
Abstract
Background:
The aim of this study was to investigate whether physical activity, sarcopenia, and anemia are associated an with increased risk of tuberculosis (TB) among the older population.
Methods:
We included 1,245,640 66-year-old subjects who participated in the National Screening Program for Transitional Ages for Koreans from 2009 to 2014. At baseline, we assessed common health problems in the older population, including anemia and sarcopenia. The subjects’ performance in the timed up-and-go (TUG) test was used to predict sarcopenia. The incidence of TB was determined using claims data from the National Health Insurance Service database.
Results:
The median follow-up duration was 6.4 years. There was a significant association between the severity of anemia and TB incidence, with an adjusted hazard ratio (aHR) of 1.28 [95% confidence interval (CI), 1.20–1.36] for mild anemia and 1.69 (95% CI, 1.51–1.88) for moderate to severe anemia. Compared with those who had normal TUG times, participants with slow TUG times (⩾15 s) had a significantly increased risk of TB (aHR 1.19, 95% CI, 1.07–1.33). On the other hand, both irregular (aHR 0.88, 95% CI 0.83–0.93) and regular (aHR 0.84, 95% CI, 0.78–0.92) physical activity reduced the risk of TB. Male sex, lower income, alcohol consumption, smoking, diabetes, and asthma/chronic obstructive pulmonary disease increased the risk of TB.
Conclusion:
The risk of TB among older adults increased with worsening anemia, sarcopenia, and physical inactivity. Physicians should be aware of those modifiable predictors for TB among the older population.
Introduction
The world is now facing an aging-related health burden. In 2010, about 8% of the world’s population was 65 years or older, and this number is expected to reach 16% of the world’s population by 2050. 1 Accordingly, almost all countries in the world are facing or will likely soon face a dramatic increase in their proportion of older adults with illness. Although noncommunicable diseases are a major disease burden among the 60-years-and-over population, the disease burden associated with infectious diseases in this sub-population cannot be dismissed; older people tend to have one or more chronic diseases and are therefore vulnerable to infectious diseases. 2
Tuberculosis (TB) remains a deadly communicable disease and a major health burden worldwide, as one of the leading causes of death from a single infectious etiology. 3 In the current era of population aging, effective strategies for TB control are especially important in order to improve public health, as aging is one of the most important nonmodifiable risk factors for TB. In addition, the older population has many comorbidities and socioeconomic factors associated with an increased risk of TB. 4 The treatment outcomes for TB in older patients are also poorer compared with the younger population. 4 However, unfortunately, despite the importance of TB in the older population, current global TB control programs or policies may not be sufficient to lower the disease burden in older adults. 5 Thus, there is an urgent need to elucidate modifiable risk factors for TB in this population.
An estimated 17% of people aged 65 years and older have been found to be anemic. 6 Anemia is a result of the most common micronutrient deficiency (iron), which may predispose an individual to certain infectious diseases. 7 Although the relationship between anemia and the risk of contracting TB remains unclear, individuals with anemia are more susceptible to infections, probably due to impaired cell-mediated immunity. 8 In one study, the incidence of TB was greater in the iron-deficiency anemia group, 8 but the analyses did not consider socioeconomic status, alcohol consumption, smoking, body mass index (BMI), or anemia severity.
Physical activity, muscle mass, and strength all decline with age, particularly after 50 years of age. The prevalence of sarcopenia, which is defined as the loss of muscle mass and function, was reported to be approximately 10% among healthy adults aged ⩾60 years. 9 Because sarcopenia is associated with physical performance, a physical test may be used to evaluate reductions in mobility among older adults. In particular, the timed up-and-go (TUG) test is a simple test that is well correlated with the risk of sarcopenia in the older population.10,11 While sarcopenia is known to be a critical factor not only in aging but also in a variety of chronic diseases, including respiratory diseases, 12 the association between sarcopenia and TB incidence has not been evaluated. In addition, the major cause of sarcopenia is insufficient physical activity and lack of exercise with advancing age. 13 Nevertheless, there have been few studies addressing the relationship between physical activity and TB incidence in the older population.
Therefore, in the present study, using data from a large population in Korea, we aimed to investigate the predictors for TB incidence among older adults. In addition, to focus on common modifiable health concerns of the older population, anemia, sarcopenia (as measured by the TUG test), and physical activity were considered.
Methods
Study setting
The Korean National Health Insurance Service (NHIS) is a mandatory universal public health insurance system that covers approximately 97% of the population, except for the 3% of Korean residents who are Medicaid beneficiaries. The NHIS database contains information regarding a patient’s use of medical facilities, including the International Classification of Diseases 10th Revision (ICD-10) codes and prescribed medicines from outpatient clinics and hospitalization. The NHIS also collects sociodemographic information (e.g. age, sex, place of residence, and income level). The NHIS data have been widely used in epidemiologic studies. 14
Since 2007, the NHIS has also provided the National Screening Program for Transitional Ages (NSPTA) to 66-year-old participants free of charge. The NSPTA program consists of health behavior (i.e. smoking status, alcohol consumption, physical activity, and past medical history), anthropometric measurements (i.e. BMI and blood pressure), laboratory tests (i.e. hemoglobin), and comprehensive geriatric assessment, including assessment of physical function (i.e. TUG test) and mental/cognitive function. 15
Study population
The present study initially included 1,551,771 participants aged 66 years who underwent the NSPTA between 2009 and 2014. We excluded individuals who had any registered disabilities (n = 237,686) and for which information for at least one variable was missing (n = 26,712). Moreover, individuals who had a diagnosis of TB (n = 3123), anemia (n = 4807), cancer (n = 33,606) or end-stage renal disease (n = 197) prior to the health screening date were excluded. A total of 1,245,640 individuals were included in the final analyses. The cohort was followed from baseline to the date of incident TB or death, or until the end of the study period (31 December 2018), whichever came first (Figure 1).

Flowchart of the study population.
This study was approved by the Institutional Review Board (IRB) (IRB File No. SMC 2019-04-132). The IRB waived the requirement for written informed consent because the data are public and anonymized under confidentiality guidelines.
Definition of tuberculosis
The main study outcome was incident active TB during the follow-up period. From the year 2005, Korea’s NHIS has provided a special copayment reduction program for all patients diagnosed with active TB to decrease the burden of TB in the nation. Specific insurance codes (V000, V206, and V246) are required to be applied to patients with active TB after confirmation of their diagnosis, and TB patients then receive free TB-related medical care. Because the NHIS database contains complete information regarding insured medical services throughout the country, the claims database enabled us to review all patients with active TB in the nation by means of their unique insurance codes. 16
Anemia
Serum hemoglobin concentration was measured using the cyanmethemoglobin method. Anemia was defined according to World Health Organization criteria as hemoglobin <12 g/dL for women and <13 g/dL for men. The severity of anemia was categorized as mild (hemoglobin ⩾11 g/dL), moderate (hemoglobin 8–10.9 g/dL), or severe (hemoglobin <8 g/dL).
Timed up-and-go test
The TUG test was used to predict sarcopenia among the study population. As part of the NSPTA program, the TUG test was conducted on the examination day at each community clinic or hospital. 17 The subjects were observed and timed while rising from an armchair, walking 3 m, turning, walking back, and sitting down again. 17 The subjects were instructed to wear regular footwear and use their customary walking aid. 17 Many different cut-offs for TUG times have been suggested in the previous studies. 18 For the analyses, the TUG test results were categorized into three groups: <10 s, 10–15 s, and ⩾15 s after considering the distribution of the TUG results.
Physical activity
Based on the results from the self-administered questionnaire, the subjects were classified according to physical activity: none, irregular, and regular physical activity. Regular physical activity was defined as performing >30 min of moderate physical activity at least 5 times per week or >20 min of strenuous physical activity at least 3 times per week. Those who exercised but did not meet the criteria for regular physical activity were included in the irregular physical activity group.
Covariates
Covariates were selected based on background clinical knowledge and data availability.19,20 The determination of income level was based on monthly insurance premiums because insurance contributions are determined based on income level and not on health risk in Korea. Smoking status was classified into never, former, and current smokers. Based on daily alcohol consumption, the subjects’ rate of alcohol consumption was classified as none (0 g/day), moderate (<30 g/day), and heavy (⩾30 g/day). BMI (kg/m2) was calculated as the subject’s weight in kilograms divided by the square of the subject’s height in meters, and the resulting BMI values were classified into five categories according to the Asia-Pacific criteria of the World Health Organization; underweight (<18.5 kg/m2), normal (18.5–23 kg/m2), overweight (23–25 kg/m2), obese (25–30 kg/m2), and severely obese (⩾30 kg/m2). We used the Modification of Diet in Renal Disease equation to calculate the glomerular filtration rate (GFR) values, which were categorized as <30, 30–60, ⩾60 mL/min/1.73 m2. The following comorbidities were included in the analyses: diabetes mellitus (DM, E10–E14 and antidiabetic medication), ischemic heart disease (I20–I25), stroke (I63–I64), and pulmonary disease [asthma (J45–J46 and use of asthma drugs) and chronic obstructive pulmonary disease (COPD, J43–J44, except for J430 and use of COPD drugs)].
Statistical analyses
Baseline characteristics of individuals with incident TB were compared with those without incident TB, using a two-tailed Student’s t-test for continuous variables and a chi-squared test for categorical variables. The incidence rate of primary outcomes was calculated by dividing the number of incident cases by the total follow-up duration (1000 person-years). A Kaplan–Meier (KM) failure time plot was used to describe the incidence of TB according to the severity of anemia and TUG test impairment. Multivariable proportional hazards model included sex, income level, smoking status, alcohol consumption, physical activity, BMI, anemia, GFR, TUG test, DM, ischemic heart disease, stroke, and pulmonary disease. Sensitivity analyses were also performed by excluding subjects with TB occurring within 1 year of follow-up to account for the possibility of reverse causation. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA), and a p-value < 0.05 was considered to indicate statistical significance.
Results
Baseline characteristics
The age of each subject at entry into the study was 66 years, and the study population included 558,387 (44.8%) men (Table 1). During the median follow-up period of 6.4 years (interquartile range 5.0–8.1), there were 9344 new cases of TB and the incidence rate was 1.15 per 1000 person-years. Individuals with incident TB were more likely to be men, current smokers, heavy alcohol drinkers, physically inactive, and have a lower BMI, hemoglobin, GFR, and slower TUG test time compared with those without incident TB. They also were more likely to have a higher prevalence of anemia, DM, stroke, and pulmonary disease compared with those without incident TB.
Baseline characteristics of study subjects.

Data are expressed as the means ± SD, or n (%).
BP, blood pressure; GFR, glomerular filtration rate; PY, pack-years; TUG, timed up-and-go.
Predictors for TB among older adults
Compared with women, men had a significantly greater risk of TB [adjusted hazard ratio (aHR) 1.66, 95% confidence interval (CI) 1.57–1.75; Table 2]. The subjects in the highest income quartile had a lower TB risk than those in the lowest quartile (aHR 0.90, 95% CI 0.85–0.95).
Hazard ratios and 95% confidence intervals for tuberculosis incidence.
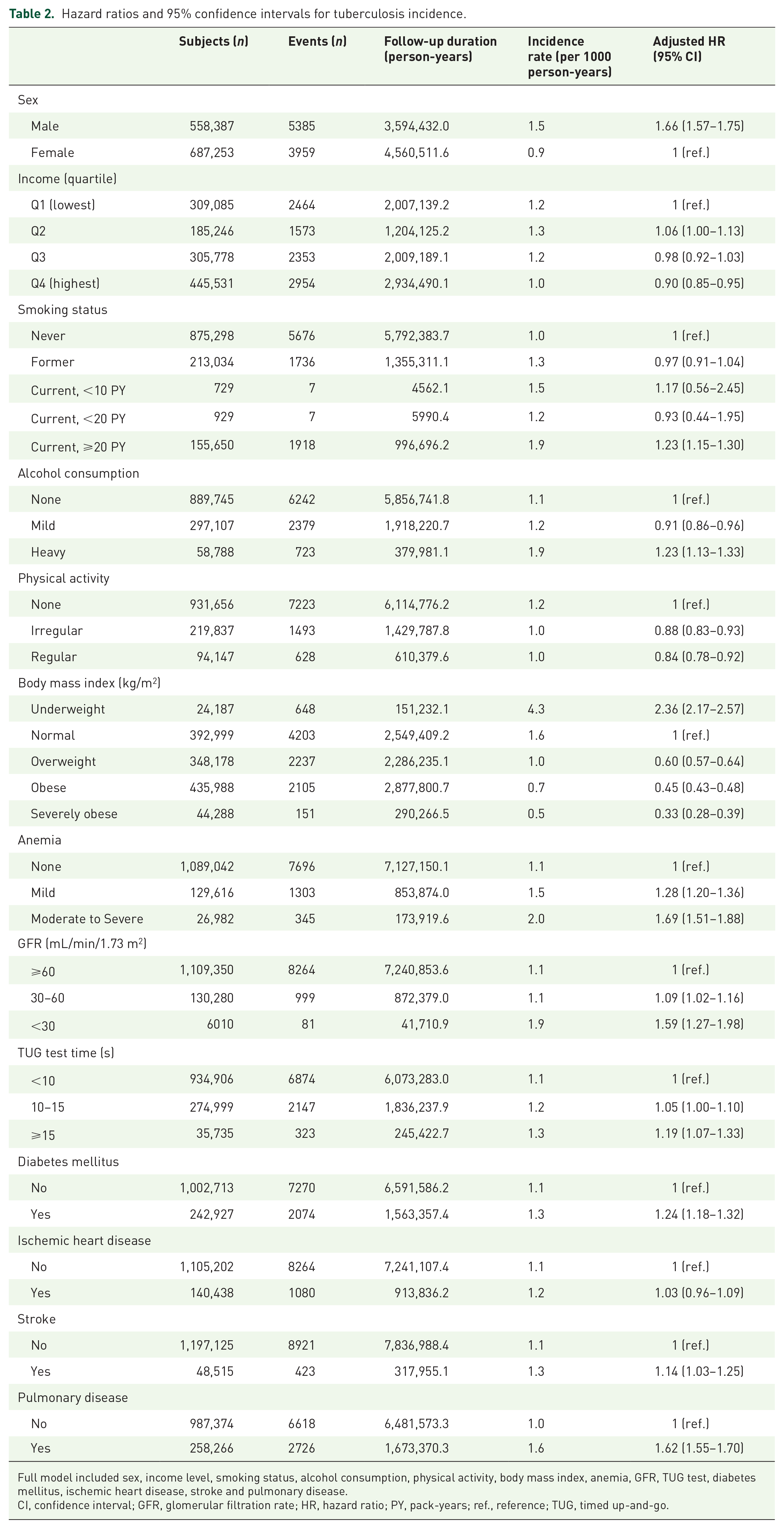
Full model included sex, income level, smoking status, alcohol consumption, physical activity, body mass index, anemia, GFR, TUG test, diabetes mellitus, ischemic heart disease, stroke and pulmonary disease.
CI, confidence interval; GFR, glomerular filtration rate; HR, hazard ratio; PY, pack-years; ref., reference; TUG, timed up-and-go.
Anemia and TB
There was a significant association between the severity of anemia and TB incidence, with an aHR of 1.28 (95% CI 1.20–1.36) for mild anemia and 1.69 (95% CI 1.51–1.88) for moderate to severe anemia.
Sarcopenia and TB
Compared with those who had normal TUG times (<10s), subjects with slow TUG times (⩾15 s) had a significantly increased risk of TB (aHR 1.19, 95% CI 1.07–1.33).
Physical activity and TB
Physical activity was associated with lower TB risk. When compared with subjects who reported no physical activity, the aHR was 0.88 (95% CI 0.83–0.93) for those who reported engaging in irregular physical activity, and 0.84 (95% CI 0.78–0.92) for those who engaged in regular physical activity.
Other TB predictors
Current smokers with 20 or more pack-years (aHR 1.23, 95% CI 1.15–1.30) and heavy alcohol drinkers (aHR 1.23, 95% CI 1.13–1.33) had greater TB risks than those who never smoked or drank. Being underweight was associated with an increased risk of incident TB as compared with the normal BMI group (aHR 2.36, 95% CI 2.17–2.57). In contrast, obese subjects showed a decreased risk of TB incidence: overweight (aHR 0.60, 95% CI 0.57–0.64), obese (aHR 0.45, 95% CI 0.43–0.48), and severely obese (aHR 0.33. 95% CI 0.28–0.39). The risk of TB increased with lower GFRs, with a GFR of 30–60 associated with an aHR of 1.09 (95% CI 1.02–1.16) and GFR ⩽ 30 associated with an aHR of 1.59 (95% CI 1.27–1.98). Having DM (aHR 1.24, 95% CI 1.18–1.32), a history of stroke (aHR 1.14, 95% CI 1.03–1.25) or pulmonary disease (aHR 1.62, 95% CI 1.55–1.70) were each associated with a greater incidence of TB. The results obtained when completing the analyses using a 1-year lag time were consistent with the main findings (Table 3).
Hazard ratios and 95% confidence intervals for the incidence of tuberculosis (the sensitivity analyses excluded subjects with the occurrence of end points within 1 year of follow-up).

Full model included sex, income level, smoking status, alcohol consumption, physical activity, body mass index, anemia, GFR, TUG test, diabetes mellitus, ischemic heart disease, stroke and pulmonary disease.
CI, confidence interval; GFR, glomerular filtration rate; HR, hazard ratio; PY, pack-years; ref., reference; TUG, timed up-and-go.
Discussion
In this study, we evaluated predictors for TB in the older population using a large nationwide longitudinal database. The results indicated that anemia, sarcopenia, and physical inactivity are predictors for TB in the older population. To the best of our knowledge, this is the first study indicating that anemia, slow TUG test (a surrogate for sarcopenia), and physical inactivity could stratify future TB risk in the older population. Further, we found that there are direct relationships between the risk of TB and the severity of anemia, the degree of physical impairment as assessed by the TUG test and of the level of physical inactivity as reported by the subjects.
Our results regarding predictors for TB in older people generally concur with those of previous studies performed in the general population. Previous studies have reported that men, lower BMI, low socioeconomic status, smoking, and alcohol consumption are significantly associated with a higher risk of TB. 19 Comorbidities such as DM, chronic kidney disease, asthma, and COPD are also important factors influencing TB occurrence. DM and chronic kidney disease can lead to impaired cell-mediated immunity21,22 and patients with asthma/COPD, especially those who use systemic or inhaled corticosteroids, can have suppressed defenses against TB in the airway, which increases the risk of TB development. 23 In addition, stroke was an independent risk TB predictor in the current study, which has not been reported in previous studies. It has been suggested that stroke induces an endogenous immunosuppression that might be an adaptive mechanism to protect against post-ischemic immune activation by brain antigens. 24
Although it is well known that many TB patients have anemia, especially anemia of chronic disease, 25 anemia has not previously been investigated as a possible risk factor for TB. A prospective cohort study evaluating human immunodeficiency virus (HIV)-infected patients who received antiretroviral therapy showed that the severity of anemia was strongly associated with TB incidence rates. 26 In HIV patients, dysregulation of the iron axis in HIV-related anemia could lead to a favorable intracellular macrophage environment for TB development.26,27 However, it is largely unknown whether anemia can predict future TB risk in the general population. To the best of our knowledge, this is the first study to report an increase in the incidence of TB according to anemia severity. In support of our findings, previous studies have reported that nutritional iron deficiency is associated with impaired phytohemagglutinin-induced lymphocyte proliferation and delayed-type hypersensitivity responses with relative preservation of humoral immunity. 28 Future studies are warranted to evaluate the exact mechanism by which anemia contributes to TB development in older adults.
Few previous studies have comprehensively evaluated whether sarcopenia is associated with TB risk. Patients who are at risk of TB have many clinical features of sarcopenia, such as low BMI, low socioeconomic status, DM, or chronic kidney disease. However, there have been no well-designed studies that evaluated the relationship between sarcopenia and TB risk. The TUG test is a simple test that consists of sit-to-stand, walking, turning, and stand-to-sit tasks, and has been widely used in older adults for geriatric assessment. As a reliable and valid functional mobility test, the TUG test is not only reflective of physiologic aging and general health status but can also effectively predict the risk of sarcopenia.10,11 Our study had the advantage of revealing novel findings that link decreased performance (slow TUG test), sarcopenia, and TB risk in the older population.
Another interesting finding in the present study was that low physical activity acted as a predictor of TB. Physical inactivity is a global public health problem that is considered a well-established preventable risk factor for non-communicable diseases such as DM and chronic heart disease. 29 Although the associations between physical activity and infectious diseases have not been well established, it is likely that physical activity can affect TB risk. A retrospective cohort study that evaluated TB risk factors in patients with DM showed that physical activity reduced the risk of TB in females with DM. 30 However, to date, no study has demonstrated that physical activity could reduce the risk of TB in the older population. From this perspective, our study provided informative data that low physical activity may be a predictor of TB in the older population. The exact mechanism by which regular physical activity confers the beneficial effect is not known. Regular physical activity may enhance the immune response against TB by improving the metabolic profile and enhancing immune function. 31
The present findings have both clinical and public health implications. Clinically, physicians should be aware of predictors for TB among the older population, and the intervention to avoid the predictors for TB might be helpful. For example, because anemia is a largely correctable disease, TB may be at least partially preventable through the treatment of anemia. It might be also important to emphasize physical activity for the prevention of sarcopenia. From a public health perspective, our study implies that reduction of anemia and sarcopenia through nutritional intervention and/or prevention of sarcopenia by encouraging physical activity would be helpful not only in enhancing general health but also by reducing TB incidence in the older population. Further research is warranted to examine whether intervening in those predictors reduces the risk of TB.
One major strength of our study was the reliability of the data obtained from the TB control system of Korea. In 2000, the Tuberculosis Notification Information System was established, and since 2001 all patients with TB have been required to register their cases electronically. 32 Other strengths included that the NHIS database includes data from the entire Korean population, which results in almost complete follow-up, and this study was conducted with a relatively large number of patients. There were also some limitations to our study. First, only 66-year-old adults were included, and we could not, therefore, identify whether TB risk is further increased in the very old age group. Second, the level of exposure might have changed over time. However, the study participants were not regularly examined during the follow-up period, and we were not able to measure the effect of a time-updated exposure. Third, as this study was performed in a country with an intermediate TB risk, the study results might not be applicable to the older population in other countries with different TB risks. Lastly, we did not formally calculate the sample size; however, this could be justifiable because all the participants who underwent NSPTA from 2009 to 2014 were retrospectively included.
Conclusion
This study showed that community-dwelling older adults who were physically inactive, had slow TUG test times, and anemia were at greater risk of developing TB. Considering the high prevalence of physical inactivity, sarcopenia, and anemia among older adults, strategies to reduce TB risk in the older population by addressing these new predictors are needed.
Footnotes
Acknowledgements
This study was performed using the National Health Insurance System database (NHIS-2020-1-054), and the results do not necessarily represent the opinion of the National Health Insurance Corporation. Restrictions apply to the availability of these data, which were used under license for this study.
Author contributions
JEY contributed to the study design and conception, interpreted of data, and drafted the work. DK and KH contributed to the data acquisition and statistical analysis. HC and YAK made substantial contributions to the interpretation of data and critically revised the work. HL and DWS contributed to the study design and conception, interpreted data, drafted the work, and were guarantors of the paper. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.