
Abstract
Hidradenitis suppurativa (HS) is a chronic inflammatory skin disease characterized by the presence of painful nodules, abscesses, chronically draining fistulas, and scarring in apocrine gland-bearing areas of the body. The exact pathogenesis of HS is not yet well understood, but there is a consensus in considering HS a multifactorial disease with a genetic predisposition, an inflammatory dysregulation, and an influence of environmental modifying factors. Therapeutic approach of HS is challenging due to the wide clinical manifestations of the disease and the complex pathogenesis. This review describes evidence for effectiveness of current and emerging HS therapies. Topical therapy, systemic treatments, biological agents, surgery, and light therapy have been used for HS with variable results. Adalimumab is the only US Food and Drug Administration (FDA) approved biologic agent for moderate-to-severe HS, but new therapeutic options are being studied, targeting different specific cytokines involved in HS pathogenesis. Comparing treatment outcomes between therapies is difficult due to the lack of randomized controlled trials. Treatment strategy should be selected in concordance to disease severity and requires combination of treatments in most cases.
Keywords
Introduction
Hidradenitis suppurativa (HS) is a chronic, relapsing, inflammatory skin disease characterized by the inflammation of hair follicles in apocrine gland-bearing areas of the body, manifesting as painful nodules, abscesses, chronically draining fistulas, and scarring.1,2 It is a disabling disease with great psychological and functional impact on patients due to pain and malodorous discharge of the lesions. Prevalence estimates vary depending on the method of data collection and ethnic background, but range between 0.7% and 1.2%, according to the largest cross-sectional and registry-based studies; 3 in most patients, onset of HS takes place after puberty, and the disease predominantly affects women in Western countries. 4
Due to the polymorphic nature of HS manifestations and patient characteristics, several attempts at phenotypic classification have been published; in a recent two-step cluster analysis of Mediterranean patients that included biomarkers, two endotypic clusters have been identified: cluster 1 (65% of patients) is characterized by non-obese males with early onset HS, nodular lesions in posterior sites, history of pilonidal sinus, high serum levels of IL-10, and presence of gamma-secretase mutations; and cluster 2 (35% of patients), characterized by obese females or males with later onset HS, lesions in anterior sites, more sinuses and abscesses, less nodules, and higher serum concentrations of IL-1, C-reactive protein, IL-17, and IL-6, which is more related to systemic inflammation. 5
The pathogenesis of HS is not yet well understood, but there is a consensus in considering HS a multifactorial disease with implication of different immunological factors.6–8 This makes HS a complex disease with a challenging approach. 9
While mild disease can be usually controlled with lifestyle modifications, weight loss, stop smoking, topical treatment, and oral antibiotics, management of moderate-to-severe HS, frequently refractory to conventional treatments, 10 is a great challenge for clinicians, and new therapeutic avenues are under study.
The aim of this article is to provide a narrative review of current, new, and future potential treatments of HS, with a special focus on medical modalities. A PubMed search was conducted, including the terms ‘hidradenitis suppurativa’, ‘treatment’, OR ‘therapy’, and the different treatments discussed in this article. Also, all the clinical trials of HS in www.clinicaltrials.gov were reviewed. To be included, studies had to discuss HS and treatment as a primary theme, be written in English, and be published in a peer-reviewed journal. After collecting the information, we collated, summarized, and reported the results using narrative synthesis.
Disease severity and outcome measures
Numerous tools have been described for assessment of patients with HS. Hurley staging has been recommended in the clinical setting, 9 since it is simple and helps determine therapeutic needs (Table 1). 11 However, it does not count the number of affected areas and fails to assess disease activity or treatment response. In an attempt to solve these limitations, the Refined Hurley staging has been proposed (Table 1). 12 Abscess and nodule counts (AN count) is feasible to perform in clinical practice and may facilitate therapeutic decisions. 9
Hurley score.

BSA, Body Surface Area.
In research settings, the Hidradenitis Suppurativa Clinical Response (HiSCR) is the most validated and widely used measure for assessing treatment response. Patients who achieve HiSCR should show a 50% reduction in the sum of abscesses and inflammatory nodules, no increase in the number of abscesses, and no increase in the number of draining fistulas from baseline. 13 The Modified Sartorius Score (mSS), the Hidradenitis Suppurativa Physician’s Global Assessment (HS-PGA), the Hidradenitis Suppurativa Severity Index (HSSI), and the International Hidradenitis Suppurativa Severity Score System (ISH4) 14 are used in clinical trials too (Tables 2 and 3). 9 The last four are also useful in daily practice.
Other outcome measures used in clinical trials.
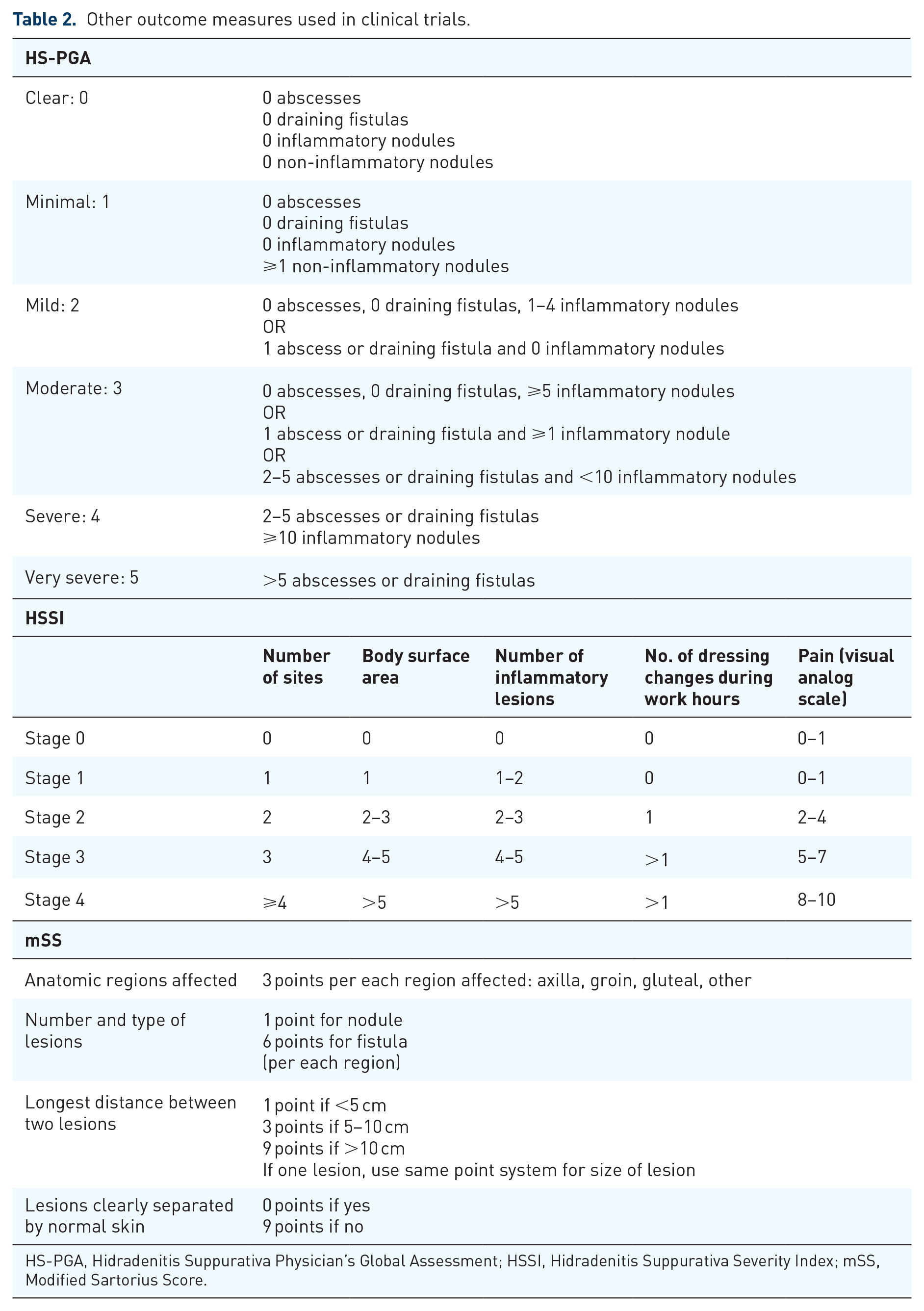
HS-PGA, Hidradenitis Suppurativa Physician’s Global Assessment; HSSI, Hidradenitis Suppurativa Severity Index; mSS, Modified Sartorius Score.
IHS4.
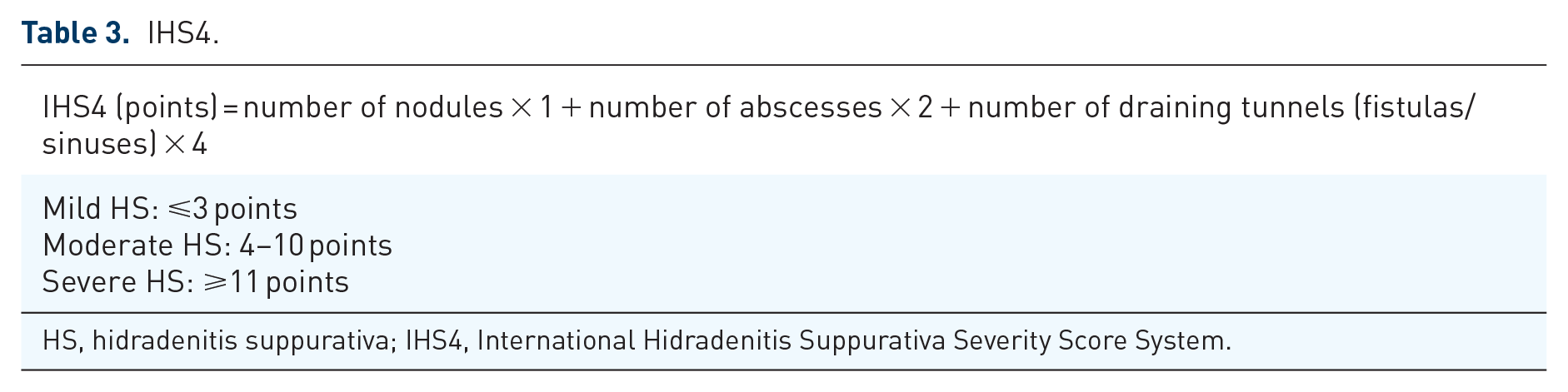
HS, hidradenitis suppurativa; IHS4, International Hidradenitis Suppurativa Severity Score System.
Pathogenesis
Genetic, environmental, and immunologic factors intervene in the pathogenesis of HS (Figure 1). 15

Causes of HS: Genetic, environmental, and immunologic factors intervene in the pathogenesis of HS. Monogenic HS can be divided into defects in Notch and γ-Secretase signaling pathways (PSENEN, NCSTN and PSEN1, POFUT1, POGLUT1) and defects in inflammasome function (NLRP3, MEFV, NOD2, NLRP12, LPIN2). Lifestyle factors including friction, smoking, obesity, and a dysbiosis have demonstrated to be contributors to HS development.
Approximately 30% of patients with HS have a positive family history. Monogenic HS is rare and can be classified into (1) defects in Notch and γ-secretase signaling pathways that lead to a severe comedone-predominant HS phenotype and (2) defects in inflammasome function that results in an inflammatory phenotype of HS with additional systemic features (Figure 1). 16
The genes encoding for proteins of the γ-secretase transmembrane complex with most widely described mutations in HS are PSENEN (coding for presenilin enhancer), NCSTN (nicastrin), and PSEN1 (presenilin-1). 17 These mutations usually show familiar aggregation with autosomal dominant inheritance and incomplete penetration but have also been observed in sporadic cases.17–20 These mutations result in reduced signaling of the Notch pathway (involved in cell maturation and differentiation) that leads to hyperkeratinization of the follicular epithelium, abnormal keratinocyte differentiation, disruption of the normal hair follicle cycle, and formation of follicular cysts.21,22 Mutations in POFUT1 (O-fructosyltransferase 1), and POGLUT1 (protein O-glucosyltransferase 1), which have also been involved in decreased Notch signaling, have been described in patients with concomitant HS and Dowling-Degos disease.23,24 Also mutation in nicastrin have been reported in patients with HS and Dowling-Degos disease. 25
As regards inflammasome dysfunction, it is recognized as a central driver for many autoinflammatory disorders, some of them associated to HS, such as Familial Mediterranean fever (MEFV mutation).26,27 Inflammasome upregulation (PSTPIP1 mutation) has also been demonstrated in pyogenic arthritis, pyoderma gangrenosum, and acne (PAPA) syndrome and pyoderma gangrenosum, acne, arthritis, and HS (PAPASH) syndrome.28,29 In the pyoderma gangrenosum, acne, and HS (PASH) syndrome, diverse mutations in the Notch signaling pathway and inflammasome function genes (NCSTN, NOD2, MEFV, NLRP3, NLRP12, PSTPIP1, LPIN2) have been reported.16,30
Environmental factors such as mechanical stress, 31 obesity, 32 diabetes, 32 metabolic syndrome, 33 diet, 34 smoking, 35 and hormonal factors 36 are known to contribute to the development or exacerbation of HS (Figure 1). Furthermore, HS has been associated to comorbidities sharing immunological dysregulation, such as axial spondyloarthritis, inflammatory bowel disease (IBD), and psoriasis. 37
Skin microbiota is also considered an environmental causative factor for HS. A pattern of cutaneous dysbiosis has been associated to HS pathogenesis after observing bacterial colonization of superficial and deep HS lesions. 38 Bacteria play a major role in the activation of the innate immunologic response (see below), and it is also thought to play a role in the maintenance of the inflammatory response. 39 The exact mechanism of the influence of microbiome in HS immunologic response is not fully understood. 38
Follicular occlusion is the first event observed in early lesions; it is produced by infundibular keratosis and hyperplasia of the follicular epithelium (Figure 2). Local cell damage caused by mechanical friction leads to release of cellular damage-associated molecular patterns (DAMPs) and penetration of microbial components into the follicles, which become dilated and eventually rupture.40,41 The release of follicular content to the dermis produces a significant inflammatory response, primarily mediated by an innate immune response to the presence of DAMPs, pathogen-associated molecular patterns (PAMPs), and microbial antigens of the commensal flora, followed by activation of Th1 and Th17 pathways. PAMPs and DAMPs released to the dermis activate macrophages through Toll-like receptor (TLR) and induce production of tumor necrosis factor-alpha (TNF-α) and, via inflammasome activation, IL-1β (Figure 2). 42 The inflammasome (Figure 3) is an intracellular protein complex located in macrophages and neutrophils essential for the control of the innate immune system. Recognition of PAMPs and DAMPs activates the inflammasome through a microbial or damage-sensing protein of the NOD-like receptor family (NLRP3). NLRP3 activates Caspase-1 and processes pro-IL-1β into its active form. 16 Secretion of IL-1β will trigger an uncontrolled activation of innate immunity, perpetuating the inflammatory activity. 43 IL-1β induces the expression of CXCL1 and CXCL6 by fibroblasts, and TNF-α induces the expression of CXCL8, CXCL11, CCL2, and CCL20 by keratinocytes. These chemokines will attract granulocytes, T cells, B cells, and monocytes; the latter differentiate to macrophages (Figure 2).40,4 Fibroblast activation via IL-1β also enhances the secretion of a range of matrix metalloproteinases (MMPs), IL-32, and IL-6 which implicates massive tissue immune cell infiltration, pus formation, and contributes to tissue destruction and fibrosis (Figure 4). 44

Early stage HS: The first event in HS lesions is hyperkeratosis and hyperplasia of the infundibular epithelium (1), produced by chronic friction, genetic predisposition, and environmental factors. This leads to follicular ‘plugging’, follicular dilatation (2), and eventual rupture (3). Bacteria and cellular debris including pathogen- and damage-associated molecular patterns (PAMPs and DAMPs) are released to the dermis initiating an innate immune response when recognized by TLRs. PAMPs and DAMPs activate the inflammasome response involving the NOD-like receptor protein 3 (NLRP3) in macrophages and neutrophils with subsequent activation of caspase-1 and activation of proinflammatory cytokines such as IL-1β. IL-1β provokes the production of chemokines by fibroblasts (CXCL1 and CXCL6) that will mainly attract neutrophils. TNF-α, secreted by macrophages and dendritic cells, induces the production by keratinocytes of a wide range of chemokines (CXCL8, CXCL11, CCL20, and CCL2), which attract neutrophils, subsets of T cells, and monocytes into the skin. Activated dendritic cells, through the production of IL-23 and IL-12, promote polarization of CD4+ T cells toward Th17 and Th1 cells, respectively. Activation of the complement pathway contributes to neutrophil activation and recruitment by C3a and C5a.

Inflammasome: Recognition of bacteria, PAMPs, and DAMPs activates the inflammasome through a microbial or damage-sensing protein of the NOD-like receptor family (NLRP3). NLRP3 activates Caspase-1 and cleaves pro-IL-1β yielding its active form. Secreted IL-1β recruits inflammatory cells (mainly neutrophils) and perpetuates the immune response. This process is favored by the presence of genetic mutations in genes that codify proteins involved in inflammasome function, such as NLRP3.

Advanced stage: Nodule, abscess, and fistula formation. Th1 (IL-12 polarized) cells produce INF-γ that will activate endothelial cells to recruit more inflammatory cells and will stimulate macrophages to produce IL-10, probably as a compensatory anti-inflammatory response. TNF-α, produced by macrophages, dendritic cells, and T lymphocytes, favors the development of Th17 cells, decreases adiponectin (anti-inflammatory hormone) secretion from adipocytes, and increases the expression of matrix metalloproteinases (MMPs). TNF-α contributes in recruiting inflammatory cells, and the massive infiltration will lead to the nodule and abscesses formation (4) and the production of pus. IL-17A and IL-17F stimulate neutrophils and macrophages resulting in an increase of the expression of IL-1β, IL-6, and TNF-α, as well as MMPs. TNF-α, IL-17A, and IL-17F induce keratinocyte proliferation. In turn, keratinocytes produce IL-17C and IL-36, which act in an autocrine manner to further potentiate their activation and proliferation worsening epidermal acanthosis. IL-1β activates fibroblasts and they produce MMPs, which will conduce to fistula formation (5) and fibrosis through extracellular matrix degeneration. IL-17/IL-22 signaling contributes to sinus keratinization. IL-1α, IL-1β, TNF-α, IL-6, IL-17, IL-12, IL-23, and IL-10 have been identified in pus from HS lesions.
The complement system has recently attracted attention in inflammatory cutaneous disorders such as HS. The complement pathway, through C3 and C5, produces inflammation, opsonization, and bacterial lysis. C3a and C5a are strong neutrophil activators and recruiters (Figure 2), suggesting that complement inhibition might be a line of action in HS treatment.45,46 High blood concentrations of C5a have been found in HS patients compared with healthy subjects, 42 and reduction of nodules and draining dermal tunnels have been observed following C5a inhibition. 47
Interferon-gamma (IFN-γ) is secreted by Th1 cells and activates endothelial cells contributing to the massive infiltration of inflammatory cells perpetuating the immune response (Figure 4). IFN-γ also activates macrophages to synthesize IL-10, which inhibits Th22 cells, thus leading to a reduction of IL-22 levels. The drop of IL-22 concentration will lessen the production of AMPs. 42
TNF-α is produced by macrophages and activated dendritic cells; it has multiple functions in the innate and adaptive response happening in HS. Elevated levels of TNF-α can be found in skin of patients with HS and they correlate with HS severity. 43 It favors the development of T helper 17 (Th17) cells, decreases adiponectin (anti-inflammatory hormone) secretion from adipocytes, and increases the expression of MMPs (Figure 4). 42 Also, a high expression of mammalian target of rapamycin gen (mTOR), implicated in cellular regulation of survival, growth, and proliferation, has been found in lesional skin. mTORC1 is important for innate and adaptive immunity and Th17 differentiation; its implication in inflammatory response in HS has been proved after the observation of a reduction of the expression of mTORC1 in lesional skin after treatment with adalimumab (ADA) during 6 weeks. 48 Anti-TNF-α treatment has also been shown to decrease circulating levels of IL-1β, IL-6, IL-8, IL-10, and IL-17A, proving its effects in innate and adaptive immunity and highlighting its modulatory effect on Th17 activity. 49
High serum levels of IL-17A have been found in HS and correlate with the severity of inflammation. 50 IL-17 stimulates neutrophils and macrophages resulting in an increase of the expression of IL-1β, IL-6, and TNF-α, as well as caspases and MMPs in the follicular unit and perilesional skin (Figure 4). 42 The fundamental role of IL-17 isoforms – bridging the innate and adaptive (via the IL-23/IL-17 pathway) immune responses – in the pathogenesis of HS is currently well recognized and has led to the development of clinical trials with anti-IL-17 biologic agents. Th17 cells are a lineage of CD4+ T helper cells producing canonical IL-17A and IL-17F as well as other cytokines; IL-23 produced by dendritic cells has a fundamental role in the commitment and maintenance of this polarization (Figure 2). Both IL-17 and IL-23 are increased in lesional and perilesional HS skin.51,52
IL-12 and IL-23, driving Th1 and Th17 commitment, are abundantly expressed by macrophages infiltrating papillary and reticular dermis, 51 and have also been targeted for therapeutic purposes.
The inflammatory components of dermal abscesses that form as a consequence of follicular disruption probably contribute to re-epithelialization and formation of dermal cysts, sinuses, fistulas, and epithelialized tunnels, which are a structural hallmark of severe HS. These epithelial structures are immunologically active, contributing IL-17C and IL-36 to the increased expression of proinflammatory cytokines and chemokines. 53 Their formation is dependent on IL-17/IL-22 signaling; furthermore, the Th17 cytokine IL-22 mediates proinflammatory effects on keratinocytes leading to epidermal acanthosis and hyperproliferation (Figure 4). 51 These chronic epithelialized cavities contribute to create a favorable habitat for biofilm-producing bacteria, which contribute and perpetuate the inflammatory reaction. 39 Sinus tracts contain an invasive proliferative gelatinous mass that is attached to the sinus tract epithelium and contains inflammatory cells and cytokines (Figure 4). 54
Multiple cytokines, including IL-1α, IL-1β, TNF, IL-6, IL-17, IL-12, IL-23, and IL-10, have been identified in pus secretion of HS lesions (Figure 4), 55 are involved in the pathogenesis of the disease, and have been therapeutically targeted, as discussed below.
Treatment of a multifactorial disease with complex pathogenesis such as HS is necessarily multipronged, with treatment algorithms based on disease severity. 41 In mild stages, topical or oral antibiotics alone or combined with topical or intralesional corticosteroids, and limited surgical or para-surgical interventions, may suffice to control the disease, but as it progresses, combined therapy including systemic and surgical approaches is required. 41
Treatment
Topical treatment
The role of microbiome in HS has been studied for many years and antibiotics are first-line therapy for HS, but antimicrobial treatment alone is unlikely to control disease activity. Monotherapy is considered for mild disease, but in advanced disease, combination with other treatments is needed. 56 Clinical response rates to antibiotics are difficult to compare and quantify due to the lack of controlled randomized clinical trials (RCTs). 56
Topical clindamycin 1% twice daily for 12 weeks is considered a first-line treatment for Hurley I–II stage, supported by two RCTs that showed superiority to placebo and equality to oral tetracyclines.57,58 Recently, an in vitro study evaluated a topical formulation of nanostructured lipid carriers containing clindamycin and rifampicin. They observed that this formulation leads to the accumulation of both antibiotics into the follicle, suggesting that it could be a promising formulation for topical treatment. 59 There are increasing reports of resistant bacterial stains. Knowledge of bacterial resistance profile before initiating therapy, choice of combined therapy over monotherapy, and avoidance of empiric treatments are recommended. 60
Topical resorcinol 15% once daily has been associated to good clinical response in an open-label study, including 65 patients with Hurley I and II HS. Overall, 85.2% (52/65) of patients achieved HiSCR at week 12, and >80% of reduction in AN count was observed. The number of sinus tracts remained unchanged, but a significant reduction in the average length and thickness was observed with ultrasonography at week 12. 61
A phase II open-label study is ongoing to evaluate the effect of topical gentian violet as an antiseptic and wound healing therapy in HS (NCT04388163). 62 A phase II open-label study with topical LTX-109 aims to evaluate its antimicrobial and anti-inflammatory effects in HS treatment (NCT04756336). Also, since biofilm contributes to inflammatory response in HS, its composition and changes after applying a topical antibiofilm surfactant wound gel are under study (NCT04648631). 63
Finally, a phase II open-label trial with topical ruxolitinib 1.5% cream, a JAK1/JAK2 inhibitor, is expected to start promptly (NCT04414514). 64
Systemic treatment
Systemic antibiotic treatment
Tetracyclines (tetracycline, doxycycline, minocycline, lymecycline) are considered first-line oral treatment for HS based on clinical experience. 10 A recent multicenter prospective cohort study showed significant decrease in IHS4 from baseline and a 40% of HiSCR achievement after 12-week treatment with tetracycline. 65 Likewise, a retrospective study comparing the efficacy of lymecycline (300 mg daily) versus the combination therapy clindamycin and rifampicin (600 mg plus 600 mg daily) during 10 weeks in 52 patients (26 per group) observed a 57.7% and 53.8% HiSCR achievement, respectively. 66
Clindamycin and rifampicin used at a dose of 300 mg twice daily have been proven effective in HS in several observational studies65,67–69 and are considered a first-line and second-line treatment for HS. A systematic review of retrospective and prospective series reported response rates from 71% to 93% in 187 patients, strongly favoring their use. 56 As recommended in international HS guidelines, systemic clindamycin and rifampicin (dosage: 300 mg twice daily) should be administered for an average length of 10 weeks in Hurley stage II/III patients presenting with several active lesions. 70 A single-center retrospective study compared the efficacy of rifampicin plus clindamycin versus ADA. Both treatments achieved a statistically significant reduction of mSS, but it was greater in the ADA group. A 34% and 60% of patients achieved HiSCR, respectively. 71
A prospective European cohort study that included 218 patients with HS compared efficacy and tolerability of oral tetracycline and a combination of rifampicin plus clindamycin. The results showed no significant differences in efficacy between the two treatments, regardless of the disease severity. 65
The association of daily clindamycin (600–1800 mg, according to weight) and ofloxacin (200–400 mg) for a mean observation period of 4.3 months in 65 patients led to a 33.8% (22/65) of complete response and a 24.6% (16/65) of partial response. 72 The authors state that the overall response rates obtained (58.4) could be comparable with the ones achieved with association of rifampicin and clindamycin. 56
Prospective and retrospective cohort studies place antibiotic regimens such as rifampin–moxifloxacin–metronidazole combined therapy, iv (intravenous) ceftriaxone and iv ertapenem (particularly effective as a rescue treatment) as a third-line therapy for severe HS patients.56,73,74 It should be taken into account that HS international alliance guidelines recommend only one antibiotic of the same class should be used for a maximum of 12 weeks. 70
Oral retinoids
Oral retinoids have been reported to modulate IL-6 and IFN-γ activity as well as exert antiproliferative activity in keratinocytes. However, there is no compelling evidence of their effect in lesional HS skin. Acitretin results in HS are variable (doses ranging from 0.5 to 0.6 mg/kg/d and mean duration of 3–12 months), with response rates close to 50% 75 and high recurrence rates in monotherapy (up to 40% as reported by Puri and Talwar). 76 However, good clinical outcomes have been reported in some series. 77 Acitretin should be considered a second- or third-line therapy for HS. 56
Isotretinoin has shown discordant results in retrospective cohort studies and case series. 78 Better responses are reported in mild disease and with low doses (<1 mg/kg/d). Isotretinoin should be considered as a second- or third-line therapy or in patients with severe concomitant acne. 56
Alitretinoin has been evaluated in a single prospective uncontrolled study of 14 women receiving alitretinoin 10 mg/kg/d for 24 weeks. Overall, 78.5% of patients were reported to experience significant clinical improvement as assessed by mSS. 79
RCTs would be required in order to evaluate the real efficacy of oral retinoids, in as much as there are no studies comparing acitretin with isotretinoin.
Hormonal treatment
Perimenstrual exacerbations, rare postmenopausal occurrence, and improvement during pregnancy suggest that an endocrine influence for the disease, 80 but no relationship to serum and tissue hormone levels, has been found. 81 Patients with polycystic ovarian syndrome and HS may benefit from hormonal therapy, either alone as monotherapy in mild-to-moderate HS or in combination therapy for more severe disease. 56 RCTs are needed to define the role of hormonal treatment as an alternative or concomitant therapy together with antibiotics or biologics. 82 An RCT compared ethinylestradiol/noregestrel with ethinylestradiol and cyproterone acetate, both showing satisfactory clinical response. 83
Spironolactone 100 to 150 mg daily is also used. 56 Recently, some reports have been published on the benefits of metformin in HS, which have been attributed to its anti-androgen and anti-inflammatory effects.82,84 A phase III RCT with 65 patients is being conducted in order to evaluate the efficacy of metformin plus doxycycline versus doxycycline in monotherapy (NCT04649502). 85
Finasteride is a selective competitive inhibitor of type II 5-α reductase. Improvement of moderate-to-severe HS has been occasionally reported, but recurrences followed treatment cessation. 86 In a preliminary trial, clinical response was observed in six out of seven patients receiving finasteride (5 mg/d) as monotherapy after 8–24 months of treatment. 87 Finasteride has also been proposed as an alternative treatment in pediatric HS with appropriate tolerance and clinical response in a case series.88,89
Oral and intralesional corticosterds
Oral corticosteroids can produce pan-cytokine inhibition, 90 which agrees with the reported efficacy of systemic and intralesional corticosteroids in acute HS flares.91,92 Intralesional corticosteroids can lead to rapid resolution of inflammatory nodules.91,93 In a multicenter retrospective study, complete resolution of inflammatory and non-inflammatory lesions was observed in 95 lesions (70.37%) treated with intralesional corticosteroids (at variable dilutions and volumes). 94 An interventional prospective study evaluated the efficacy of intralesional ultrasound-guided injections of triamcinolone plus lincomycin, at baseline and after 2 weeks; clinical and symptomatic improvement was observed in 36 out of 37 patients at week 4. 95 However, the only RCT conducted with two different doses of intralesional triamcinolone (10 and 40 mg/ml) showed no statistical differences with placebo (intralesional normal saline). 96 Comparing the results of different studies is difficult due to the diversity of dosages and volumes used. It is not clear which is the most effective concentration. 97 An ongoing phase IV RCT including 200 patients aims to evaluate three different dosages of intralesional triamcinolone (10, 20, and 40 mg/ml) and find the optimal posology (NCT04582669). 98
High dose and protracted treatment with oral corticosteroids are not recommended since HS rapidly flares after tapering, but low-dose systemic prednisolone can be a valuable adjunct therapy for recalcitrant HS. 99 American guidelines recommend the use of prednisone pulses or multiweek tapers starting at 0.5 to 1 mg/kg daily as rescue therapy for flares or as a bridge to other long-term therapy; the effect is rapid and substantial, but side effects limit their prolonged use. 56
Surgery
Recommendations for the surgical management of acute HS lesions rely on low-quality, uncontrolled, retrospective reports. Incision and drainage of acute lesions provide a rapid relief of the symptoms, but recurrence rates are close to 100%. 100 Deroofing, with lower recurrence rates (20–40%), is adequate to treat localized lesions or all the lesions of one anatomical site in Hurley I–II stage. 101 Limited local excision consists in the excision of separate lesions with surgical margins; it is indicated for Hurley I–II HS and has similar recurrence rates to deroofing.101,102 Combination of deroofing with subsequent sinus tract excision enhances clinical results and decreases recurrence rates. 103 Wide excision is indicated for Hurley II–III HS and consists in the excision of large areas of involved skin with wide margins. 102 This technique is associated with lower recurrence rates. 100 The reconstruction strategy chosen after wide excision determines recurrence rates: 22% with primary closure, 11% with secondary intention healing, 2% with skin graft, and 2% with fasciocutaneous flaps. 104 Location of lesions can also predict clinical outcomes: perianal, vulvar, and inferior breast excisions have higher recurrence rates. 9
Prior medical treatment can improve surgical outcomes. Combination surgery with biologic treatment has demonstrated higher rates of cure. 105
Laser therapy
Laser and photodynamic therapy (PDT) have been used alone and in combination with other therapies with variable results. 106 Comparison between treatment modalities is challenging because there are no standardized treatment protocols using these devices and settings vary between machines. Larger randomized controlled trials are needed to elucidate their role and determine the optimal treatment settings. 107
Long-pulsed neodymium-doped yttrium aluminum garnet (Nd:YAG) laser (1064 nm) has shown clinical improvement 108 and diminution of inflammation in tissue biopsy specimens. 108 Carbon dioxide (CO2) laser (10,600 nm) has been used in combination with Nd:YAG or alone. 107 CO2 laser (fractional mode) used before Nd:YAG enhances the depth of penetration of the latter. 109 Ablative CO2 laser can be used to perform sinus deroofing or ablative destruction of lesions, 110 and is useful in treating anesthetic scars or contractures of chronic scars. 107 Alexandrite laser has shown promising results in case reports and case series. 107 An ongoing open-label study aims to evaluate the efficacy of Alexandrite hair removal laser in 20 patients with bilateral disease (axilla or groin). One side will be treated and the other one will serve as control (NCT03054155). 111
PDT has been associated with good clinical outcomes in several studies. The photosensitizers used in different concentrations include 5-aminolevulinic acid (ALA), methyl aminolevulinate (MAL), and methylene blue (MB). PDT has been performed following either topical (ALA, MAL, and MB) or intralesional (ALA and MB) application of the photosensitizing agent. Light sources also vary, including red light (635 nm), blue light, Intense Pulsed Light (630 nm), and laser diode (400 nm). 106 Response rates are not comparable between studies, but intralesional PDT seems to determine better outcomes and the axillary region has better response rates. 112
Photobiomodulation is also a useful tool for non-invasive treatment of HS. It has been reported to have beneficial effects on promoting wound healing, angiogenesis, vasodilation, and relieving from pain and inflammation in an in-vitro model mimicking HS disease. It has been proposed as an adjuvant third-line treatment for the management of HS. 113
Targeted biologic therapy
Table 4 summarizes the above-mentioned studies of biologic therapies.
Anti-TNF-α agents
Adalimumab. ADA is a fully human monoclonal antibody targeting soluble and transmembrane TNF-α. It is the only biologic approved for the treatment of moderate-to-severe HS in adults and adolescents by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA), based on the results of two phase III trials (PIONEER I and PIONEER II). 114 These double-blind, placebo-controlled studies enrolled 633 patients who received subcutaneous (sc) ADA 160 mg at week 0, 80 mg at week 2, and 40 mg weekly starting at week 4, or placebo. In PIONEER II, patients were permitted to continue treatment with antibiotics (tetracyclines) in stable doses. 104 The HiSCR with ADA was higher than with placebo at week 12 (50.6% versus 26.8%, p < 0.001, pooled efficacy from trials PIONEER I and II). 115 The Dermatology Life Quality Index (DLQI) score was also improved,115–117 and ADA was well tolerated with the expected adverse event (AE) profile. 115 Among the 88 patients who entered an open-label extension (OLE) study with ADA 40 mg weekly, HiSCR rates were 62.5% at week 36 and 52.3% at week 168. 116 ADA also reduced number and duration of flares, and lengthened flare-free intervals both in short- and long-term follow-up.118,119
Real-life data provided in a retrospective, multicenter cohort study showed ADA efficacy/safety and an inverse correlation between therapeutic delay and clinical response, supporting early ADA use and providing evidence for a ‘window of opportunity’ in HS treatment. 120 Real-life data provided in a retrospective cross-sectional study showed efficacy rates and improvement in DLQI rates comparable with previous trials. 121
ADA 40 mg weekly is more effective and offers more prevention of flaring than 40 mg every other week 122 and may be continued indefinitely. 116 Dose intensification to 80 mg weekly has been proposed for patients with insufficient response or with loss of efficacy after initial response to 40 mg/week, but larger studies are required to corroborate this observation. 123
Biosimilar ADA (SB5) has also been found to be effective, well tolerated, and interchangeable with originator ADA for HS treatment in a retrospective 36 weeks ‘real life’ observational study. 124
Calprotectin, fractalkine, and HCC-4 have been identified as potential predictive biomarkers of ADA response (86% predictive accuracy rate for ADA response). 125
The superior response to TNF-α blockade of subcutaneous nodules versus tunnels suggests that the formation of the latter is mediated by IL-17 rather than by TNF-α signaling. 53
Infliximab. Infliximab (IFX) is a chimeric monoclonal antibody targeting soluble and transmembrane TNF-α. 114 In a phase II randomized, double-blind study, 38 patients with moderate-to-severe HS received 5 mg/kg of iv IFX on weeks 0, 2, 4, 6, 14, and 22. At week 8, 57% of patients had a < 50% decrease of HSSI vs. 5% in the placebo group (p = 0.092). A post-hoc analysis showed that 60% of patients had a 25% to <50% decrease in HS HSSI compared with 5.6% of patients receiving placebo (p < 0.001). 126 IFX also reduced inflammatory markers as well as improved mean DLQI and visual analog scores (VAS) of pain. 126 The drug was well tolerated, and no safety issues were reported. 126
Doses higher than 5 mg/kg have been proposed. Oskardmay et al. 127 conducted a retrospective cohort study with 52 patients treated with IFX 10 mg/kg every 6 or 8 weeks, obtaining satisfactory results. Also, a prospective study concluded that starting IFX at 7.5 mg every 4 weeks, with possible dose escalation to 10 mg, provides optimal control of disease activity. 128 New prospective placebo- or active-agent-controlled phase III trials should be done to ascertain the eventual role of IFX in HS treatment. 129
In a recent retrospective cohort study, the efficacy of IFX versus its biosimilar infliximab-abda has been found to be clinically equivalent (HiSCR 71% versus 60% at week 10, p = 0.47). 130
In a practice cohort study, drug survivals of ADA and IFX in HS have been found to be similar and rather low (30.5% and 48.6% at 24 months); treatment interruption was predominantly determined by ineffectiveness and side-effects. 131
Certolizumab pegol. Certolizumab pegol (CZP) is a pegylated humanized monoclonal antigen-binding fragment of IgG, which binds to TNF-α. A retrospective study on off-label use of TNF-inhibitors reported no efficacy of low-dose CZP (200 mg every 2 weeks) in two patients. 132 Several case reports purport successful results of CZP 400 mg sc every 2 weeks133–136 in patients with moderate to HS refractory to other biologics.
Unlike other anti-TNF-α agents, CZP is not subject to active placental transfer and would be idoneous for the treatment of pregnant patients. 137 To date, there is only one report of successful treatment of HS with CZP during pregnancy in a patient with Hurley stage III HS. 136
Other TNF-α inhibitory agents. Etanercept is a recombinant human TNF-α receptor p75-Fc fusion protein that competitively binds membrane-bound TNF-α receptors. Only one phase II open-label, single-arm RCT of etanercept has been conducted, with no significant improvement in patient- or physician-reported outcomes. 138
Golimumab is a fully human anti-TNF-α monoclonal antibody that binds to soluble and membrane-bound TNF-α. Two case reports of golimumab treatment with HS have been published;139,140 it was successful only in one patient with concomitant pyostomatitis vegetans and silent ulcerative colitis who was treated with golimumab 200 mg followed by 100 mg every 4 weeks. 140
Anti-IL-17 agents
Serum levels of IL-17 have been found to be elevated in patients with HS compared with healthy controls, and to correlate with disease severity according to the Hurley stage. 50 This has led to investigate new therapeutic strategies, even though the relative contributions of the different isoforms of IL-17 (A, F, C, etc.) have not been completely elucidated.
Secukinumab. Secukinumab (SEC) is a human monoclonal immunoglobulin G1 kappa antibody that selectively binds to IL-17A. An open-label pilot trial included nine patients with moderate-to-severe HS who were administered SEC 300 mg sc weekly for 5 weeks, then every 4 weeks for 24 weeks; 67% (6/9) of patients achieved HiSCR. 141
A single-arm, open-label pilot trial included 20 HS patients, Hurley grades II–III, who received SEC 300 mg weekly for 5 weeks; then 9 patients were administered SEC 300 mg every 4 weeks, and 11 patients were treated with 300 mg every 2 weeks through week 24. Seventy percent (14/20) of all patients achieved HiSCR by week 24. 142
Similar results of the same protocol were observed in a retrospective study evaluating 20 Hurley IC - III HS patients previously refractory to antibiotics and anti-TNF-α (ADA or IFX): after 16 weeks, 75% (15/29) of patients achieved HiSCR and the response was maintained for an average of 14 months. 143 In two patients who developed Crohn’s disease during treatment, the drug was stopped and they were successfully treated with ustekinumab (UST) and IFX, respectively. 143 There is some concern about the risk of developing IBD with anti-IL-17 treatment in HS patients, who are already at higher risk of IBD. 144 In a recent Italian retrospective study of HS patients treated with psoriasis dosage of SEC, 13/31 (41%) of patients achieved HiSCR at week 28, and there was no report of IBD triggering or worsening. 145
Three phase III RCTs of SEC for the treatment of HS are currently ongoing (NCT03713632, NCT03713619, NCT04179175).146–148
SEC has been reported to induce HS in a patient with psoriasis, probably due to cytokine imbalance after treatment initiation. 149
Brodalumab. Brodalumab (BRO) is a monoclonal antibody that binds to the IL-17RA subunit of the IL-17 receptor dimer and blocks signaling of multiple isoforms of IL-17 (mostly IL-17A, IL-17C, and IL-17F). This may be important as each of these cytokines can drive neutrophilic inflammation, and the blockade of multiple isoforms might provide superior results to blockade of individual cytokines.
BRO has shown promising results in three case reports,133,150,151 and two phase I open-label trials have been conducted. An open-label cohort study included 10 patients with moderate-to-severe HS who were treated with BRO 210 mg sc at weeks 0, 1, and 2 and every 2 weeks thereafter until week 24. At week 12, all patients (10/10) achieved HiSCR (as early as week 2 in some), and 80% achieved IHS4 category change. The authors highlighted the rapid reduction of tunnel drainage and ultrasonographical signs of inflammation, usually refractory to other therapies. 152 However, two patients with extensive gluteal tunnels experienced relapses of drainage 1 week after each drug administration during the maintenance period (210 mg every 2 weeks). Thus, a subset of patients with severe disease and high proportion of sinus tracts might require higher doses of BRO. 152 This hypothesis was evaluated in another open-label study including 10 patients with draining tunnels and severe HS. BRO 210 mg weekly was administered for 24 weeks with good tolerance and safety profile. At week 12, 100% of patients achieved HiSCR, 80% achieved a 75% reduction in total AN count (HiSCR-75), and 50% achieved a 100% reduction (HiSCR-100). In contrast to the every 2-week dosing, cyclical disease suppression or recurrence in tunnel drainage was not observed with weekly dosing. 153
The efficacy of BRO in reducing drainage of sinus tracts is remarkable, since other therapies have been proven unsuccessful; 152 blockade of keratinocyte-derived IL-17C might provide a potential explanation.
Other anti-IL-17 agents. Bimekizumab is an humanized monoclonal antibody that potently and selectively neutralizes IL-17A and IL-17F. 154 A phase II RCT comparing bimekizumab with placebo including 90 patients has been recently published. Bimekizumab 640 mg was administered subcutaneously at week 0 and then 320 mg every 2 weeks during 10 weeks. At week 12, HiSCR was achieved in a 57.3% of patients in the bimekizumab group and 26.1% in the placebo group (95% credible interval for difference, 11.0–50.4%; posterior probability of superiority = 0.998). 155 Two phase III RCTs are being conducted to evaluate the efficacy and safety of bimekizumab for HS treatment (NCT04242446, NCT04242498).156,157
Ixekizumab is a humanized IgG4-type monoclonal antibody that binds with high affinity to soluble IL-17A and IL-17 A/F. There is scarce evidence of the efficacy of this drug for HS treatment; our literature review only found three recent case reports suggesting the potential usefulness of ixekizumab for HS.158–160
CJM112 is a novel fully human anti-IL-17A IgG1/κ monoclonal antibody that binds with similar affinity as ixekizumab to both human IL-17A and IL-17A/F. 161 A phase II RCT multicenter study in patients with moderate-to-severe HS has been completed to determine the efficacy and safety of multiple doses of CJM112 (NCT02421172). 162 At 16 weeks, the HS-PGA response rate was 32.3% (10/31) with CJM112, which was significantly superior to 12.5% (4/32) with placebo. The decrease in number of inflammatory lesions (abscesses, nodules, and fistulas) was 56% with CJM112 compared with 30% for placebo. 163
Anti-IL-12/23 agents
UST. UST is a human IgG1K monoclonal antibody that binds with high affinity to the p40 subunit of IL-12 and IL-23. These cytokines are thereby prevented from interacting with their IL-12Rb1 receptor protein, which is expressed on the surface of T cells and natural killer cells. 114 Certain genetic variations within the gene encoding the common IL-12bR1 subunit of the IL-12/IL-23 receptor have been shown to be associated with a more severe course of HS. 164
One phase II open-label study evaluated the efficacy of UST, as measured by mSS, in 17 patients with moderate-to-severe HS. The weight-based psoriasis dosage of UST was used at weeks 0, 4, 16, and 28, followed by an observation period until week 40. At week 40, improvement of mSS was marked in 35% of patients and moderate in 47%. A 47% of patients achieved HiSCR at week 40. Although the authors compared these results with those obtained in ADA RCTs, the high dropout rate in their study carries a significant risk of bias. 164
Response rates to UST have been variable in several case reports and small series.165–172 As in the study conducted by Blok et al., 164 psoriasis dosages have been used in most cases, but it is believed that higher doses (like those in Crohn’s disease) might be necessary to control HS. 164
A retrospective multicenter study evaluated HS treatment with iv infusions of UST adjusted by weight (⩽55 kg, 260 mg; 56–85 kg, 390 mg; ⩾86 kg, 520 mg), followed by subcutaneous maintenance dose of 90 mg every 8 weeks (the regime approved for Crohn’s disease) in 14 patients. Included patients had recalcitrant HS that had not responded to at least one prior biologic treatment. At 16 weeks, 50% of patients achieved HiSCR and a significant improvement of DLQI was reported in over 70% of patients. 173 A retrospective study including six patients treated with this regime obtained the same clinical response. 174 Moreover, in a retrospective study, HiSCR was achieved by 9/10 patients treated with UST 90 mg every 8 weeks (without induction dose). 175 Whether higher doses are more effective in HS requires further evaluation in RCTs.
Anti-IL-23 agents
Guselkumab. Guselkumab (GUS) is a human monoclonal antibody that targets the p19 protein subunit of extracellular IL-23. Six published case reports and retrospective case series have reported positive results treating recalcitrant HS with GUS 100 mg sc at weeks 0, 4, and then every 8 weeks.176–181 A case series reported poor results with higher doses of GUS (100 mg at weeks 0, 4, and then every 4 weeks): discrete improvement in two patients, no response in one patient, and worsening in one patient. 182 These variable results might be explained because most patients have severe disease refractory to other biologic therapies.
A phase II randomized, placebo-controlled, double-blind study evaluating the efficacy, safety, and tolerability of three different dosages of GUS in patients with moderate-to-severe HS has been completed, but its results have not yet been published (NCT03628924). 183
Other anti-IL-23 agents. Risankizumab is a humanized immunoglobulin G1 monoclonal antibody selective to the IL-23. Three publications report clinical response to risankizumab in four patients treated at psoriasis doses (150 mg sc at week 0, week 4, and every 12 weeks thereafter).184–186 A phase II, double-blind RCT to evaluate the safety and efficacy of two dose levels of risankizumab in adult patients with moderate-to-severe HS is being conducted (NCT03926169). 187
Tildrakizumab is a humanized monoclonal antibody that targets the p19 subunit of IL-23. Only a case series reports a successful clinical response in five patients receiving tildrakizumab 100 mg sc at weeks 0, 4, and 200 mg every 4 weeks thereafter. All patients demonstrated an improvement in AN count at week 8 compared with baseline and four patients reported improvement in DLQI. 188
Anti-IL-1 agents
Anakinra. Anakinra is a recombinant form of human IL-1 receptor antagonist (IL-1RA), and it competitively inhibits the interaction of both IL-1α and IL-1β with their receptor.
The efficacy of anakinra in the literature remains controversial. An open-label phase II trial including six patients with moderate-to-severe HS treated with daily anakinra 100 mg sc for 8 weeks demonstrated a significant mean decrease of 34.8 points in mSS and improvement of DLQI in five patients, but post-treatment rebound was observed in all patients during an 8-week follow-up period. 189 Moreover, in an RCT including 20 patients with Hurley stage II or III, HiSCR rate was 78% in patients receiving anakinra versus 30% in the placebo arm at week 12 (p = 0.04). However, after a 12-week post-treatment observation period, the HiSCR difference between groups was not significant. 190 Long-term efficacy and safety of anakinra was suggested in a small series of three patients with follow-up ranging from 6 months to 7 years, but all of them eventually relapsed and required a treatment switch to anti-TNF. 191 Additional case reports and case series alternate success192,193 with failure.139,194,195
Although the IL-1 pathway has been shown to be upregulated in HS, 44 the available evidence on anakinra together with frequent injection site reactions 189 make it less attractive than other potential therapeutic alternatives.
Bermekimab. Bermekimab (BER), also known as MABp1, is a recombinant human IgG1 monoclonal antibody that neutralizes IL-1α by binding it with high affinity. High concentrations of IL-1α in lesional skin 190 provide the basis for clinical development of BER as an HS treatment. Intravenous BER (7.5 mg/kg every 2 weeks) resulted in 60% of patients (6/10) achieving HiSCR versus 10% of patients (1/10) in the placebo group at 12 weeks. 196 Eight patients who had received placebo were then transitioned to open-label i.v. BER and 75% achieved HiSCR at week 12 of the OLE period. 197
An open-label phase II study evaluated the efficacy of weekly BER 400 mg sc in patients with moderate-to-severe HS who were naïve (18 patients) or had failed to anti-TNF therapy (23 patients). A 61% of anti-TNF naïve and 63% of anti-TNF failure patients achieved HiSCR at week 12. There was also a significant reduction in AN count [60% (p < 0.004) and 46% (p < 0.001)] and VAS pain score [64% (p < 0.001) and 54% (p < 0.001)] in anti-TNF naïve and in anti-TNF failure group, respectively, with no drug-related AEs with the exception of injection site reactions. 198
BER seems a promising first-line biologic treatment option for refractory moderate-to-severe HS as well as a second-line alternative for patients with failure to anti-TNF agents. 199
Canakinumab. Canakinumab is a human IgGκ monoclonal antibody targeting IL-1β and has shown positive200,201 and negative202,203 results in terms of efficacy in case reports; no RCTs are registered in www.clinicaltrials.gov.
Apremilast
Apremilast (APR) is an oral selective phosphodiesterase–4 (PDE-4) inhibitor. In a phase II RCT, 8/15 patients (53.3%) receiving APR 30 mg twice daily for 16 weeks achieved HiSCR compared with 0% in the placebo group (p = 0.055). 204 Four of the responders continued APR therapy, with maintenance of response after 2 years of treatment. 205 These findings contrast with those in an investigator-initiated trial that did not detect statistically significant changes in inflammatory markers in lesional skin of HS patients receiving APR compared with placebo, despite clinical improvement in the APR group. 206
Complement C5a inhibitors
IFX-1 is a monoclonal IgG4 kappa antibody that selectively binds to C5a and blocks its biological activity. In a phase II open-label trial, administration of IFX-1 800 mg iv on days 1, 4, 8, 15, 22, 29, 36, 43, and 50 was performed. Nine out of 12 patients (75%) achieved HiSCR at the end of treatment and 10/12 (83.3%) at the end of the 3-month follow-up period. 47 A phase II randomized placebo-controlled trial (NCT03487276) has been recently completed and has avaliable results. In total, 175 patients were randomized to receive double-blind treatment with placebo or four different doses of IFX-1 (400 mg every 4 weeks, 800 mg every 4 weeks, 800 mg every 2 weeks, and 1200 mg every 2 weeks). HiSCR achievement was achieved in 47.1%, 40.4%, 51.5%, 38.7%, and 45.5%, respectively. 207
Avacopan is an oral C5a receptor antagonist under development for treatment of HS, Antineutrophil cytoplasmatic antibodies-associated vasculitis, and atypical hemolytic uremic syndrome. A phase II RCT is currently ongoing (NCT03852472), 208 as well as a mechanistic study to examine the role of C5a receptors in HS (NCT04251663). 209
JAK inhibitors
Tofacitinib is a Janus kinase inhibitor that has been used with successful results and no safety concerns in two patients with Hurley III ulcerated HS resistant to other biologics. 210
INCB054707 is an orally administered Janus kinase 1 (JAK1) inhibitor under development for the treatment of HS. 199 Two recently completed phase II trials (NCT03569371, NCT03607487) have assessed the safety of this drug in 10 and 35 patients, respectively. In the NCT03607487 trial, patients were randomized to receive placebo or INCB054707 30, 60, or 90 mg. Preliminary results indicate that 80% of patients treated with 30 and 60 mg had grade 1–2 AEs. With the 90 mg dose, 50% of patients had grade 1–2 AEs and a 37% had grade 3 AEs. 211,212 Another phase II RCT including 200 patients and intending to assess drug efficacy is currently recruiting (NCT04476043). 213
A phase II randomized placebo-controlled trial with upadacitinib, another JAK inhibitor, is about to start promptly (NCT04430855). 214
Other molecules under development
Iscalimab (CFZ533) is a fully human anti-CD40 IgG1 monoclonal antibody that blocks the CD40–CD154 costimulatory pathway. 199 A phase II randomized, placebo-controlled trial assessing its efficacy and safety in HS treatment is currently recruiting patients (NCT03827798). 215
Spesolimab, a monoclonal antibody directed against the IL-36 receptor, which is under clinical development for pustular psoriasis and other diseases characterized by neutrophilic infiltration, is also being tested in HS patients (NCT04762277). 216
Ismidolimab (ANB019) is a monoclonal antibody directed against the IL-36 receptor, with a phase II RCT registered in www.clinicaltrials.gov (NCT04856930). 217
LY 3041658 is a monoclonal antibody that neutralizes chemokines that bind to the CXCR1 or CXCR2 receptors. It is being evaluated in a phase II randomized placebo-controlled study for HS (NCT04493502). 218
LYS 006 is an orally administered leukotriene A4 (LTA4) hydrolase inhibitor under development for the treatment of HS and inflammatory acne. Patients are being recruited in two phase II trials (NCT03827798 and NCT03497897).215,219
KT-474 is an oral small molecule that degrades the IL-1 receptor-associated kinase 4 (IRAK4) and is currently being evaluated for the treatment of interleukin-1 receptor (IL-1R)/TLR-driven immune-inflammatory diseases. A first-in-human study (phase I) evaluating safety, tolerability, drug pharmacokinetics and pharmacodynamics is currently in the recruitment phase (NCT04772885). 220
Several small molecules are currently being developed by Pfizer, aiming for oral treatment of HS and other inflammatory diseases. Patient recruitment is ongoing in a phase II, randomized, placebo-controlled 16-week study evaluating the safety and efficacy of PF-06650833, PF-06826647, and PF-06700841 in the treatment of 192 adults with moderate-to-severe HS (NCT04092452). 221 PF-06650833 is an IRAK4 inhibitor under development for the treatment of HS and rheumatoid arthritis. PF-06826647 is a tyrosine kinase 2 (TYK2) inhibitor under development for the treatment of HS, psoriasis, and ulcerative colitis. PF-06700841 is a TYK2/JAK1 inhibitor that prevents IL-12 and IL-23 signaling 199 and is being developed for the treatment of HS and psoriasis. 222
Biologic treatments for hidradenitis suppurativa.

sc, subcutanepus; po, oral; AN, abscess and nodule; CI, confidence interval; HiSCR, Hidradenitis Suppurativa Clinical Response; HS-PGA, Hidradenitis Suppurativa Physician’s Global Assessment; HSSI, Hidradenitis Suppurativa Severity Index; IFX, infliximab; LTA4, leukotriene A4; PDE-4, phosphodiesterase–4; RCT, randomized clinical trial.
Where are we now and where are we going?
To date, ADA is the only approved biologic treatment with extensive evidence on HS. The existence of a subset of patients with failure to ADA has derived in an intensive search for other molecules. The wide array of treatment options provides hope to those patients with advanced and treatment-refractory disease.
As shown in this review, a large amount of new molecules are being evaluated for HS treatment. As the pathogenesis of HS is becoming better known, it is logic to expect an increase in research of new molecules.199,223 However, the identification of potential drugs for HS has been based on preexistent drugs for other diseases (such as psoriasis) rather than in translational research based on HS pathogenesis. This would explain poorer results in RCTs compared with those in psoriasis; even though common inflammatory pathways are activated, those in HS might be wider and different. 19
Measurement of clinical outcomes in RCTs has also been subject to some criticism. On one hand, HiSCR counts the reduction in inflammatory abscess and nodules, but it does not consider draining fistulas of advanced disease. On the other hand, IHS4 considers nodules, abscesses, and draining fistulas, and thus may be a more representative outcome measure of HS. However, results in most RCTs are measured by HiSCR, which may lead to underestimation of response, since highly cicatricial disease can occur with low inflammatory nodule counts. 224 Extensive historical use of HiSCR determines the need of evaluating future studies by HiSCR in order to obtain comparable results, but a change (or supplementation) of treatment outcome measures used in clinical trials is highly advisable.
The cytokine cascade of HS appears complex and has been the main objective of research in recent years, but the mechanisms underpinning the initiation and progression of inflammation remain unknown. Although high serum and tissue levels of some cytokines have been detected, their specific blockade has not been leading to high rates of complete clinical response. This reaffirms the implication of genetic and environmental factors and suggests the presence of unidentified agents modifying disease activity or determining drug resistance. 19
Our ignorance of the exact pathogenesis of HS is compounded by its highly heterogeneous character, with different clinical presentations that have led to define different phenotypes of the disease. 225 These variants most likely represent the underlying pathogenetic heterogeneity of the disease. Also, clinically distinguished phenotypes have been shown to have different cytokine profiles, and thus would probably correspond to endotypes. 5 Whether better responses can be achieved with a particular cytokine inhibitor in a concrete phenotype or endotype has not been studied so far. 5
Furthermore, differences have been found between cytokine profiles in fistula drainage. Whether cytokines measured in pus secretion are predictors of treatment response with specific inhibitors is not known. 55
A crucial point is to start treatment early, before the disease progresses to fibrotic or clinically irreversible lesions. Efforts are being made to find disease biomarkers and to elucidate the factors of poor prognosis and early disease progression. This will help tailor treatment to HS patients.125,226
In the authors’ opinion, we are heading to a precision medicine approach with mediator-targeted therapies that will provide the most suitable treatment for HS depending on the predominant inflammatory pathway alteration. We are far from this objective nowadays, but hopefully it will be achieved in due course.
The main limitation of our review is potential bias in the selection of information sources; the search was extensive but not exhaustive, and not limited to randomized controlled trials. We did not intend to answer a specific research question with a meta-analysis, but to provide an expert review of the state of the art in HS treatment and the existing lines of research.
Conclusion
HS is a complex multifactorial disease that requires combination therapy, including lifestyle modifications, antimicrobial agents, hormonal therapy, surgery, and biologic therapy, if necessary. Due to the lack of effective treatments for moderate-to-severe HS, new therapeutic options are being studied, targeting specific cytokines involved in HS pathogenesis. Anti-IL-17 and anti-IL-1α inhibition seem to be promising therapeutic options for ADA-refractory moderate-to-severe HS. Nevertheless, head-to-head clinical trials are not available yet. Current investigations on HS biomarkers will hopefully lead to improved disease assessment, and further knowledge of the involved inflammatory phenomena and cytokine cascades/networks will lead to highly effective targeted precision therapy.
Footnotes
Author contributions
Dr. Victoria Amat-Samaranch and Dr. Eugènia Agut-Busquet contributed to the conceptualization of the article, drafted the initial manuscript, and reviewed the manuscript. Dr. Eva Vilarrasa and Dr. Lluís Puig made substantial contributions to the conception and design, and reviewed the manuscript for important intellectual content. All authors have approved the manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lluís Puig has perceived consultancy/speaker’s honoraria from and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Baxalta, Biogen, Boehringer Ingelheim, Celgene, Gebro, Janssen, JS BIOCAD, Leo-Pharma, Lilly, Merck-Serono, Merck Shsrp and Dohme (MSD), Mylan, Novartis, Pfizer, Regeneron, Roche, Sandoz, Samsung-Bioepis, Sanofi, and Union Chimique Belgue (UCB). Eva Vilarrasa has perceived consultancy/speaker’s honoraria from and/or participated in clinical trials sponsored by AbbVie, Almirall, Amgen, Bayer, Boehringer Ingelheim, Celgene, Gebro, Isdin, Janssen, Leo-Pharma, Lilly, Merck-Serono, MSD, Novartis, Pfizer, Roche, Sandoz, Sanofi, and UCB. Victoria Amat-Samaranch and Eugènia Agut-Busquet declare no conflicts of interest for this work. The Associate Editor of Therapeutic Advances in Chronic Disease is an author of this paper; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor had no involvement in the decision-making process.