.70,71 HCB-1019 is based on tonabersat, a compound initially studied as an anti-migraine agent. Therefore, there is compelling evidence on this repurposed drug in terms of safety. 72 One of the most significant advantages of this system is that it is orally administered, displaying a suitable pharmacokinetic profile and tolerability by patients.72,73
Gene therapy
Gene therapy could represent the ultimate form of sustained release of anti-VEGF molecules to tackle angiogenesis. Gene therapy aims to transfer one or more therapeutic nucleic acids to a patient’s cells or correcting a defective gene. 74 Early stages of clinical gene therapy sought to establish safety and experience in patients. Immune responses and insertional mutagenesis were major concerns. 75 The goal of these therapies in the field of proliferative retinopathies is to modify genes in retina to induce an endogenous and in situ anti-VEGF secretion.76,77 If successful, this would decrease the need of continuous intravitreal injections, which is one of the main disadvantages of most anti-VEGF therapies.
RGX 314. Phase II. RegenXbio
This system utilizes an adeno-associated virus (AAV8), a small nonpathogenic viral vector designed to transfect retinal cells. Successful transfection induces the in situ production of a soluble monoclonal antibody fragment similar to ranibizumab. 78 RGX-314 has been tested as a single-dose subretinal injection via pars plana vitrectomy. Preclinical studies showed promising results, and clinical trials to assess safety and tolerability are undergoing.41,77,79
ADVM-022 (AAV2.7 m8-aflibercep). Phase II. Adverum biotechnologies
This system utilizes a recombinant AAV optimized to induce the expression of aflibercept (see Table 1). 80 ADVM-022 uses the AAV2.7 m8 capsid, which has been engineered from AAV2 to induce an efficient retinal transduction following intravitreal administration. Preclinical studies in a nonhuman primate model showed that ADVM-22 could induce the production of aflibercept in equivalent amounts to the observed 56 days after the administration of one single intravitreal dose of aflibercept. 81 Phase I study has been completed (NCT04418427) and two phase II clinical trials are ongoing (NCT04418427, NCT05536973).80,82
HMR59 or AAVCAGsCD59. Phase I. Hemera biosciences
AAVCAGsCD59 (HMR59) aims to avoid the formation of the membrane attack complex (MAC), which induces apoptosis of retinal cells. HMR59 uses a recombinant adeno-associated virus serotype 2 vector to induce the expression of a human CD59 protein. 83 The transfected CD59 protein interacts with the C8 and C9 components of nascent MAC, which prevents that the endogenous C9 protein can bind with the aforementioned to form the MAC complex. Consequently, the complement-mediated cell lysis is inhibited. 84 Phase 1 study to assess efficacy and safety of two doses of HMR59 has been completed.83,85
OXB201. Phase I. Oxford biomedica
OXB201 was developed to transfect two genes that encode for endostatin and angiostatin. At preclinical stage, these proteins showed to suppress blood vessel growth and leakage. Results from clinical trials, however, showed that despite an apparent reduction in fluorescein angiographic leakage, only one subject showed convincing evidence of antiangiogenic activity.77,86
Potential impact of upcoming therapies
Uncontrolled angiogenesis as a highly deteriorative condition for retina. Although anti-VEGFs have shown to be successful to halt neovascularization, they face issues such as a lack of vision improvements for many patients, and that the long-term use of anti-VEGF therapy is associated with adverse events. Therefore, there is a current need to develop efficient strategies that reduce or eliminate ocular injections. Therapies described herein were limited to results obtained using a software-based IA analysis and individual searches in databases. Results were also limited to therapies currently found in clinical trials. Analysis indicates that developments follow three main strategies: (a) increasing the efficacy of anti-VEGF therapy, (b) inhibiting pharmacological pathways related to oxidative stress and inflammation, and (c) inducing the in situ production of anti-VEGF molecules to avoid the need of reinjection. Strategy 1 is being addressed with new anti-VEGF molecules with targets beyond VEGF-A, by increasing the intravitreal residence time to produce long-lasting effects, or by targeting VEGF receptor. Strategy 2 seems promising not only because drugs in this classification have shown to be efficient, but also because they could be used in patients who do not respond to the conventional anti-VEGF therapies, or for patients in early and mid-stage of disease development. One of the main highlights is that some of these therapies avoid the intravitreal pathway, which could enhance patient compliance. Strategy 3 is addressed through gene therapy. This has a lot of potential, but there are several obstacles that it needs to overcome. If successful, this platform could, however, improve clinical outcomes while reducing treatment burden.
Conclusions
The analysis performed herein described the mechanism of action of anti-antiangiogenic therapies in clinical development. A significant set of these novel therapies target the angiogenic cascade driven by the VEGF. This strategy is being addressed with novel anti-VEGF aiming long-lasting effects. Another significant area of development targets non-VEGF pathways. These set of therapies not only display efficacy but could represent a primary alternative for patients nonresponsive to available anti-VEGF compounds and, in some cases, without the burden of intraocular administrations. Finally, gene therapy can potentially improve clinical outcomes while drastically reducing treatment burden. These therapies, however, need to demonstrate safety and efficacy. In summary, the diverse mechanism of action of upcoming therapies is likely to increase the current portfolio for treating proliferative retinopathies, providing significant benefits for patients and clinicians.