
Abstract
Fucoidan is a marine polysaccharide. In recent years, fucoidan has attracted wide-scale attention from the pharmaceutical industries due to its diverse biological activities such as lipid-lowering, anti-atherosclerosis, and anticoagulation. This review clarifies the pharmacological effects of fucoidan in the treatment of human cardiovascular and cerebrovascular diseases. Fucoidan exerts a hypolipidemic effect by increasing the reverse transport of cholesterol, inhibiting lipid synthesis, reducing lipid accumulation, and increasing lipid metabolism. Inflammation, anti-oxidation, and so on have a regulatory effect in the process of atherosclerosis endothelial cells, macrophages, smooth muscle cells, and so on; fucoidan can not only prevent thrombosis through anticoagulation and regulate platelet activation, but also promote the dissolution of formed thrombi. Fucoidan has a neuroprotective effect, and also has a positive effect on the prognosis of the cardiovascular and cerebrovascular. The prospects of applying fucoidan in cardio-cerebrovascular diseases are reviewed to provide some theoretical bases and inspirations for its full-scale development and utilization.
Introduction
Cardiovascular disease (CVD) is a category of diseases related to the circulatory system, including atherosclerosis (AS), hypertension, hyperlipidemia, and thrombosis. In the past decade, the global number of deaths from CVD has increased by 12.5%, and reportedly, CVD has already become the leading cause of human deaths worldwide.1,2 The incidence of CVD is also increasing year by year in China. 3 One of the most important pathological bases of CVD is AS, which is usually caused by endothelial dysfunction due to an imbalance in lipid metabolism and the accumulation of monocytes under the endothelium. Monocyte-derived macrophages cannot effectively reduce the inflammatory response and eventually lead to the formation of atherosclerotic plaques. 4 Statins are mainly used to reduce the levels of very-low-density lipoprotein cholesterol and low-density lipoprotein (LDL) cholesterol caused by the lipid metabolism imbalance. 5 The current guidelines for the management of dyslipidemia recommend statins as the first choice for patients with high fat [triglycerides (TG) ⩾ 2.3 mmol/L] complicated with a high risk of CVD. However, the side effects of statins, such as myalgia, myositis, rhabdomyolysis, 6 and liver injury, cannot be ignored, and it may increase the risk of hemorrhagic stroke in patients with cerebrovascular disease. 7 Therefore, it is necessary to develop new bioactive substances. The marine biome contains highly valuable natural resources, and marine polysaccharides have a variety of biological activities. The biological activity of fucoidan and its potential applications are of particular interest.
Fucoidan, an intercellular polysaccharide inherent in brown algae, such as edible kelp, is a polysaccharide composed of L-fucose and sulfate groups and different proportions of galactose, rhamnose, xylose, and mannose.6,8,9 Fucoidan is found in the cell wall of brown algae as well as some marine invertebrate tissues.10,11 The chemical structure of fucoidan varies greatly with alga species, location of origin, harvest season, extraction method, and so on, 12 and the molecular weight ranges from tens of thousands to hundreds of thousands of Daltons. 13 Fucoidans have two major types of molecular skeleton (Figure 1). The first, type I, consists of (1-3)-connected or (1-4)-connected L-fucose residues, with sulfate groups located on the fucose residues C-2 and C-4. The second, type II, contains alternately repeated (1-3)- and (1-4)-linked L-fucose.14,15 The skeletal and monosaccharide composition, the content and location of the sulfate groups, and the molecular weight of fucoidan all affect its biological activity. 16

Two main skeletal structures of fucoidan (simplified). (a) The structure of type I fucoidan is composed of repeated (1-3)-linked α-L-fucose. (b) The structure of type II fucoidan is composed of alternating (1-3)- and (1-4)-linked α-L-fucose. ‘R’ can be a monosaccharide or sulfuric acid group. 17
Fucoidan was first discovered in 1913, and more recently, it is attracting an increasing amount of attention and is beginning to appear in significantly more research articles. 18 Fucoidan has a variety of biological activities, such as anti-tumor, 13 hypolipidemic, 19 anticoagulant, 20 anti-inflammatory, 21 antiviral, 22 and other biological effects. Fucoidan can reduce inflammatory reactions and P-selectin expression, maintain the integrity of the glomerular basement membrane and glomerular structure, improve spherical filtration function, protect against the abnormal degradation of renal glycosyl ribose, and inhibit renal fibrosis and glomerular sclerosis by reducing the accumulation of the extracellular matrix. 23 Fucoidan brings great impetus to the immune system by enhancing phagocytosis. In clinical and animal studies, fucoidan has been demonstrated to improve innate immunity and reduce inflammation. 24 In vitro and in vivo data have shown that the polysaccharide is effective against influenza viral infection, and specific inhibitory activity against novel coronavirus infection in vitro was demonstrated for fucoidan.15,17 Fucoidan can also protect mice from lipopolysaccharide-induced acute lung injury by regulating the GSK-3 β-Nrf2 signal pathway to inhibit inflammation and oxidation. 25
In recent years, the blood-lipid reduction, anti-atherosclerosis, and anti-thrombus effects of fucoidan have been widely investigated by researchers. However, there are much fewer systematic reports on the properties of fucoidan in relation to CVD. In this article, we review the progress of research into the use of fucoidan for the treatment of CVD in recent years, including its hypolipidemic, anti-atherosclerotic, and antithrombotic effects and mechanisms. The benefits of treating CVD patients with fucoidan are emphasized, and we provide some theoretical bases and inspiration for the development of cardiovascular drugs.
The hypolipidemic effects of fucoidan
In recent years, the incidence of hyperlipidemia has gradually increased and shown a growing prevalence in younger people. Hyperlipidemia is a large-scale metabolic disorder caused by various factors that increases the level of blood cholesterol or triglyceride, and it is a common public health problem. 26 Lipid abnormalities are accompanied by other metabolic changes that are closely related to the pathogenesis of AS. Long-term increase in blood lipids can easily cause cholesterol to invade the walls of large blood vessels, deposit and accumulate, and promote the proliferation of smooth muscle cells and fibroblasts in arterial leiomyoma. 27 Hyperlipidemia is a major risk factor for CVD such as atherosclerosis, coronary artery disease, and acute myocardial infarction, so effective medical treatment needs to be developed as soon as possible. 28 The research and development of lipid-lowering drugs is a field worthy of in-depth research. Fucoidan, as a natural active polysaccharide, has a variety of pharmacological activities, and its lipid-lowering effects have been widely discussed.
Increasing cholesterol reverse transport
Reverse cholesterol transport (RCT) plays an important role in AS. RCT is a physiological process that transports peripheral lipids to the liver through high-density lipoprotein (HDL) in the blood, decomposes and converts cholesterol in the liver, and then excretes the lipids in the small intestine.29,30 The dysfunction of RCT-related genes is the main cause of atherosclerotic lipid deposition, chronic inflammation, and foam cell formation, and has become the main target of anti-AS therapies. It was found that RCT is also a possible target of fucoidan. 31
Studies have shown that fucoidan can complete the outflow of intracellular free cholesterol by up-regulating SR-B1, LDLR, ABCG1, and ABCA1 expression in ApoE mice and phagocytizing and clearing the excess peripheral lipids via their transport to the liver by HDL, which is the first step of RCT. Peroxisome proliferation-activated receptor (PPAR) α and β are also key node proteins in cholesterol regulation. Fucoidan increases the amount of PPAR α and promotes the metabolism and efflux of cholesterol in the liver, while ABCA1 and ABCG8 decompose and metabolize the cholesterol transported to the liver. Levels of cholesterol 7-hydroxylase (CYP7A1) are also increased, which decomposes cholesterol into bile salts or bile acids.32,33 Cholesterol can also be reabsorbed by Niemann-pick C1-like 1 apolipoproteins in the brush border membrane of intestinal cells, transported to ABCG5/G8 membrane proteins, and finally excreted in vitro. 34 Fucoidan can reduce lipid levels by affecting the expression of genes and proteins related to the process of RCT to slow the progression of AS.
Inhibiting lipid synthesis
In addition to controlling lipid intake, .such as the maintenance of a healthy diet . Inhibiting lipid synthesis are also an important way to improve lipid metabolism. Sterol-regulated primary binding protein (SREBP)-2 regulates the expression of genes involved in cholesterol synthesis and uptake. SREBPs are cleaved and released as transport factors to bind to the gene operon of the LDL receptor (LDLR) or hydroxymethyl glutarate coenzyme A synthase. Fucoidan was found to reduce the expression of mature SREBP-2 protein, then decrease the expression of the HMG-CoA-R gene in the liver; hence, it is relatively specific to cholesterol synthesis. 35 In a study on different types of fucoidans, the down-regulation of SREBP-1 C was found to lead to a decrease in fatty acid synthesis. 36
Fucoidan extracted from Kjellmaniella crassifolia increased the protein levels of PPARα by approximately 17.01% in a hyperlipidemic rat model, and the protein levels of SREBP-1 decreased significantly by about 22.31%. The molecular mechanism by which fucoidan regulates hyperlipidemia is inhibiting cholesterol and fatty acid synthesis, accelerating mitochondrial β-oxidation or fatty acid peroxisome oxidative degradation in the body. 37
Some findings have suggested that fucoidan has a hypolipidemic effect equivalent to that of lovastatin, and the mechanism is related to an increase in lecithin cholesterol acyltransferase (LCAT) activity. 38 A fucoidan of Saccharina sculpera inhibits cholesterol synthesis by down-regulating HMG-CoA-R and up-regulating LCAT, thus reducing the levels of serum lipids in hyperlipidemic rats and effectively preventing lipid accumulation in the liver. 39 After treatment with fucoidan from an extract of Sargassum siliquosum, a brown, biological activity related to anti-adipogenesis and lipid synthesis decreased by 28.9% compared with the free-fatty-acid-induced control. 40
Therefore, fucoidan inhibits lipid synthesis by regulating the activity of sterol-regulated binding protein, lecithin cholesterol acyltransferase, and HMG-CoA synthase.
Reducing lipid accumulation
Elevated levels of serum total cholesterol (TC) and TG are important risk factors for CVD. When ApoE-gene-deleted mice fed a high-fat diet were given low-dose (50 mg/kg/day) or high-dose (200mg/kg/day) fucoidan, the lesion/lumen ratio decreased by 29.9% and 46.9%, respectively, and lipid deposition in the liver decreased by 35.5% and 59.3%, respectively, compared with the control group. 33 In addition, combination medication of fucoidan also had a hypolipidemic effect. When fucoidan from Japanese thick-leaf kelp and Undaria pinnatifida were, respectively, mixed with Hawthorn extract at a 1:1 ratio and intragastrically administered to hyperlipidemic rats, the levels of TC, TG, LDL-C, and the atherosclerotic index decreased significantly after 28 days. 41 Clinical trials have reported a similar effect, as LDL cholesterol levels were reduced in obese patients after 3 months of using fucoidan derived from Saccharomyces cerevisiae. 42 Thus, fucoidan improved atherosclerotic lesions and lipid distribution in a dose-dependent manner.
In vitro and in vivo studies have shown that fucoidan has an indirect effect on energy and lipid homeostasis by regulating fat absorption, thus reducing fat accumulation in the liver. 43 In a high-fat and high-sugar obese mouse model, sea cucumber fucoidan improved metabolic inflammation by inhibiting TLR4/NF-kappa b-dependent lipolysis in co-cultured adipocytes, thus reducing the levels of blood lipids. 44 When 3 T3-L1 adipocytes were treated with fucoidan, oil red-O staining showed a decreased content of TG and the induction of lipolysis, reducing the accumulation of TG in a fucoidan concentration-dependent manner. 45 Fucoidan from Mexican ginseng inhibited the proliferation of 3 T3-L1 preadipocytes. After oil red-O staining, fucoidan was also shown to decrease lipid accumulation in adipocytes. On studying the mechanism, fucoidan was seen to significantly down-regulate SREBP-1 C and further down-regulate the expression of fatty acid synthase-related genes, fatty acid transporter-related genes, and triglyceride synthase-related genes.39,46 Fucoidan can also down-regulate fat-specific fatty acid binding protein and acetyl-CoA carboxylase to inhibit fat accumulation and effectively reduce blood lipids, similar to the effects of hypolipidemic drugs. 47
Increasing lipid metabolism
The liver is the most critical metabolic and biotransformation organ in the body and plays an important role in lipid metabolism, especially in maintaining the lipid metabolic balance. 48 The liver has been identified as a possible target for fucoidan treatment for dyslipidemia. Jinhee Park and Hui Xu found that fucoidan inhibited the expression of SREBPs in the liver and further regulated the expression of downstream genes for acetyl-CoA carboxylase, fatty acid synthase, HMG-CoA-R, and LDLR.35,49 In addition, fucoidan can inhibit the expression of SR-B1, CD36, PPARS, CYP7A1, and ATP binding cassette transporter, thus promoting lipid uptake and metabolism. 50
In ApoE mice fed with a high-fat diet with 1% or 5% fucoidan for 12 weeks, the treatment significantly reduced the thickness of lipid-rich plaques in the aorta by increasing plasma lipoprotein lipase (LPL) activity. In addition, Plasma TC, TG, and non-low-density lipoprotein decreased by 28.9%, 35.6%, and 31.7%, respectively. 51 In a mouse model of hyperlipidemia, the activities of serum LCAT, hepatic endothelial lipase (HL), and LPL increased after the intragastric administration of sargassum fucoidan, indicating that fucoidan has a potent hypolipidemic effect that acts by accelerating the catabolism of TC and LDL. 52 Fucoidan induced LPL secretion in a dose- and time-dependent manner in vitro, increased ApoC-II-mediated LPL activation in the blood, regulated blood TG content, and accelerated TG clearance. 51
Fucoidan plays a role in reducing blood lipids by regulating the activities of proteins and enzymes involved in cholesterol synthesis, transport, and metabolism. Table 1 summarizes the lipid-lowering mechanisms of fucoidan.
Lipid-lowering mechanisms of fucoidan.
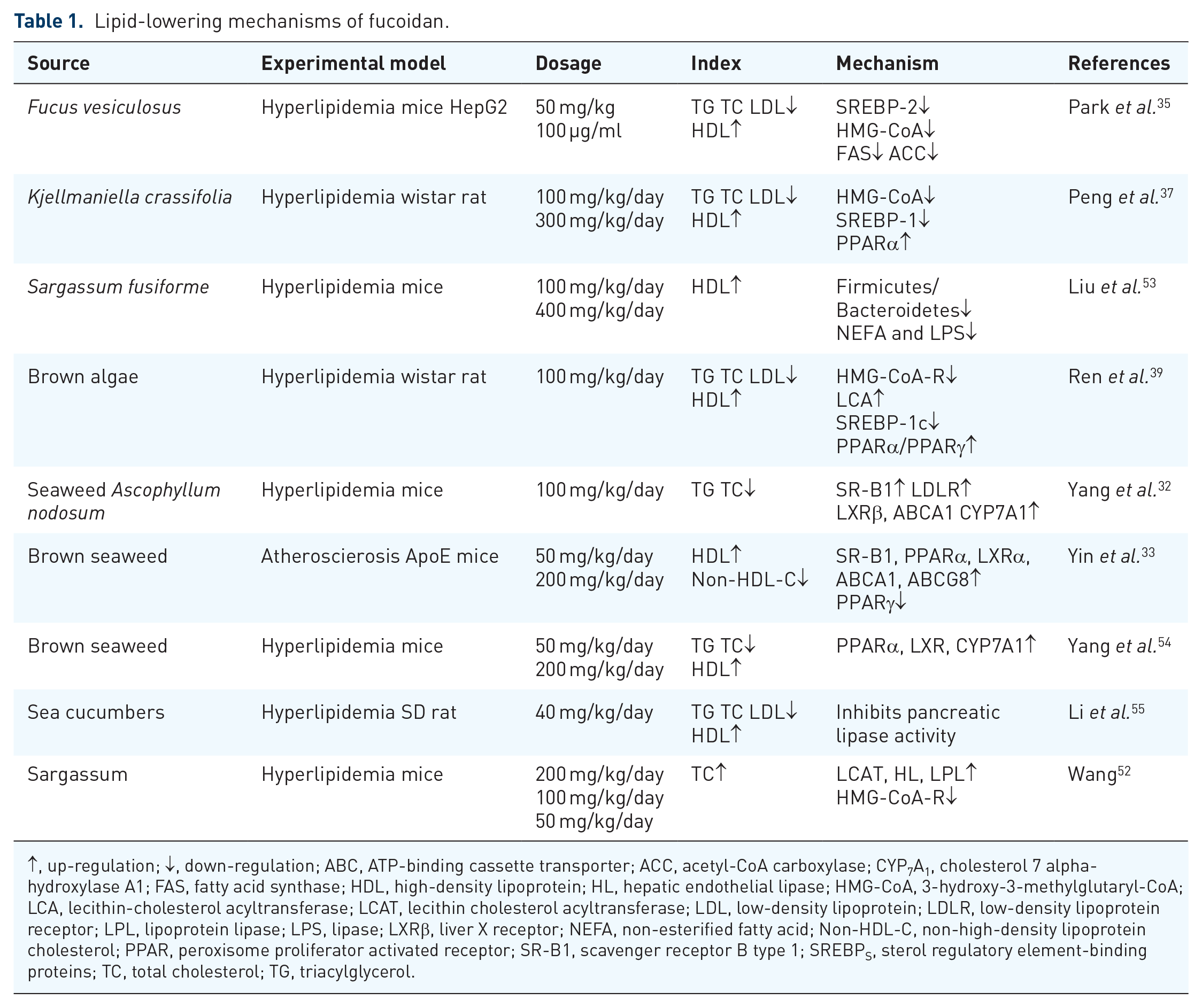
↑, up-regulation; ↓, down-regulation; ABC, ATP-binding cassette transporter; ACC, acetyl-CoA carboxylase; CYP7A1, cholesterol 7 alpha-hydroxylase A1; FAS, fatty acid synthase; HDL, high-density lipoprotein; HL, hepatic endothelial lipase; HMG-CoA, 3-hydroxy-3-methylglutaryl-CoA; LCA, lecithin-cholesterol acyltransferase; LCAT, lecithin cholesterol acyltransferase; LDL, low-density lipoprotein; LDLR, low-density lipoprotein receptor; LPL, lipoprotein lipase; LPS, lipase; LXRβ, liver X receptor; NEFA, non-esterified fatty acid; Non-HDL-C, non-high-density lipoprotein cholesterol; PPAR, peroxisome proliferator activated receptor; SR-B1, scavenger receptor B type 1; SREBPS, sterol regulatory element-binding proteins; TC, total cholesterol; TG, triacylglycerol.
Therapeutic effects of fucoidan on atherosclerosis
AS, which is an important pathological cause of cardiovascular disease, is generally considered to be a chronic inflammation induced by lipid accumulation. 51 In the process of AS, lipids are first deposited on blood vessel walls; macrophages then absorb lipid oxides through scavenger receptors to form foam cells, and smooth muscle cells proliferate and grow. Plaques then develop into unstable plaques, increasing the risk of plaque rupture and thrombosis, which in turn endangers the life of the patient. Therefore, it is essential that drugs to treat AS and slow the course of the disease are developed. Natural medicines from marine sources are considered ideal candidates for the effective prevention and treatment of atherosclerosis because of their extensive pharmacological activities. Recently, research on the biological activity of fucoidan has increased rapidly. Experiments in vivo and in vitro show that the course of atherosclerosis slows down significantly after fucoidan treatment; thus, this compound is considered to be a promising therapeutic agent for atherosclerosis.56,57
Treatment of endothelial cells in AS
AS is a cardiovascular and inflammatory disease related to endothelial dysfunction. 58 With the continuous increase in blood lipids, large amounts of LDL, LDL-C, ApoB, and other proteins are deposited on the arterial wall. The modified LDL becomes oxidized (Ox)-LDL, which causes a series of pathological changes. Lipids and inflammatory cytokines accumulate in the arterial intima 59 and initiate an inflammatory cascade, local endothelial cell dysfunction, and vascular endothelial cell damage, which play important roles in the process of atherosclerosis. 60 Ox-LDL also induces the production of reactive oxygen species, which mediate a variety of pathological processes (including lipid peroxidation), destroy redox homeostasis, and lead to the progression of atherosclerosis. 61 The fucoidan isolated from brown algae exhibited active oxygen scavenging activity in a concentration-dependent manner. 62 According to reports, the fucoidan extracted from kelp can be used to treat diseases caused by free radical damage. 63 Free radicals interact with endothelial cells and destroy cell membranes, leading to endothelial cell dysfunction and damage, and fucoidan scavenges free radicals and enhances the activity of antioxidant enzymes. 64 Nadir et al. found that sulfated polysaccharides have a heparin-like effect, protecting endothelial cells from oxidative free radical damage. It is speculated that negatively charged fucoidan binds and inactivates cationic proteins, activating the complement system and histamine and thus increasing the stability of vascular endothelial cell membranes. 65
High blood pressure, smoking, an unhealthy diet, heavy drinking, metabolic syndrome, and other factors also induce the production of inflammatory factors. 66 Pro-inflammatory cytokines and adhesion molecules are markers of systemic inflammation and play an important role in endothelial dysfunction and the development of AS. 67 Fucoidan can reduce the expression of endothelin-1 and the pro-inflammatory cytokines interferon (IFN)-γ and tumor necrosis factor-α (TNF)-α, reduce the intensity of inflammation, improve metabolic disorders, and protect endothelial cells from injury. In addition, fucoidan can enhance immune activity and reduce the release of inflammatory cytokines, thus reducing damage to endothelial cells. 68
Treatment of macrophages in AS
As important immune cells, monocytes/macrophages are considered to be the first cells to enter atherosclerotic lesions, and they play important roles in the formation, development, and prognosis of atherosclerotic plaques. Monocytes are recruited to the inflamed endothelial region through the interaction between the P-lectin glycoprotein ligand-1 and endothelial agglutinin secreted by platelets and endothelial cells. Under the action of a variety of proteins, such as the monocyte integrin VLA-4, vascular cell adhesion molecule 1, and intercellular adhesion molecule 1, monocytes adhere to and pass between endothelial cells and enter the intima of blood vessels, where they differentiate into macrophages.
With the continuous progression of atherosclerosis, macrophages activate and promote the migration and proliferation of vascular smooth muscle cells. 69 Collagen fibers are synthesized and secreted and gradually cover the surface of the lesion area to form the cap structure of fibrous plaques. Under the continuous activity of the inflammatory environment, IFN γ secreted by T cells reduces the ability of vascular smooth muscle to synthesize collagen, while matrix metalloproteinases (MMP) released by macrophages degrade the collagen, which weakens and destabilizes the cap structure. 70 Therefore, a variety of secondary lesions, such as thrombi, and plaque ruptures occur easily, eventually leading to serious cardiovascular disease. Therefore, the treatment of macrophages plays a positive role in preventing the occurrence and development of cardiovascular diseases.
Regulation of macrophage polarization
Macrophages are a group of immune cells with high phenotypic and functional heterogeneity that can change their polarization to adapt to complex external conditions. 71 Macrophages show a high degree of heterogeneity in the process of atherosclerosis. When macrophages are affected by various plaque microenvironment stimuli, such as lipid oxides, cytokines, and aging red blood cells, they polarize into two main phenotypes: pro-inflammatory M1 and anti-inflammatory M2. 72 AS can be regarded as a chronic inflammatory state, and anti-inflammatory macrophages contribute to tissue repair and remodeling and plaque stability. 59 Therefore, regulating macrophage polarization and changing the proportion of macrophage phenotypes in plaques present opportunities for new treatments for atherosclerosis. 73
In an atherosclerosis mouse model with unstable plaques, we found that the plaques showed a significant increase in M1 markers (CD86 and iNOS) and fewer M2 markers (Arg1 and TGF-b), while the overexpression of STAT6 basically reversed this phenomenon. Up-regulation of STAT6 promoted macrophages to differentiate into M2 subtypes, thus promoting the stability of the atherosclerotic plaques. 74 Previous studies have shown that, in an obese mouse model induced by a high-fat and -glucose diet, fucoidan extracted from sea cucumbers reduced the production of inflammatory cytokines by activating PPAR γ. The expression of M2 marker genes, CD206, Arg-1, and IL-10, increased significantly in the liver, while levels of M1 markers TNF-α, IL-1 β, and iNOS decreased, indicating that administering fucoidan increased the polarization of liver M2/M1 cells, and thereby reduced the inflammatory infiltration of epididymal adipose tissue. 44
Reducing macrophage inflammation
At the end of the 20th century, the famous pathologist Ross first put forward the ‘inflammation theory’ of atherosclerosis, which provided new ideas for the treatment of the condition. Studies have shown that fucoidan can reduce the inflammatory cytokines TNF-α, IL-1b, and iNOS released by macrophages and significantly reduce the adhesion of the Ox-LDL coating to the surface of macrophages, 75 thus reducing the transformation of macrophages into foam cells. Fucoidan from brown algae enhanced p62/SQSTM1-dependent selective autophagy by targeting macrophages, promoting the co-localization of NLRP3 and p62, inhibiting the activation of NLRP3 inflammatory bodies, and thus reducing inflammation and slowing the progression of atherosclerotic plaques. 76 A mechanistic study has shown that fucoidan isolated from Saccharomyces japonicum can significantly inhibit the production of pro-inflammatory cytokines, such as iNOS, COX-2, and TNF-α induced, by lipopolysaccharides and effectively inhibit inflammation by blocking NF-κB, mitogen-activated protein kinase, and JAK-STAT pathways. 77
Other effects on macrophages
Under the action of scavenger receptor A and type B family member CD36, which are expressed on the surface of macrophages, macrophages excessively phagocytose the modified lipid Ox-LDL, which accumulates near the endothelium, and serious accumulation of lipids in the cells is promoted by negative feedback regulation of the related receptors. Finally, the cells gradually become foamy and turn into foam cells that gradually accumulate to form the initial marker of atherosclerosis—early lipid stripes. 78 Fucoidan has been found to significantly inhibit Ox-LDL uptake by macrophages at a range of concentrations (1-100 mg/ml), thus reducing the possibility of macrophages transforming into foam cells. 79 In addition, fucoidan attenuates the migration of THP-1-derived macrophages and the production of pro-inflammatory factors by regulating the production of colony-stimulating factor 1, slowing the development of atherosclerosis. 80
Promoting autophagy of foam cells
During the formation of atherosclerotic plaques, monocytes enter the sub-endothelium of the vascular wall and transform into macrophages. Modified lipoproteins increase the risk of cholesterol accumulation in monocyte-derived macrophages. 81 A large number of lipid droplets also gathers in smooth muscle cells (SMCs), which determines the possibility of their conversion into foam cells. It has been reported that macrophages are the main source of foam cell formation, but SMCs can produce foam cells during the late and early pathological stages in humans. Stem/progenitor cells and endothelial cells can also form foam cells. 81 Foam cells are a sign of early pathological changes in AS; therefore, they also present important targets for the treatment of AS.
Autophagy, a cell and tissue self-renewal process, can degrade the lipids in foam cells and is particularly critical in foam cell formation. Fucoidan can enhance the autophagy-lysosome system of foam cells, increase cell autophagy to degrade lipids, and thus play a role in anti-atherosclerosis defenses. 82 The fusion of autophagosomes and lysosomes can remove improperly folded or polymerized proteins, excessive or damaged cells, and intracellular pathogens.83,84 It has been demonstrated that fucoidan can reduce the formation of new plaques by decomposing the lipids in foam cells via autophagy mechanisms. Fucoidan was found to induce the transport of chemokine receptor-4 (CXCR4) and human MMP-9 protein into autophagosomes by recruiting autophagy substrate protein P62 and form autophagy lysosomes with the participation of lysosomes, which degraded their contents. This results in a decrease in CXCR4 protein production and MMP9 exocrine secretion on the cell membrane, reducing the cell’s ability to migrate and invade. 85 Fucoidan reduces lipid accumulation in foam cells by up-regulating the expression of TFEB, p62/SQSTM1, and microtubule-associated protein light chain 3, which are the main regulators of autophagy and lysosome function, as well as enhancing autophagy. 82
Treatment for vascular smooth muscle cells in AS
Vascular SMCs exist in the tunica media of the vascular wall. Studies have shown that, under the action of various stimulating factors and growth factors, the status of vascular SMCs can change from differentiation to de-differentiation, and the cells migrate to the intima and proliferate, which is one of the main causes of vascular wall thickening, decreased vascular compliance, and severe stenosis, leading to diseases such as AS and vascular restenosis. Therefore, the proliferation and migration of smooth muscle cells may accelerate the pathological process of atherosclerosis. 86
Low molecular weight fucoidan (LMWF) improved the inflammatory response by down-regulating IL-6 and up-regulating IL-10 transcription on atherosclerosis in ApoE-knockout mice. LMWF restored p-JNK and cyclin D1 to normal levels, prevented SMCs from migrating to the aortic intima, inhibited the formation of atherosclerotic plaques, and improved the occurrence and development of atherosclerosis. 86 In vitro studies also showed that LMWF reduces the proliferation and migration of rabbit smooth muscle cells, thus reducing the rate of intimal hyperplasia. 72 Arteriogenic factor FGF-2 can increase the contents of smooth muscle cell binding protein and regulate smooth muscle cell proliferation through the MEK/Erk pathway. LMWF down-regulated the expression of FGF-2 signaling pathway genes in the arterial endothelium, thereby inhibiting the proliferation and migration of SMCs and the infiltration of macrophages, and slowing the course of AS. 60
In summary, fucoidan can regulate the activities of endothelial cells, macrophages, and smooth muscle cells in AS through its anti-inflammatory and antioxidant effects. Therefore, fucoidan treatment can be beneficial throughout the entire course of AS, and research and development into fucoidan therapy for cardiovascular diseases is of great significance.
The antithrombotic effect of fucoidan
Thrombotic events, such as myocardial infarction and ischemic stroke, are leading causes of global morbidity and mortality. 87 Late atherosclerotic plaques invade the arterial lumen, hinder blood flow, and lead to tissue ischemia, causing thrombosis. 88 In addition, the lipid necrotic core and the thin fibrous cap of high-risk plaques lead to plaque instability and rupture due to inflammatory cell and diffuse calcification infiltration. The interaction between exposed atherosclerotic plaque components, platelet receptors, and coagulation factors eventually leads to platelet activation and aggregation, followed by thrombosis, which damages the arterial lumen. 89 The formation of a thrombus can block the vascular lumen, and its movement also causes adverse vascular events. For example, strokes caused by thrombi are a serious threat to human health; hence, the search for effective antithrombotic and thrombolytic drugs is an important research area. With the in-depth study of marine natural products, the antithrombotic activity of fucoidan has been widely investigated.
Anticoagulation
The natural active polysaccharide fucoidan has anticoagulant effects. Reportedly, most fucoidans can inhibit the production of thrombin during endogenous and exogenous coagulation. It increases activated partial thromboplastin time (aPTT) and thromboplastin time (TT), and the degree of increase is equal to or higher than that of heparin. 90 A sulfated fucoidan from sea cucumbers was extracted and purified, and its anticoagulant activity was identified. The results showed that heparin cofactor II had inherent anticoagulant activity and specific antithrombin activity. 91 The specific sulfation mode and position of the glycosidic bonds in fucoidan confer its anticoagulation activity. Further studies on the mechanisms have shown that fucoidan strongly inhibits the internal coagulation pathway by targeting the intrinsic coagulation factor Xase. 92 Ganapathy et al. 93 showed that fucoidan significantly inhibited both endogenous and exogenous coagulation factors involved in the coagulation pathway. A fucoidan was isolated and purified from sargassum, and mice treated with the highest concentrations showed the longest clotting time, and the clotting time of each component was longer than that in the presence of aspirin and clopidogrel. 94 Therefore, fucoidan, as an anticoagulant and antithrombotic drug with fewer side effects, has good application prospects for the treatment of cardiovascular diseases.
Regulation of platelet activation
At the site of atherosclerotic plaque rupture, exposure to highly thrombotic matrix proteins and procoagulant factors triggers platelet recruitment. Platelet activation plays a key role in maintaining thrombus stability, preventing platelet activation, and thus preventing aggregation, disrupting the growth of the developing thrombus. 95 Fucoidan extracted and purified from sea cucumbers can be used to treat platelet aggregation caused by the immunosuppressive drug cyclophosphamide. It is speculated that fucoidan can reduce the risk of thrombosis. 96 Fucoidan was seen to have an affinity for the P-selectin expressed by activated platelets in thrombi, and its thrombolytic efficiency was observed by monitoring platelet density. 97 Compared with high-molecular weight fucoidan, free-radical-depolymerized LMWF has better absorption and higher bioavailability; hence, it has the potential to become an oral antithrombotic drug. 98 It has been reported that LMWF with a molecular weight of <10 KDa has a good in vivo absorption rate. 99 In further studies, highly sulfated fucoidan with a molecular weight of 3900 Da seemed to be a more suitable antithrombotic drug, with specific inhibitory activity on platelet aggregation and low anticoagulant activity, and it was associated with a low risk of bleeding in vivo. 100
Thrombolysis
The formation of a lipid necrotic core and the thin fibrous cap on atherosclerotic high-risk plaques means the plaques easily rupture and form an intraluminal thrombus, which is the main cause of acute coronary syndrome and cardiovascular disease. 101 The use of thrombolytic drugs is an excellent treatment strategy for thrombosis. Traditional drugs, such as tissue plasminogen activator (t-PA), urokinase, and streptokinase, can unblock occluded blood vessels, but bleeding is always a risk. Fucoidan has been shown to covalently bind to dilysine (which can bind t-PA non-covalently) in vivo to target a thrombus in the lumen and improve the efficiency of t-PA fibrinolysis against acute thrombosis. 102
Reportedly, the ligands of macrophage scavenger receptors can induce the production of urokinase-type plasminogen activator. 103 Fucoidan also plays a thrombolytic effect by enhancing the concentration and activity of t-PA. Sulfated fucoidan isolated and purified from brown algae was used for antithrombotic activity analysis, which showed that fucoidan increased the percentage of t-PA and plasminogen activator inhibitor 1, indicating that it had greater fibrinolytic activity and better effect of thrombolysis. 104 Fucoidan from Fucus and Undaria increased t-PA release from the vascular endothelium in a dose-dependent manner, thus exerting a thrombolytic effect. 105 As a thrombolytic drug, fucoidan has important pharmacological significance, and there is no risk of bleeding after thrombolysis.
In general, fucoidan has dual effects in that it not only prevents thrombosis but also promotes thrombolysis. After the use of fucoidan, the incidence of myocardial infarction is lower and ischemic cardiac events are reduced, so it has high clinical value and provides a new resource for the development of antithrombotic drugs for AS.
The impact of fucoidan on cardiovascular and cerebrovascular disease prognosis
If patients with atherosclerosis do not receive timely and effective treatment, vascular stenosis and blockage can cause complications such as stroke, myocardial infarction, and even sudden death. Primary and secondary cardiovascular and cerebrovascular prevention measures can reduce cardiovascular and cerebrovascular events, improve a patient’s quality of life, and reduce complication-related costs. 106 The natural marine drug fucoidan also has a positive effect on reconstruction after infarction.
Ischemic stroke is caused by blood flow damage. Mice induced with chronic hypoxia for 35 days were given fucoidan P-selectin antibody, which significantly improved blood vessel remodeling and restored right ventricular function. 107 Fucoidan extract with high fucose and sulfate contents had an inhibitory effect in an in vitro model of angiogenesis, 108 and LMWF can promote the angiogenesis- and migration-promoting activity of human endothelial cells that is induced by FGF-2, which may be conducive to blood remodeling in the ischemic area. 109 Compared with FGF-2 alone, fucoidan and FGF-2 have a greater effect on tube formation and cell migration. The results showed that, in the presence of FGF-2, fucoidan can activate p38 and JNK and induce angiogenesis through AKT/MMP-2 signaling. 110
In a mouse hindlimb ischemia model, the antioxidant properties of fucoidan protected neurons from the cerebral oxidative stress induced by transient ischemia and alleviated the aggravation of ischemic brain injury under obesity. 111 Fucoidan significantly reduces the neurological deficit and infarct volume during cerebral ischemia and reperfusion by reducing inflammatory factor levels and oxidative stress and inhibiting cell apoptosis and the mitogen-activated protein kinase (MAPK) pathway. 112 Fucoidan can reduce the recruitment of white blood cells, decrease the infiltration of neutrophils, and weaken the inflammatory response, thereby exerting a neuroprotective effect in cerebral ischemia injury. 113 Fucoidan exerts a neuroprotective effect by inhibiting inflammation, oxidative stress, cell apoptosis, and other pathways, and it can be used as an effective neuroprotective agent and provide a new strategy for improving cardiovascular and cerebrovascular disease prognosis.
Concluding remarks and future outlooks
The incidence of cardiovascular disease is increasing year by year, and CVD has become the main cause of mortality worldwide; if reasonable treatment is not available soon, the conditions will lead to many more deaths. Fucoidan is a complex marine acidic polysaccharide with diverse biological activities that is found in a wide range of organisms, and it can play an important therapeutic role at all stages of cardiovascular disease: initial hyperlipidemia, the formation of fat streaks in the arteries, lipid accumulation, fibrous plaques, atherosclerotic plaques, plaque hemorrhage and rupture, thrombosis, and cerebral infarction. Hyperlipidemia is the basis of many cardiovascular and cerebrovascular diseases, and fucoidan has shown particularly diverse and potent effects on lipid levels. The anti-inflammatory, lipid-lowering, and antioxidant effects of fucoidan can have a positive impact over the entire course of atherosclerosis, and its prospects as a treatment for cardiovascular and cerebrovascular diseases are good.
Although fucoidan has a wide range of biological activities and promising preclinical effects, there are still some problems that need to be urgently solved before fucoidan can be developed as a drug. As a marine polysaccharide, its specific structure is still unclear, and its sulfate content, monosaccharide content, and molecular weight vary greatly among the different sources and extraction methods. Furthermore, the relationship between its composition and activity remains uncertain. Research on polysaccharides brings certain difficulties, and clarifying the molecular structure of fucoidan is still a major challenge. It is known that fucoidan is a high-polarity polymer compound with limited absorption in the human body. In addition, there have been few studies to date on its pharmacokinetics, and further research to determine its clinical dosage, drug efficacy, toxicity, and so on is of great significance. Therefore, the clinical application of fucoidan will require substantial effort. However, an increasing number of people use fucoidan as a dietary supplement and health product, and fucoidan should have broader research value as a therapeutic drug for cardiovascular diseases.
Footnotes
Acknowledgements
We thank excellent collaboration and our participants for their valuable time and cooperation.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shandong Provincial Natural Science Foundation, China (ZR2017MH040).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This article is a review article; it is a summary of the articles in recent years, and a summary of the experiments done by the predecessors. It does not involve our own experiments and hence no ethics approval is needed.