
Abstract
Purpose:
A large number of systemic reviews and meta-analyses have explored the relationship between nonalcoholic fatty liver disease (NAFLD) and multiple health outcomes. The aim of this study is to conduct an umbrella review to assess the strength and evidence for the association between NAFLD and health outcomes.
Methods:
We systematically identified the present meta-analyses of observational studies reporting an association between NAFLD and health outcomes. For each meta-analysis, we assessed the quality with AMSTAR2 and graded the epidemiologic evidence.
Results:
Fifty-four articles comprising 111 unique meta-analyses were included in this study. Eighty-five unique outcomes showed significant associations (P ← 0.05), whereas 26 unique outcomes showed insignificant associations, and we cannot assess the epidemiologic evidence. For 85 significant health outcomes, four outcomes (carotid intima-media thickness (C-IMT), peak A velocity, left ventricle end-diastolic diameter, incident chronic kidney disease (CKD) in adult patients) was graded as high quality of evidence, 23 outcomes were graded as the moderate quality of evidence, and the remaining 58 outcomes were graded as weak quality of evidence. Fourty-seven (87.03%) studies showed critically low methodological quality.
Conclusion:
In this umbrella review, only four statistically significant health outcomes showed high epidemiologic evidence. NAFLD seems to relate to an increased risk of C-IMT, peak A velocity, left ventricle end-diastolic diameter, and incident CKD in adult patients.
Introduction
The global prevalence of nonalcoholic fatty liver disease (NAFLD) has only been increasing in the population and suspect to increase in the future leading to increase global burden. NAFLD affects up to 25% of adults, up to 3~10% of the Western pediatric population and increases up to 70% among obese children. 1 Many research studies have demonstrated how NAFLD can contribute to several disease processes including hepatic, extrahepatic diseases, and overall increase in mortality.2,3 It is becoming the most common and major cause of chronic liver disease worldwide, especially in high-income countries, resulting in considerable liver-related disease such as hepatocellular carcinoma (HCC), 4 cryptogenic liver cirrhosis, 5 and liver-specific mortality. 6 It is also a major cause of extrahepatic disease with earlier studies demonstrating that NAFLD also contributed to the risk of cardiovascular diseases7,8 and diabetes. 9 The risk factors for cardiovascular diseases and diabetes are also known for metabolic syndrome. According to Lonardo et al., 10 NAFLD is not only a manifestation but also a precursor of the metabolic syndrome. In recent research studies, there has been further investigation regarding NAFLD association with other diseases. A great number of studies and meta-analyses have demonstrated that NAFLD may increase the risk of various diseases, including gastrointestinal diseases,11–13 chronic kidney diseases (CKD),14,15 atrial fibrillation, 16 and all-cause and cause-specific mortality, 17 indicating that NAFLD poses a threat to human health.
Although multiple investigations explored the correlation between NAFLD and other health outcomes, the reported associations may be flawed. The magnitudes of the observed effects are affected by inherent biases such as selective bias, publication bias, and residual confounding.18,19 Despite many systematic reviews and meta-analyses that have examined NAFLD and other health outcomes, to our knowledge, there have been no systematic efforts to accurately summarize and critically appraise the evidence. Umbrella review is increasingly more important for overviewing the evidence of systematic and meta-analyses on a specific topic. An umbrella review focused on a specific disease that can provide important guidance and reliable evidence for prevention, diagnosis, and treatment. We performed an umbrella review of observational meta-analyses to comprehensively assess methodological quality, investigate potential bias, and evaluate the epidemiologic evidence of the associations between NAFLD and health information. We believe that this work can provide useful information about NAFLD and human health.
Materials and methods
We followed Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) protocols to research literature systematically. 20 Before beginning the umbrella review, we registered the protocol with PROSPERO (registration number: CRD42021279078).
Literature search
PubMed, Web of Science, and Cochrane Database of Systematic Reviews were searched from the initiation to September 2021. The search terms applied were (‘Meta-Analysis’ OR ‘metaanaly’ OR ‘meta-analy’ OR ‘Systematic review’ OR ‘systematic review’ AND ‘Nonalcoholic Fatty Liver Disease’ OR ‘NAFLD’ OR ‘Nonalcoholic Fatty Liver Disease’ OR ‘Fatty Liver, Nonalcoholic’ OR ‘Fatty Livers, Nonalcoholic’ OR ‘Liver, Nonalcoholic Fatty’ OR ‘Livers, Nonalcoholic Fatty’ OR ‘Nonalcoholic Fatty Live’ OR ‘Nonalcoholic Fatty Livers’ OR ‘Nonalcoholic Steatohepatitis’ OR ‘Nonalcoholic Steatohepatitides’ OR ‘Steatohepatitides, Nonalcoholic’ OR ‘Steatohepatitis, Nonalcoholic’). We also manually screened the reference to identify the eligible articles. LZ and WC independently conducted the literature search. Any discrepancies were discussed and resolved with ST.
Selection criteria
Two authors (LZ and CW) scrutinized independently the full texts of potentially eligible articles. Only the meta-analyses of the epidemiological studies examining the relationship between NAFLD and other health outcomes in humans were considered. Trials and meta-analyses of interventional trials were not available for our study. The protocols, abstracts of the conference, and letters to editors were also excluded. When several meta-analyses simultaneously reported the same health outcome, we included the one with the largest number of studies.
Data extraction
The data of included studies were extracted by two authors separately. For each eligible meta-analysis, we extracted the following information: the first author, publication year, the design of studies, the number of participants and cases, the effects sizes (SMD, WMD, MD, ORs, RRs, or HRs), the p values of pooled effects, Cochrane Q measurement, Egger ‘s test measurement and I 2 . When we met discrepancies, we resolved them through discussion.
Assessment of methodological quality
Two authors used AMSTAR 2, 21 which consists of 16 items, to assess the methodologic quality of each included meta-analysis independently. AMSTAR 2 is a strict and reliable measurement tool to evaluate the quality of systematic reviews and meta-analyses. According to the AMSTAR 2 scores, four grades (high, moderate, low, and critically low) were categorized to describe the result of methodologic quality. No or only one non-critical defect is considered high methodologic quality and more than one non-critical defect is considered moderate methodologic quality. Only one critical weakness with or without non-critical defects is considered low method quality and more than one critical weakness with or without critical defects is considered critically low methodologic quality. Discrepancies between AMSTAR 2 scores were resolved by discussion.
Evaluation of the evidence quality
We classified the evidence from meta-analyses of observational studies with the parameters that have been applied in various fields.22–26 The parameters consist of the following criteria: (1) precision of the estimate (p value for the estimate ← 0.00127,28 and the number of cases ⩾1000; (2) no heterogeneity (I 2 ← 50% and p value for Cochran Q-test > 0.10); (3) no evidence of small-study effects (p value for Egger’s test > 0.10). The strength of epidemiologic evidence was categorized into high (if all these criteria were satisfied), moderate (if p value for estimate ← 0.001 with a maximum of 1 criterion was not satisfied), or weak (p value for estimate ← 0.05 with all other cases). If the p value for estimate > 0.05, the evaluation of evidence quality was not applicable.
Data analysis
According to the extracted raw data from each published study, we recalculated the missing data (ig. heterogeneity and publication bias) with a random-effects model whenever possible. When the p value was←0.05, the total impacts of pooled meta-analyses were considered significant. I 2 test and Q test were used to evaluate the heterogeneity between studies and publication bias was calculated by Egger’s test. The p value ← 0.1 for heterogeneity and publication bias were both considered significant.
Results
Characteristics of the meta-analyses
The results of systematic research and selection of eligible meta-analyses are summarized in Figure 1. Overall, a total of 2200 research articles were investigated from PubMed (n = 1295), Web of Science (n = 862), and Cochrane database (n = 43). After excluding the 17 articles and 53 overlapping meta-analyses (Supplementary Table 1), 54 articles with 111 unique health outcomes were included29–82 (Table 1). The publication dates of these studies range from 2013 through 2021. Among the meta-analyses included in our umbrella review, the median number of primary studies was 7 (range: 2–30), the medium number of participants was 19,274 (range: 146–613,715) and the median number of cases was 1444 (range: 44–36,448). As we see in Figure 2, health outcomes associated with NAFLD relate to the following categories of diseases: cardiovascular disorders (n = 36), cerebral and cerebrovascular disease (n = 5), skeletal system disorders (n = 9), mortality (n = 8), metabolic disorders (n = 3), digestive disorders (n = 20), nephrological disorders (n = 3), urological disorders (n = 2), serum marker disorders (n = 10), respiratory system disorders (n = 3), and other health outcomes (n = 12) (Figure 2). Among 111 unique meta-analyses, 85 (76.58%) reported significant summary outcomes (p ← 0.05) and the remaining 26 (23.42%) meta-analyses showed no significant association with NAFLD. According to the statistically significant outcomes, it can be concluded that NAFLD may increase the risk of a wide variety of diseases and have harmful effects on human health.

The PRISMA consort flow diagram of literature search and study selection.
Characteristics of the unique meta-analyses investigating the associations between NAFLD and multiple health outcomes.

C-IMT, carotid intima-media thickness; US, ultrasound; CT, computed tomography; FLI, fatty liver index; HIS, hepatic steatosis index; ICD, International Classification of Diseases; LAI, liver attenuation index; CNS, comprehensive NAFLD score; LFS, liver fat score; NFS, NAFLD fibrosis score; MRI, magnetic resonance imaging; CAC, coronary artery calcification; CVD, cardiovascular disease; CAD, coronary artery disease; LEVF, left ventricular ejection fraction; E/e’ ratio, early mitral velocity/early diastolic tissue velocity; E/A ratio, early mitral velocity/late mitral velocity ratio; BSA, body surface area; EFT, epicardial fat tissue; GLS, global longitudinal strain; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ECC, extrahepatic cholangiocarcinoma, IP, intestinal permeability; AP, acute pancreatitis, BMD, bone mineral density; ACM, all-cause mortality; T2D, type-2 diabetes; CKD, chronic kidneys disease; MPV, mean platelet volume; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; ICU, intensive care unit; PWV, posterior wall velocity; NR, not reported.
The result was reanalyzed.
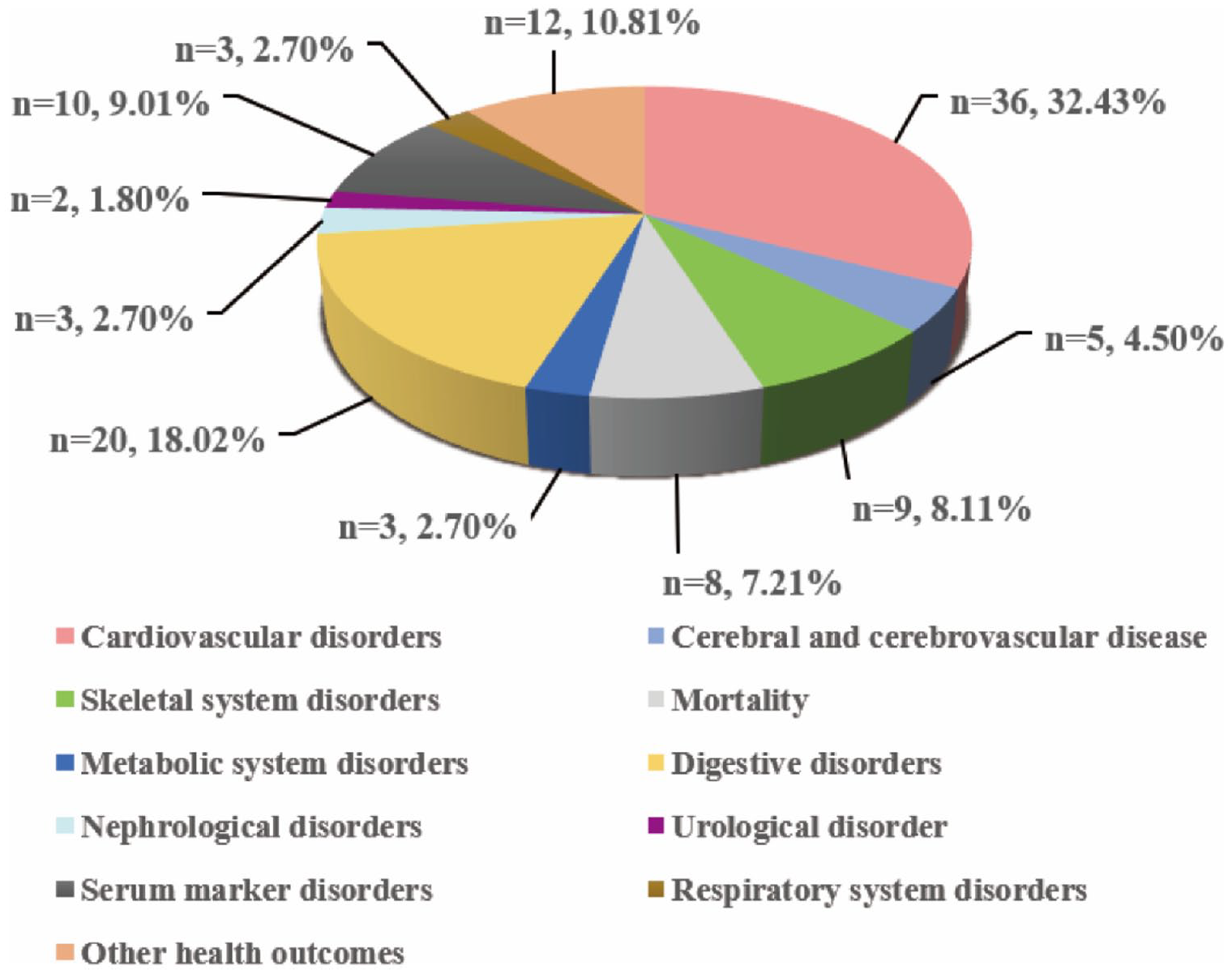
Map of achievements associated with NAFLD.
Heterogeneity
According to Table 1, we recalculated the two results of two articles34,44 because they did not report the outcomes of heterogeneity. However, owing to the lack of raw data in one article, 46 we failed to recalculate the I 2 and the p value for the Cochran Q-test by random or fixed model, so the heterogeneity was not able to be evaluated. Among the 111 unique meta-analyses, only 26 (23.42%) health outcomes indicated no heterogeneity (I 2 ← 50% and p value for Cochran Q-test ⩾ 0.1), whereas 85 (76.58%) health outcomes showed significant heterogeneity (I 2 ⩾ 50% and p value for Cochran Q-test ← 0.1).
Publication bias
Fifty-three outcomes were recalculated using the Egger’s test through which the raw data in each included meta-analysis to evaluate for potential publication bias. Due to the small number of studies, there were still 21 outcomes in 15 articles that could not be recalculated using the Egger’s test,32,40,49,57–59,61,65,67,70–72,74,76,79 thus we were not able to assess their publication bias. In the end, 71 health outcomes had no publication bias (p value for Egger’s test ⩾ 0.1) while 19 health outcomes presented publication bias (p value for Egger’s test ← 0.1).
Methodological Quality Assessment
The 16 items including in AMSTAR 2 and the result of the methodological qualities assessment of the 54 included articles are presented in Table 2. Only 7 (12.96%) articles were assessed to be low methodological quality, and the remaining 47 (87.04%) articles were assessed to be critically low (Figure 3). It is worthy to note that there were no high/moderate methodological quality based on the AMSTAR 2 criteria. The major critical flaws were the absence of registered protocol (n = 40, 75.47%), the inadequacy of the literature search (n = 52, 96.30%) and without the list for excluding primary studies (n = 39, 72.22%).
Assessments of AMSTAR2 scores.

AMSTAR 2 checklist (items in italic are considered critical):
1, PICO description; 2, protocol registered before the commencement of the review; 3, study design included in the review; 4, adequacy of the literature search; 5, two authors study selection; 6, two authors study extraction; 7, list for excluding individual studies; 8, included studies descripted in detail; 9, risk of bias for the single studies that included in the review; 10, source of funding of primary studies; 11, appropriateness of meta-analytical methods; 12, impact of risk of bias of single studies on the results of the meta-analysis; 13, consideration of risk of bias when interpreting the results of the review; 14 explanation and discussion of the heterogeneity observed; 15, assessment of presence and likely impact of publication bias; 16, funding sources and conflict of interest declared.
Abbreviations: Y, yes; PY, partial yes; N, no.
No 2, 4, 7, 9, 11, 13, and 15 are the critical items.

Map of results of AMSTAR 2.
Strength of epidemiologic evidence
The results of epidemiologic evidence are shown in Table 3. According to the criteria mentioned above, the assessment of epidemiologic evidence was not applicable for 26 (23.42%) health outcomes because their p value for pooled effects were more than 0.05 which was not statistically significant. The relevant criteria were considered to be not satisfied if a meta-analysis lacked the result of heterogeneity and publication bias. Among the remaining 85 statistically significant health outcomes, only 4 (3.60%) outcomes were rated as high epidemiologic evidence, 23 (20.72%) outcomes showed moderate epidemiologic evidence, and 58 (52.25%) outcomes were graded as weak epidemiologic evidence (Figure 4).
The strength of epidemiologic evidence of 111 unique health outcomes.

C-IMT, carotid intima-media thickness; CAC, coronary artery calcification; CVD, cardiovascular disease; CAD, coronary artery disease; LEVF, left ventricular ejection fraction; E/e’ ratio, early mitral velocity/early diastolic tissue velocity; E/A ratio, early mitral velocity/late mitral velocity ratio; BSA, body surface area; EFT, epicardial fat tissue; GLS, global longitudinal strain; HCC, hepatocellular carcinoma; ICC, intrahepatic cholangiocarcinoma; ECC, extrahepatic cholangiocarcinoma, IP, intestinal permeability; AP, acute pancreatitis, BMD, bone mineral density; ACM, all-cause mortality; T2D, type-2 diabetes; CKD, chronic kidneys disease; MPV, mean platelet volume; FEV1, forced expiratory volume in the first second; FVC, forced vital capacity; ICU, intensive care unit; PWV, posterior wall velocity.
Note. The strength of epidemiologic evidence was rated as follows:
High, if all criteria were satisfied: precision of the estimate (p < .001 and >1000 disease cases), consistency of results (I 2 < 50% and Cochran Q-test p > .10), and no evidence of small-study effects (p > .10).
Moderate, if a maximum of 1 criterion was not satisfied and a p < .001 was found.
Weak, in other cases (p < .05).
NA, p values are greater than 0.05, so the epidemiologic quality of these meta cannot be rated.

Map of results of evidence assessment.
Discussion
Main findings and interpretation
Our umbrella review provides a comprehensive overview of the association between NAFLD and other health outcomes based on the existing evidence from identified 54 observational studies with 111 unique outcomes. We also critically evaluated the strength of evidence for all these associations with the criteria broadly applied to assess the epidemiologic evidence in the various field22–26 and the quality of methodology of each publication, including in the current review. We found that NALFD increased the risk of 85 health outcomes that contained cardiovascular disorders, cerebral and cerebrovascular disorders, digestive disorders, nephrological disorders, urological disorders, metabolic disorders, mortality, skeletal system disorders, serum marker disorders, respiratory system disorders, and other health outcomes. However, 26 health outcomes had no relationship with NALFD and could not be assessed the epidemiologic evidence in this study. Only four outcomes (carotid intimal medial thickness (C-IMT), peak A velocity, left ventricle end-diastolic diameter (LVEDD), and incident CKD in adult patients) showed high epidemiologic evidence. The 81 remaining associations were either rated as moderate epidemiologic evidence or weak epidemiologic evidence. Heterogeneity and small-study effects were the two main reasons for the evidence rating downgrade in our study.
NAFLD increased C-IMT which is considered as a marker of subclinical atherosclerosis with high epidemiologic evidence in the review. The potential mechanism seems to relate to high oxidative stress caused by steatosis-stimulated fatty-acid oxidation in the liver, increased insulin resistance, and macrophage activation.7,83,84 Through early detection and intervention, subclinical atherosclerosis can be controlled and even reversed. 85 Therefore, for NAFLD, it is important to identify the C-IMT earlier. The cardiac function and structure were also damaged by NAFLD. We demonstrated the association between NAFLD and peak A velocity and LVEDD was both graded as high. In NAFLD patients, the role of pro-inflammatory cytokines, insulin resistance, and dyslipidemia acts together on the cardiac metabolism and function,86–88 which directly causes the impairment on the heart.
In 2020, a large database analysis in Germany, comprised of 48,057 patients with NAFLD and 48,057 patients without NAFLD, supported that NAFLD constitutes an independent risk factor for CKD. 89 Similarly, in our umbrella review, the incidence of CKD was also increased by NAFLD with high epidemiologic evidence. There exists a common pro-inflammatory and profibrotic mechanism of disease progression in both NAFLD and CKD; furthermore, kidney-liver crosstalk also appears in NAFLD. 89 In addition to insulin resistance, pro-inflammatory factors, oxidative stress, the rein-angiotensin-aldosterone system also plays a role in the pathogenesis.90–92
We noted that no study included in this umbrella review showed high/moderate methodologic evidence and only seven studies showed low methodological quality according to AMSTAR 2 criteria. The most critical flaws were the absence of registered protocol, the literature search’s inadequacy, and the list for excluding individual studies. Eighty-five outcomes showed remarkable heterogeneity between studies. We concluded that this may be caused by several factors such as NAFLD severity, sex, the diagnosis of NAFLD, the study design, and body mass index, resulting in unreliable results. Among 111 health outcomes, 19 outcomes presented publication bias detected by Egger’s test. The main reason for publication bias is that positive results are easier to publish than negative results, leading to incomplete literature included in the meta-analysis. Another common reason is that the study sample size is too small.
Strength and limitations
Our umbrella review had several strengths. To our knowledge, it is the first umbrella review of observational meta-analysis and provides a comprehensive overview of the associations of NAFLD and health outcomes. A strong search strategy and data extraction were performed by two authors independently which made the result more reliable. Furthermore, we used validated AMSTR 2 tool to evaluate the methodological quality in our umbrella review.
However, several limitations should be considered in the interpretation of our umbrella review. We did not evaluate the quality of the primary studies because it was beyond the scope of the current umbrella review. We conducted the review based on the published meta-analyses with the largest number of studies at present, and we might have missed some individual studies, which could have an influence on the results. In this umbrella review, 21 health outcomes publication bias could not be assessed due to the limited number of primary studies (less than two) and missing data which indicates unreliable results. Thus, more research is needed to investigate these associations that were based on small number of included studies.
Another limitation to consider is that we could not conduct the subgroup analysis in this study (eg. sex differences, pre-menopausal, and post-menopausal women) owing to lack of raw data. As comprehension evolves, sex differences, and menopausal status are increasingly apparent in the prevalence, risk factors, progression, and outcomes in NAFLD. Numerous studies have indicated compare to women, men have higher risk and prevalence of NAFLD.93,94 But the prevalence of NAFLD is equal in men and post-menopausal women. 95 A meta-analysis pointed out that after age 50, women have a higher risk of developing advanced fibrosis than men. 96 However, several studies have shown that women have a higher incidence of NAFLD in early menarche and a higher risk of NASH and advanced fibrosis.97,98 Almost all of the included meta-analyses did not distinguish between sex, pre-menopausal, and post-menopausal women in the included participants, which made it difficult to re-analyze the results according to the sex difference and menopausal status. However, we recognize the importance of sex difference and menopausal status and will focus on this aspect in future studies.
Conclusion
In summary, 54 studies explored 111 unique health outcomes; only four outcomes showed high epidemiologic evidence with statistical significance. NAFLD may be related to the increased risk of C-MIT, peak A velocity, LVEDD, and incident CKD in adult patients. However, more robust studies and investigations are needed to achieve high epidemiologic evidence for the associations between NAFLD and health outcomes.
Supplemental Material
sj-docx-1-taj-10.1177_20406223221083508 – Supplemental material for Nonalcoholic fatty liver disease and health outcomes: An umbrella review of systematic reviews and meta-analyses
Supplemental material, sj-docx-1-taj-10.1177_20406223221083508 for Nonalcoholic fatty liver disease and health outcomes: An umbrella review of systematic reviews and meta-analyses by Lixian Zhong, Chutian Wu, Yuting Li, Qiuting Zeng, Leizhen Lai, Sisi Chen and Shaohui Tang in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
The authors would like to acknowledge all authors of the original studies that were included in this meta-analysis.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent statement and ethical approval
Consent statement and ethical approval are not required as the current study does not involve human participants and animal subjects.
Availability of data and material
The data used to support the findings of this study are included within the article. The primary data used to support the findings of this study are available from the corresponding author upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.