
Abstract
Background:
Currently the global data on the glomerular filtration rate of healthy adults are insufficient, with relatively little data for other races and countries. Especially in China, there are no such figures.
Methods:
In this cross-sectional study, we included healthy Han adults in southern China. Participants completed a lifestyle and medical history questionnaire and had their blood pressure measured, and blood and urine samples collected. Serum creatinine was measured and used to estimated glomerular filtration rate (eGFR) by the Modification of Diet in Renal Disease (MDRD) and Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formulae. The normal range of eGFR is described, and the influence of gender and age on eGFR is analyzed by the statistical method.
Results:
We provided the largest sample size of eGFR research in China at present. The mean age of the 20,930 healthy individuals was 40.9 ± 12.3 years, 58.8% were women. The eGFRMDRD for women and men were 111.3 ± 17.4 mL/min per 1.73 m2 and 103.3 ± 15.9 mL/min per 1.73 m2, respectively. The eGFRCKD-EPI for women and men were 110.3 ± 12.1 mL/min per 1.73 m2 and 103.8 ± 13.3 mL/min per 1.73 m2, respectively. The eGFRMDRD of women and men in all age groups decreased continuously by 7.3 ml/min/1.73 m2/decade and 4.4 ml/min/1.73 m2/decade, respectively. The eGFRCKD-EPI of women and men in all age groups decreased continuously by 8.4 ml/min/1.73 m2/decade and 6.9 ml/min/1.73 m2/decade.
Conclusions:
The eGFR of women is higher than men and with the increasing age, the eGFR of women declines faster than men.
Introduction
Glomerular filtration rate (GFR) is defined as the total amount of ultrafiltrate produced by all glomeruli in both kidneys within 1 minute. It is considered to be the best overall indicator of kidney function in health and disease.1,2 However, GFR data for healthy adults around the world are insufficient, especially for the Chinese.
The gold standard for evaluating GFR is the measurement of inulin clearance, but this method is time-consuming and expensive, so it is not commonly used in clinical practice.3,4 As an alternative method, the National Kidney Foundation (NKF) recommends using an equation based on creatinine to estimate the GFR. 5 In China, two of the more popular GFR prediction equations are the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation 6 and an equation developed by adaptation of the Modification of Diet in Renal Disease (MDRD) equation on the basis of data from Chinese chronic kidney disease patients. 7 A study shows the CKD-EPI equation is believed to estimate GFR more accurately in healthy Asian people. 8
It is well known that adult GFR decreases with age, but the rate of decline is controversial.9,10 At the same time, some studies have shown that GFR may also be affected by gender, with women having either higher, 11 lower 12 or similar 10 GFR values compared to men. Therefore, there are still many contradictions regarding the influence of age and gender on GFR. At the same time, due to geographical and ethnic differences, the normal value of GFR of the Asian population is different from that of European and American countries. 13 Our study included 20,956 healthy Han adults from southern China, and obtained the reference range of age and gender-based estimated glomerular filtration rate (eGFR) for Chinese healthy adults for the first time.
Methods
Study participants
The research subjects were from healthy adults over 20 years old from the Han nationality in southern China. Inclusion criteria were: (a) age 20 years or older; (b) normal blood pressure (systolic blood pressure <140 mmHg, diastolic blood pressure <90 mmHg); (c) fasting blood sugar <7 mmol/L; (d) normal urine microscopic, blood, urine and biochemical analysis; (e) absence of any clinical history suggesting renal impairment. Exclusion criteria were: (a) obesity (body mass index ⩾28 kg/m2); (b) previous diabetes mellitus, hypertension, cardiovascular diseases, cerebrovascular disease, liver function damage, infectious disease, malignant tumors, kidney disease, gout or other life-threatening diseases; and (c) ethnic minorities other than the Han nationality. This study was approved by the regional ethics committee of the Second Affiliated Hospital of Nanchang University, and the approval number was no. (2016) 011. All participants gave written informed consent before data collection.
Study method
From July 2017 to September 2020, we adopted a multi-stage, stratified sampling method to obtain a representative sample of healthy people aged 20 years or over. We sampled six provinces (Guangdong, Jiangsu, Sichuan, Guangxi, Hunan, Jiangxi) proportionally from different geographical regions (southwest or southeast) in southern China. The survey divided all county (district)-level administrative units in these six provinces into four categories according to the level of economic development, namely, large cities, small and medium-sized cities, ordinary rural areas, and poor rural areas. In the first stage, three county (district)-level units were randomly selected from each province and each type of area, a total of 72 units. In the second stage, each unit used a method proportional to the population to draw six village (neighborhood) committees at equal intervals. In the third stage, according to the actual distribution of all households in each selected village (neighborhood) committee (building groups/village groups), each 15 households are divided into groups according to their geographical location, and the remaining groups are divided into groups with neighboring buildings or village groups. A group of households was organized so that all households were included in the sampling group; two groups were selected according to the simple random sampling method, and a total of 30 households were used as health survey households. A questionnaire was conducted on all family members, and a health check-up was performed after preliminary screening. There were 12,960 households in total, and this sample is representative of the southern region. Through the exclusion and inclusion criteria, 20,930 healthy people were finally included for eGFR data analysis.
With the help of general practitioners, nurses and medical students, all participants completed a questionnaire recording their general demographic data (e.g. age and sex), personal health and family history (e.g. hypertension, diabetes, cardiovascular, cerebrovascular diseases and so on), and lifestyle (e.g. smoking, drinking and exercise). After taking off shoes and thick clothes, each subject was measured with standard equipment, such as weight, height and waistline. Body mass index (BMI) is calculated as body weight (in kilograms) divided by height squared (in square meters), [BMI = weight (kg)/height2 (m2)]. 14 Elbow venous blood was collected for at least 10 hours on an empty stomach for determination of blood biochemical indexes, and the midstream urine of the first voiding in the morning was collected for albumin and creatinine analysis. The blood and urine samples were transported to the central laboratory of the Second Affiliated Hospital of Nanchang University for measurement. Before being tested, the blood samples were stored in the environment of −20°C, and the urine samples were stored in the environment of 4°C. All research investigators and staff were uniformly trained before the start of the survey to ensure that they master the correct methods of data collection.
When measuring blood pressure, after the subject sat quietly for 15 minutes, the researchers used a sphygmomanometer to measure the blood pressure of the left brachial artery three times every 5 minutes, and calculated the average of the three readings, unless the difference in the readings was greater than 10 mmHg. In that case, the average of the two closest measurements would be used. Hypertension was defined as systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg, or taking any antihypertensive medications in the past 2 weeks or any self-reported history of hypertension. Fasting blood glucose was determined by a glucose oxidase enzymatic method. Participants with fasting plasma glucose ⩾7.0 mmol/L or any oral hypoglycemic agents or any self-reported history of diabetes were classified as diabetes.
Urinary albumin and creatinine were detected from a fresh morning urine sample stored at 4°C for less than one week. Urinary albumin was determined by immunoturbidimetry. Urinary creatinine was measured via Jaffe’s kinetic method on a Hitachi 7600 autoanalyzer (Hitachi, Tokyo, Japan). The ratio of urinary albumin to creatinine (ACR; mg/g creatinine) was calculated, and patients with an ACR greater than 30 mg/g were considered to having albuminuria.
Serum total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, and uric acid were measured with a Hitachi 7600 automatic analyzer (Hitachi, Tokyo, Japan).
Method of GFR estimation
Serum creatinine was measured via Jaffe’s kinetic method on a Hitachi 7600 autoanalyzer (Hitachi, Tokyo, Japan). eGFR was calculated with the Chronic Kidney Disease Epidemiology Collabora-tion (CKD-EPI) equation 6 and an equation developed by adaptation of the Modification of Diet in Renal Disease (MDRD) equation on the basis of data from Chinese chronic kidney disease patients. 7
The eGFRMDRD was calculated according to the formula:
eGFR (mL/min per 1.73 m2) = 175 × Scr−1.234 × age−0.179 (if female, × 0.79)
The eGFRCKD-EPI was calculated according to the formula:
Female eGFR (mL/min per 1.73 m2) = 144 × (Scr/0.7)−0.329 × (0.993)Age (if Scr ⩽0.7 mg/dL) eGFR (mL/min per 1.73 m2) = 144 × (Scr/0.7)−1.209 × (0.993)Age (if Scr >0.7 mg/dL)
Male eGFR (mL/min per 1.73 m2) = 141 × (Scr/0.9)−0.411 × (0.993)Age (if Scr ⩽0.9 mg/dL) eGFR (mL/min per 1.73 m2) = 141 × (Scr/0.9)−1.209 × (0.993)Age (if Scr >0.9 mg/dL)
where Scr is serum creatinine concentration (in mg/dL) and age in years.
Statistical analysis
The main goal of the analysis is to determine the reference values of eGFR based on age and gender. The results were expressed as mean ± standard deviation or median (range or interquartile range). The Kolmogorov–Smirnov (K–S) test was employed to evaluate the distribution of variables. For men and women, all calculations were performed separately. The Mann–Whitney test was used to determine whether there were significant differences in eGFR values between men and women in different age groups. The unpaired Student’s t-test was used to determine whether there was a significant difference in the rate of decline of eGFR per decade between men and women of different age groups. In addition, one-way analysis of variance (ANOVA) and post-analysis (Bonferroni test) was applied to determine whether there was a significant difference in the rate of decline of eGFR per decade between male and female age groups. Pearson’s correlation test was used for the correlation between variables. Simple and multivariate regression analyses were employed to assess the effect of age and gender on eGFR (dependent variable). All statistical analyses were performed using SPSS 24.0 software, and p-value <0.05 was considered as statistically significant.
Results
A total of 20,930 healthy adults of Han nationality in southern China were included for evaluation, providing the largest sample size in China at present. Among them, women were 12,297 (58.8%), the mean age was 40.4 ± 11.4 years (range 20–88), men were 8633 (41.2%), and the mean age was 41.6 ± 13.5 years (range 20–89). The mean eGFRMDRD for women and men were 111.3 ± 17.4 mL/min per 1.73 m2 (range 64.1–150.0 mL/min per 1.73 m2) and 103.3 ± 15.9 mL/min per 1.73 m2 (range 60.1–150.0 mL/min per 1.73 m2), respectively. The mean eGFRCKD-EPI for women and men were 110.3 ± 12.1 mL/min per 1.73 m2 (range 61.3–135.2 mL/min per 1.73 m2) and 103.8 ± 13.3 mL/min per 1.73 m2 (range 54.7–132.8 mL/min per 1.73 m2), respectively. The mean eGFR of women was greater than that of men. There was significant difference in mean eGFR obtained by the MDRD and CKD-EPI formulae between women and men, with a p-value of <0.05.
After stratifying data by age decades, the mean, standard deviation and median of eGFRMDRD and eGFRCKD-EPI for men and women in different age groups are shown in Table 1, respectively. The interquartile range of eGFRMDRD and eGFRCKD-EPI for men and women at different ages are shown in Figure 1, respectively. In every age group, the mean eGFR of women is higher than that of men. Except for the mean eGFRMDRD value of people 60–69 years and over 70 years of age with no significant difference between men and women (p = 0.074 and p = 0.902, respectively), there were significant differences among other age groups, with a p-value of <0.05. The mean value of eGFRCKD-EPI was significantly different between men and women in each age group, p-value <0.05. In general, eGFR of women was higher than that of men, with statistical differences.
eGFR values by MDRD and CKD-EPI formulae according to gender in different age groups.

CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; eGFR, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease.

The interquartile range of estimated glomerular filtration rate (eGFR) by MDRD and CKD-EPI formula for each age group (Panel A: females eGFRMDRD; Panel B: males eGFRMDRD; Panel C: females eGFRCKD-EPI; Panel D: males eGFRCKD-EPI).
Figure 2 shows the median eGFR by age group in women and men separately. Through one-way ANOVA and post-analysis (Bonferroni test), there was no difference in the decrease of eGFR between groups younger than 40, 40–60 and older than 60 years. The eGFRMDRD of women and men in all age groups decreased continuously by 7.3 ml/min/1.73 m2/decade and 4.4 ml/min/1.73 m2/decade, respectively, with statistically significant differences (p < 0.001). The eGFRCKD-EPI of women and men in all age groups decreased continuously by 8.4 ml/min/1.73 m2/decade and 6.9 ml/min/1.73 m2/decade, respectively, with statistically significant differences (p < 0.001). In the analysis, it was found that there was no difference in the decrease of eGFR between men and women in the age groups less than 40 years old and more than 60 years old (p > 0.1), while the decrease of eGFR in women between 40 and 60 years old was faster than that in men, with a significant difference (p < 0.001).

Differences in the median estimated glomerular filtration rate (eGFR) with age group per decade between men and women in the study (Panel A: MDRD; Panel B: CKD-EPI).
There was a significant inverse correlation between age and eGFRMDRD in women and men (r = −0.436 and r = −0.377, p < 0.01, respectively). There was a significant inverse correlation between age and eGFRCKD-EPI in women and men (r = −0.770 and r = −0.696, p < 0.01, respectively). Simple linear regression analysis confirmed the effect of age between different genders on eGFR (Figure 3). Figures 3 and 4 show the relationship between age and eGFR for all patients in the form of graphs and equations. Figure 3 shows the linear equation and 95% confidence interval (CI) of age between different genders on eGFR. Figure 4 shows the cubic equation and 95% CI of age between different genders on eGFR. The sample size of female participants over 80 years of age was small, and there was an error in representing the total eGFR with a small number of individuals [Figure 4(a) and (c)]. There is a good linear relationship between male GFRCKD-EPI data and age [Figures 3(d) and 4(d)]. eGFRCKD-EPI data have a greater correlation with age and a smaller dispersion degree than eGFRMDRD data, which may indicate that the CKD-EPI formula is more suitable for Chinese people.

Scatter plot of estimated glomerular filtration rate (eGFR) by MDRD and CKD-EPI formula against age for healthy adults (Panel A: females eGFRMDRD; Panel B: males eGFRMDRD; Panel C: females eGFRCKD-EPI; Panel D: males eGFRCKD-EPI). The central straight-line shows the best-fitting equation, the upper and lower boundaries are 97.5th and 2.5th percentiles.
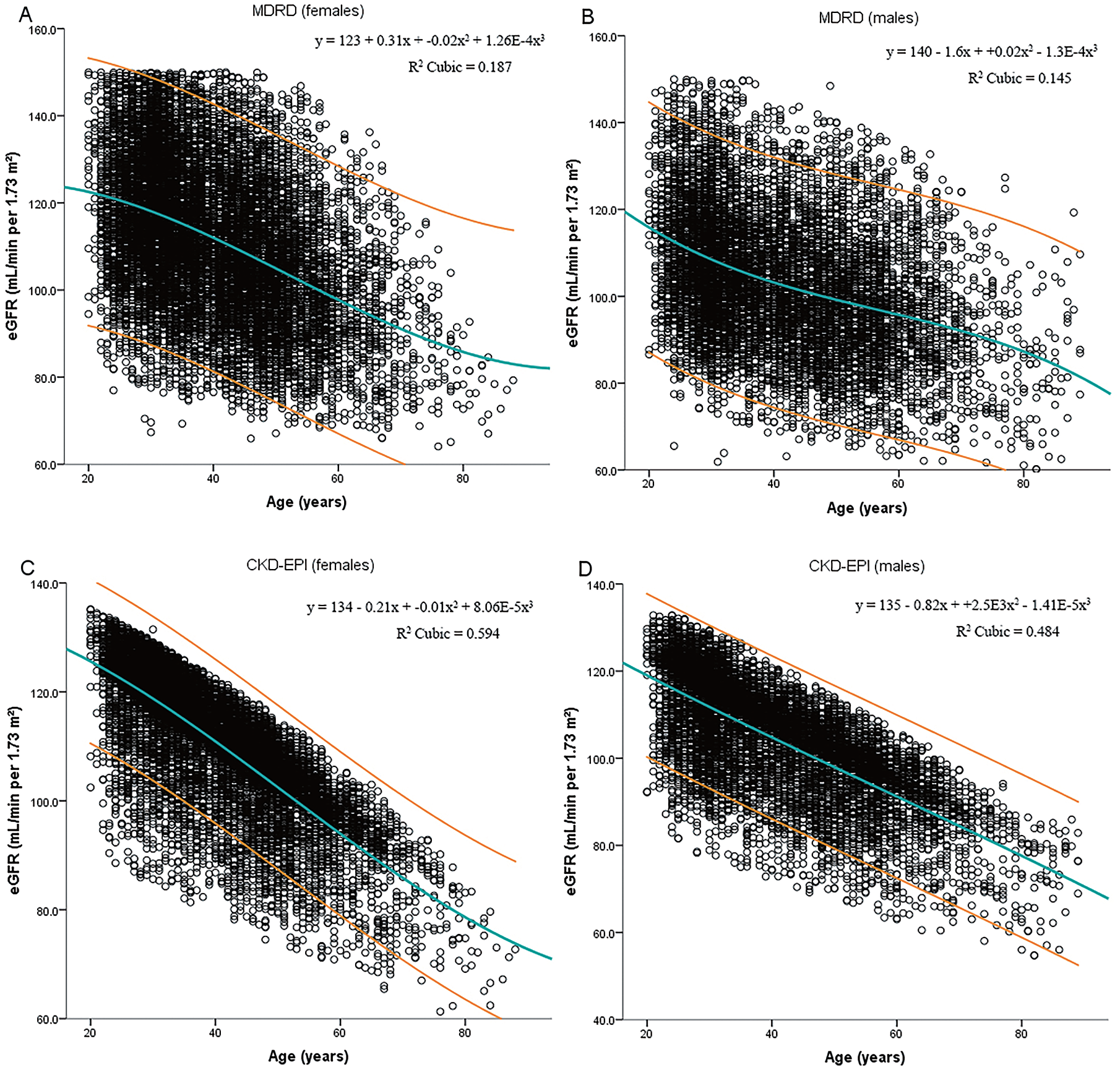
Scatter plot of estimated glomerular filtration rate (eGFR) by MDRD and CKD-EPI formula against age for healthy adults (Panel A: females eGFRMDRD; Panel B: males eGFRMDRD; Panel C: females eGFRCKD-EPI; Panel D: males eGFRCKD-EPI). The central cubic curve shows the best-fitting equation, the upper and lower cubic curve are 97.5th and 2.5th percentiles.
Discussion
This study is to the best of our knowledge the largest published series to date of eGFR in a healthy Chinese population. Previous studies recommended the use of age and gender reference limits to measure renal function, as using a uniform reference limit independent of age and gender may lead to inaccurate classification of renal function.15–17 Based on a large-scale population study, we obtained the first reference values for eGFR in healthy Chinese adults of a specific age and gender.
In our study, the mean eGFRMDRD in women and men was 111.3 mL/min/1.73 m2 and 103.3 mL/min/1.73 m2, and the eGFRCKD-EPI was 110.3 mL/min/1.73 m2 and 103.8 mL/min/1.73 m2, respectively. The results of this study seem to be lower than the reported value of 109–129 mL/min/1.73 m2 in the western population,3,11,18–21 but it seems to be higher than the reported 103 mL/min/1.73 m2 of healthy people in West Africa 22 and the reported 81.4 mL/min/1.73 m2 of potential adult kidney donors in India, 13 consistent with the results of a previous Chinese report. 23 This difference might be due to differences in dietary intake among ethnic groups living in different regions, differences in age and gender distribution in different studies, and differences in GFR measurement and estimation methods.24,25
At present, most of the published literature has found no significant difference in GFR values between men and women,3,10,13,19,26–28 and a few studies have found that men have higher GFR,12,26 this is contrary to our findings. In our study, except for the age group 60–69 years and over 70 years old, the mean value eGFRMDRD of women in other age groups was higher than that of men, while the mean value eGFR of women in all age groups of eGFRCKD-EPI was higher than that of men. This is different from the results of most previous studies, probably because the participants in these studies were potential kidney donors and the sample size was relatively low,3,10,26,27 while our study provided the largest sample size in China and the included volunteers were picked from healthy people. This approach tends to minimize selection bias, because donors are mostly relatives of kidney recipients and may have a higher proportion of unidentified kidney diseases. 3 Therefore, this study used a sample composed entirely of healthy people, and the results are suitable to provide a reference value. Meanwhile, in 2005, Barai et al. 13 published mean GFR results in 610 healthy potential Indian kidney donors using the 99mTc-DTPA (diethylenetriamine pentaacetic acid) two-plasma sample method of Russell. He found that in the 40–45-year age group, the mean GFR of women was higher than that of men, and the difference was significant. In 2009, Poggio et al. 11 found higher mean GFRs in African-American (AA) women compared with AA men. In the following year, a Chinese study 23 showed that the mean GFR of women was higher than that of men in the 18–29-year age group. These studies all indirectly support our findings. Next, it seems necessary to conduct more research to explain and prove the differences between healthy men and women.
Published studies consistently show that GFR declines with age in healthy individuals, and it has been demonstrated that aging is also associated with a decline in other physiological parameters, such as renal blood flow, and with structural changes such as a reduction in nephron number, glomerulosclerosis, and tubulointerstitial fibrosis.26,29,30 However, most studies failed to confirm any gender differences in age-related decline in GFR,10,27,28,31 but our research found a continuous linear decline in eGFR with age, and a more rapid decline in women. We found that the eGFRMDRD of women and men in all age groups decreased continuously by 7.3 ml/min/1.73 m2/decade and 4.4 ml/min/1.73 m2/decade and the eGFRCKD-EPI of women and men in all age groups decreased continuously by 8.4 ml/min/1.73 m2/decade and 6.9 ml/min/1.73 m2/decade, respectively. In the analysis, it was found that the decrease of eGFR in women between 40 and 60 years old was faster than that in men, with a significant difference. This is consistent with the results of previously published studies.23,32,33
Several theories have been put forward to explain the more rapid GFR decline seen in women. First, it has been suggested that young adult women may have a higher GFR than men, which is masked by the proportion of body surface area (BSA), which may lead to a faster decline in eGFR, similar to hyperfiltration-related renal pathology. 34 Second, with the increase of the age of healthy individuals, the renal function is preserved, but the renal function reserve decreases gradually. 35 Men may have a higher reserve of renal function to compensate for the accumulation of sclerosing glomeruli during aging. Previous studies have shown that healthy men have a greater ability than women to maintain their GFR by increasing filtration fraction. 36 Thirdly, as women age, the impact of estrogens on renal hemodynamics and structure disappear as estrogen levels gradually decline, even before the menopause.37–39 There is no evidence that this faster rate of decline in women is harmful to their health.
The advantage of this study is its large scale, which increases the universality of our reference range. However, there are some limitations to our study. Using serum creatinine to estimate GFR may underestimate the normal value of GFR. 11 There are relatively few individuals over the age of 80 years, and this is to be borne in mind when interpreting our eGFR reference ranges in this age group. Our data are cross-sectional rather than longitudinal. The change in eGFR with age that we describe is the change in mean eGFR at the population level.
Conclusion
Based on a large-scale population study, we obtained the first reference values for eGFR in healthy Chinese adults of a specific age and gender. We found that the eGFR of women was higher than men and eGFR decreased continuously with the increase of age, and the decline rate of eGFR of women was faster than men. Our research shows that gender and age are important factors in determining the normal glomerular filtration rate in healthy adults.
Footnotes
Acknowledgements
YM performed the data collection, analysis, reviewed articles, and wrote the manuscript. JZ revised the manuscript and GX designed the study. All the authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was supported by the National Natural Science Foundation of China (No. 81970583 and No. 82060138), the Nature Science Foundation of Jiangxi Province (No. 2020BABL206025), and the Projects in the Second Affiliated Hospital of Nanchang University (No. 2019YNLZ12008).
Conflict of interest statement
The authors declare that there is no conflict of interest.