
Abstract
Aim:
The aim of this study was to establish whether non-vitamin K antagonist oral anticoagulants (NOACs) are superior to warfarin in preventing stroke recurrence for atrial fibrillation (AF) patients with an ischemic or hemorrhagic stroke at the baseline.
Methods:
From 1 January 2009 to 31 December 2017, stroke patients with AF treated with oral anticoagulants in the National Health Insurance Research Database in Taiwan were enrolled. The study was retrospective cohort design. Outcome measures were ischemic and hemorrhagic stroke recurrence. The Cox proportional hazard model was used to obtain the hazard ratio (HR).
Results:
In total, 39,840 stroke patients with AF treated with NOAC and 42,583 treated with warfarin were identified. NOACs were superior to warfarin in preventing all recurrent stroke [adjusted HR: 0.67, 95% confidence interval (CI), 0.63–0.71, p < 0.001]. Results for the ischemic stroke population were the same as that for all types for stroke (adjusted HR: 0.66, 95% CI, 0.62–0.70, p < 0.001). For the hemorrhagic stroke population, NOACs were equivalent to warfarin in preventing ischemic stroke (adjusted HR: 1.11, 95% CI, 0.86–0.43, p < 0.001), but NOACs were superior to warfarin in preventing hemorrhagic stroke (adjusted HR: 0.64, 95% CI, 0.55–0.74, p < 0.001).
Conclusions:
NOACs were generally superior to warfarin in terms of efficacy and safety in previous stroke patients. The robustness of our findings was verified and should add new information to current recommendations for Asian stroke patients in selecting NOACs.
Introduction
Stroke is the second leading cause of death and physical disability for adults globally.1,2 Atrial fibrillation (AF), the most common cardiac arrhythmia causing ischemic stroke,3–5 accounts for 12–20% of stroke cases.6,7 In Taiwan, stroke is also the third or fourth leading cause of death, 8 and AF was identified in 10.9% of ischemic stroke patients in a nationwide registry. 9 AF is also reported to increase the risk of ischemic stroke by 4–5-fold in Taiwan and globally. 4 Oral anticoagulants (OACs) are prescribed for patients with AF to prevent cardioembolic stroke. Warfarin used to be the most common OAC worldwide; however, warfarin exhibited a higher bleeding tendency in Asians. 10 Due to their non-inferior efficacy, better safety, and easier administration without the need for frequent blood tests, non-vitamin K antagonist OACs (NOACs) are currently considered first-line treatment for AF patients.11–14 Previous phase IV studies verified the efficacy and safety of four NOACs (rivaroxaban, dabigatran, apixaban, and edoxaban) for non-valvular AF Asian patients in Taiwan.15–18 Nevertheless, studies on NOAC treatment for patients with stroke at the baseline, especially hemorrhagic stroke, are scant. A recent study using a Danish nationwide database indicated no significant difference between NOACs and warfarin in preventing the ischemic and recurrent hemorrhage stroke incidence after 1 year in previous hemorrhagic stroke patients who had sustained AF. 19 The aim of this study was to offer the latest evidence for establishing the efficacy and safety of NOAC treatment for Asian patients who developed stroke and had sustained AF.
Methods
Design of the study
The study had a retrospective cohort study design. The National Health Insurance (NHI) system in Taiwan is a compulsory health insurance program, which covers >99.9% of all residents, and is characterized for comprehensive coverage of all outpatient and inpatient medical costs. 20 The NHI Research Database (NHIRD) contains all registered medical information for 23 million enrollees in the NHI system in Taiwan. 21 This study was approved by the Joint Institutional Review Board of Taipei Medical University (reference number: N201803076). The need for informed consent was waived as original personal information is encrypted and de-identified in the NHIRD.
Study population
From 1 January 2009 to 31 December 2017, patients who were diagnosed with stroke and who took any OACs for AF were enrolled. Diagnoses of ischemic stroke and hemorrhagic stroke (Table I, Supplemental material) were defined by the International Classification of Disease 9th Revision, Clinical Modification (ICD-9-CM) from 1 January 2009 to 31 December 2015, and by the ICD-10-CM from 1 January 2016 to 31 December 2017. Outpatients with a diagnosis of stroke were included if they had two clinic visits within 180 days (the date of the first visit was used as the index date), while inpatients were included and for whom the admission date was used as the index date. Exclusion criteria were the following: (1) patients who were aged <20 years, and (2) no use of any of the NOACs of dabigatran, rivaroxaban, apixaban, and edoxaban. Comorbidities and the medication history were accessed before the index date of a diagnosis of stroke. Initially, 1,230,390 stroke patients were identified. To examine the recurrent stroke risk, the CHA2DS2-VASc scores 22 were assessed for all enrolled patients. Of them, 1,100,217 stroke patients were excluded because they did not use any OACs, and 17,347 patients were excluded because of no prescription of any OACs after the incidence of stroke. The remaining 112,826 stroke patients were enrolled to assess the efficacy and safety between NOACs and warfarin (Figure 1).

Flow diagram of the study.
Use of OACs
Exposure to NOACs and warfarin was referenced to medication records in the NHIRD system. In Taiwan, rivaroxaban was approved for clinical use on 1 January 2012, dabigatran on 1 June 2012, apixaban on 1 January 2014, and edoxaban on 1 July 2016. For the NOAC group, the date on first use of any one of dabigatran, rivaroxaban, apixaban, and edoxaban after stroke diagnosed was defined as the index date. For warfarin, the index date was set as its first use after 1 January 2012. The codes for NOACs and warfarin are listed in Table II (Supplemental material). Of 112,826 stroke patients, 56,379 patients were identified to have used NOACs and 56,087 to have used warfarin. Among NOAC users, 14,426 patients were excluded for taking ⩾2 NOACs, and 2473 were excluded for taking both NOACs and warfarin. Among warfarin users, 13,504 were excluded for no prescription after 1 January 2012.
Outcome measurements
The primary outcome was a measure of all types of stroke recurrence, and secondary outcomes were measures of recurrent ischemic and hemorrhagic stroke, respectively. A new event of stroke recurrence was defined as fulfilling the criteria: (1) a previous stroke patient presenting to the emergency department (ED) with a diagnosis of stroke, and (2) subsequent admission for in-hospital management of stroke within 3 days of the date of the ED visit. The endpoints in this study were (1) a new event of stroke recurrence, (2) death, or (3) end of the study (31 December 2017). The sample size was estimated according to two previous studies. For the hemorrhagic stroke population, a study analyzing Danish nationwide data 19 showed that 55.9% of patients were treated with NOACs, and a sample size of 74–8316 was needed for a hazard ratio (HR) of 0.52–0.94, with α = 0.05, and 1−β (power) = 0.8. For the ischemic stroke population, a previous study 23 showed that 50.0% of patients were treated with NOACs, and a sample size of 15–565 was needed for an HR of 0.23–0.70, with α = 0.05, and 1−β = 0.8.
Subgroup analyses
Three types of subgroup analyses were conducted in this study. First, we conducted the subgroup analysis for different types of recurrent hemorrhagic stroke outcomes, including intracranial hemorrhage (ICH), subdural hemorrhage (SDH), subarachnoid hemorrhage (SAH). Second, we performed the subgroup analysis for four NOACs, and assessed their risk of recurrent stroke between different doses, respectively. Third, we investigated the outcomes of recurrent stroke for obesity population. The ICD-9-CM of 278 and ICD-10-CM of I66 were respectively employed to define the patients with obesity.
Statistical analyses
Continuous and discrete variables were respectively tested by Student’s t-test and Pearson’s Chi-squared test (or Fisher’s exact test). The inverse probability of treatment weighting (IPTW) by the propensity score was used to control for an imbalance of covariates between the NOAC and warfarin groups. 24 Characteristics of age, sex, baseline stroke diagnosis (ischemic or hemorrhagic stroke), comorbidities of AF, including peripheral artery occlusive disease, coronary artery disease (CAD), chronic heart failure, diabetes mellitus, hyperlipidemia, chronic kidney disease, and chronic liver disease (codes in Table III, Supplemental material), and medical history of warfarin and antiplatelet use (see codes in Table IV, Supplemental material) were included in the IPTW adjustment. The standardized mean difference (SMD) was computed to examine whether characteristics between NOAC and warfarin groups were balanced. An absolute difference of the SMD of <0.1 was considered a balanced baseline status between the NOAC and warfarin groups. The survival curves were plotted by Kaplan–Meier method. The Cox proportional hazard model was employed to assess the HR between the NOAC and warfarin groups. Outcomes of measures were analyzed for three categories of previous strokes at the baseline: (1) all types of stroke, (2) the ischemic stroke population, (3) and the hemorrhagic stroke population. Subgroup analyses of the four kinds of NOACs were conducted. All statistical analyses were performed with SAS 9.4 software (Cary, NC, USA) and Stata 15 (TX, USA). A two-sided p-value of <0.05 was defined as statistically significant.
Sensitivity analyses
We conducted six sensitivity analyses to assess the robustness of our findings. First, patients in the NOAC and warfarin groups were examined for days of medication use of 1–30, 31–90, 91–180, 181–360, and >360 days. Second, low-dose and standard-dose NOACs were compared. Standard and low doses for each NOAC were 15–20 and <15 mg for the rivaroxaban subgroup, 300 and <300 mg for dabigatran, 10 and <10 mg for apixaban, and 60 and <60 mg for edoxaban, respectively. Third, analysis with different lengths of prescription days after the index date (>1, >30, >90, >180, and >360 days) was performed. Fourth, a model of a competing risk of death was conducted. Lastly, patients who were enrolled before 1 January 2012 were excluded from analysis of all new stroke incidences after 1 January 2012.
Results
Baseline characteristics of all types of stroke populations
A flow diagram for identifying stroke patients taking NOACs and warfarin is shown in Figure 1. In this study, 39,840 stroke patients were identified as NOAC users and 42,583 as warfarin users. Of NOACs users, 20,687, 12,090, 5122, and 1941 patients were respectively treated with rivaroxaban, dabigatran, apixaban, and edoxaban. Baseline characteristics of stroke patients taking OACs are shown in Table 1. Before adjustment with the IPTW, patients treated with NOACs were older than those treated with warfarin (74.83 ± 9.63 versus 69.75 ± 12.83 years, SMD = 0.448), and the two groups showed differences in comorbidities of AF (70.90% versus 35.70%, SMD = –0.755), CAD (55.97% versus 50.81%, SMD = –0.104), hypertension (90.63% versus 85.75%, SMD = 0.152), and hyperlipidemia (60.25% versus 52.56%, SMD = –0.156), of warfarin use before the stroke (37.40% versus 66.53%, SMD = 0.610), and of antiplatelet use before the stroke (91.24% versus 87.12%, SMD = –0.133). Characteristics of gender, baseline stroke types, and other comorbidities were generally similar. The average times to the event between the NOAC and warfarin groups were 622.5 ± 503.8 and 987.4 ± 727.7 days, respectively. After IPTW adjustment, all characteristics showed SMDs of <0.1, and all variables between the NOAC and warfarin groups were in a balanced status. A graph on the distribution before and after IPTW adjustment is shown in Figure 2(A).
Baseline characteristics of stroke patients taking oral anticoagulants under Inverse Probability of Treatment Weighting (IPTW).
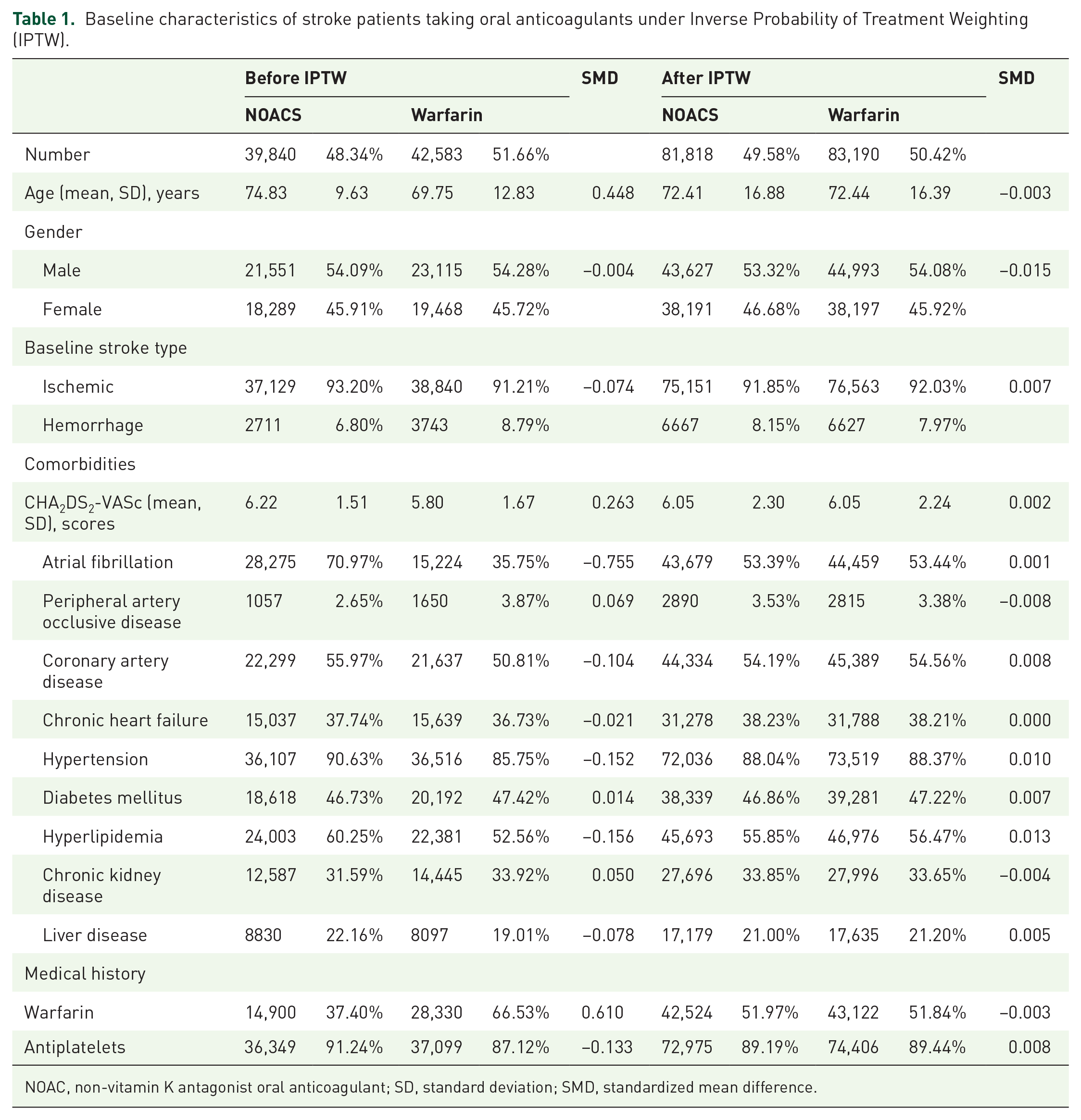
NOAC, non-vitamin K antagonist oral anticoagulant; SD, standard deviation; SMD, standardized mean difference.
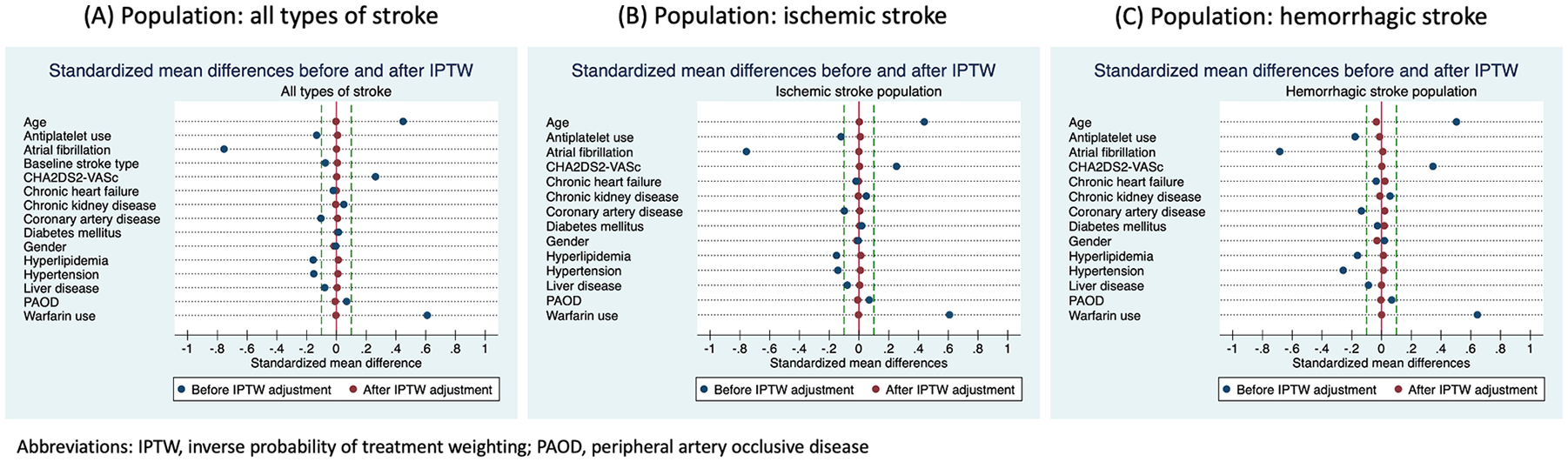
Data distribution before and after the inverse probability of treatment weighting (IPTW) adjustment for population of (A) all types of stroke at baseline; (B) ischemic stroke at baseline; and (C) hemorrhagic stroke at baseline.
Outcomes of measures for all types of stroke populations at the baseline
The survival curves for all types of stroke population are plotted in Figure 3. Incidence rates of recurrent stroke among the NOAC and warfarin groups with ischemic stroke are shown in Table 2. Both the NOAC and warfarin groups were followed up for more than 1 year, but the warfarin group was followed up longer (2.70 years) than the NOAC group (1.70 years). Patients treated with NOACs had lower recurrence rates of both types of stroke than those treated with warfarin (1.42 versus 1.77 per 100 person-years). The warfarin group had a higher proportion of recurrent hemorrhagic stroke than the NOAC group (24.32% versus 28.87%). Compared with the warfarin group, the NOAC group showed a significantly lower risk of all stroke recurrence (crude HR: 0.69, 95% confidence interval (CI), 0.64–0.74, p < 0.001; adjusted HR, 0.67, 95% CI, 0.61–0.73, p < 0.001; and adjusted HR under IPTW: 0.67, 95% CI, 0.63–0.71, p < 0.001). For recurrent ischemic stroke, the NOAC group showed a significantly lower risk than the warfarin group (crude HR: 0.73, 95% CI, 0.67–0.80, p < 0.001; adjusted HR, 0.71, 95% CI, 0.64–0.78, p < 0.001; and adjusted HR under IPTW: 0.70, 95% CI, 0.67–0.75, p < 0.001). For recurrent hemorrhagic stroke, the NOAC group also showed a significantly lower risk than the warfarin group (crude HR: 0.59, 95% CI, 0.50–0.68, p < 0.001; adjusted HR, 0.58, 95% CI, 0.49–0.69, p < 0.001; and adjusted HR under IPTW: 0.60, 95% CI, 0.54–0.66, p < 0.001).

The Kaplan–Meier curves for outcomes of recurrent stroke between (A) NOACs and warfarin; and (B) different NOACs and warfarin for population of all types of stroke.
Incidence rates of recurrent stroke for stroke patients taking NOACs or warfarin.

p < 0.001.
Adjusted for age, gender, baseline stroke type, atrial fibrillation, peripheral arterial occlusive disease, coronary heart disease, chronic heart failure, hypertension, diabetes mellitus, use of warfarin, and use of antiplatelets.
Incidence rate denotes events/total person-years (per 100 person-years).
HR, hazard ratio; n, number; NOAC, non-vitamin K antagonist oral anticoagulants; IPTW, inverse probability of treatment weighting.
Outcomes of measures for the ischemic stroke population at the baseline
The survival curves for ischemic stroke population were shown in Figure 4(A). Baseline characteristics for ischemic stroke patients before and after the IPTW adjustment are shown in Tables V and VI (Supplemental material). A graph on the distribution of the characteristics for ischemic stroke patients before and after IPTW adjustment is shown in Figure 2(B). In total, 75,969 patients with ischemic stroke at the baseline were identified. Of these, 37,129 and 38,540 ischemic stroke patients were categorized into the NOAC and warfarin groups, respectively (Table 3). Similar to the population with all types of stroke, the warfarin group had a longer follow-up time than the NOAC group (1.72 versus 2.73 years). The NOAC group had a significantly lower risk than the warfarin group of all types of stroke recurrence (crude HR: 0.68, 95% CI, 0.63–0.75, p < 0.001; adjusted HR, 0.65, 95% CI, 0.59–0.71, p < 0.001; and adjusted HR under IPTW: 0.66, 95% CI, 0.62–0.70, p < 0.001). As to secondary outcomes, the NOAC group had lower risks of recurrent ischemic stroke (crude HR: 0.70, 95% CI, 0.64–0.77, p < 0.001; adjusted HR, 0.68, 95% CI, 0.62–0.76, p < 0.001; and adjusted HR under IPTW: 0.68, 95% CI, 0.64–0.73, p < 0.001) and hemorrhagic stroke (crude HR: 0.61, 95% CI, 0.49–0.76, p < 0.001; adjusted HR, 0.49, 95% CI, 0.38–0.63, p < 0.001; and adjusted HR under IPTW: 0.55, 95% CI, 0.47–0.64, p < 0.001).

The Kaplan–Meier curves for outcomes of recurrent stroke between NOACs and warfarin for population of (A) ischemic stroke; and (B) hemorrhagic stroke.
Incidence rates of recurrent stroke among the ischemic stroke population taking NOACs or warfarin.

p < 0.001.
Adjusted for age, gender, baseline stroke type, atrial fibrillation, peripheral arterial occlusive disease, coronary heart disease, chronic heart failure, hypertension, diabetes mellitus, use of warfarin, and use of antiplatelets.
Incidence rate denotes events/total person-years (per 100 person-years).
HR, hazard ratio; IPTW, inverse probability of treatment weighting; NOAC, non-vitamin K antagonist oral anticoagulant.
Outcomes of measures for the hemorrhagic stroke population at the baseline
The survival curves for ischemic stroke population are shown in Figure 4(B). Baseline characteristics of hemorrhagic stroke patients before and after the IPTW adjustment are shown in Tables VII and VIII (Supplemental material). A graph on the distribution of the characteristics for hemorrhagic stroke patients before and after IPTW adjustment is shown in Figure 2(C). In total, 6454 patients with a hemorrhagic stroke at the baseline were identified. Of these, 2711 and 3743 patients were classified into the NOAC and warfarin groups, respectively (Table 4). Different from the ischemic stroke population at the baseline, no significant difference between the NOAC and warfarin groups was found in preventing a recurrent ischemic stroke (crude HR: 1.30, 95% CI, 0.91–1.86, p < 0.001; adjusted HR, 1.21, 95% CI, 0.81–1.81, p < 0.001; and adjusted HR under IPTW: 1.11, 95% CI, 0.86–1.43, p < 0.001). On the other hand, the NOAC group showed a lower risk of developing a hemorrhagic stroke than the warfarin group (crude HR: 0.72, 95% CI, 0.58–0.90, p < 0.001; adjusted HR, 0.67, 95% CI, 0.52–0.85, p < 0.001; and adjusted HR under IPTW: 0.64, 95% CI, 0.55~0.74, p < 0.001).
Incidence rates of recurrent stroke among the hemorrhagic stroke population taking NOACs or warfarin.

p < 0.05, **p < 0.01, ***p < 0.001.
Adjusted for age, gender, baseline stroke type, atrial fibrillation, peripheral arterial occlusive disease, coronary heart disease, chronic heart failure, hypertension, diabetes mellitus, use of warfarin, and use of antiplatelets.
Incidence rate denotes events/total person-years (per 100 person-years).
HR, hazard ratio; IPTW, inverse probability of treatment weighting; NOAC, non-vitamin K antagonist oral anticoagulant.
Subgroup analysis I: subtypes of hemorrhagic stroke outcomes
The outcomes for subtypes of hemorrhagic stroke are shown (Table IX, X, XI, Supplemental material). For all types of stroke populations at the baseline, the NOAC group showed significantly lower risk than the warfarin group for ICH (crude HR: 0.58, 95% CI, 0.49–0.69, p < 0.001; adjusted HR, 0.56, 95% CI, 0.46–0.68, p < 0.001; and adjusted HR under IPTW: 0.59, 95% CI, 0.52–0.66, p < 0.001), and SDH (crude HR: 0.50, 95% CI, 0.33–0.74, p < 0.001; adjusted HR, 0.56, 95% CI, 0.34–0.81, p < 0.001; and adjusted HR under IPTW: 0.49, 95% CI, 0.38–0.65, p < 0.001), respectively. Alike all types of stroke at baseline, both the population of ischemic stroke and hemorrhagic stroke at baseline showed the NOAC group with lower risk for ICH and SDH in comparison to warfarin. For SAH outcomes, no significant difference was observed for NOAC and warfarin groups for population of all types of stroke, ischemic stroke, and hemorrhagic stroke at baseline.
Subgroup analysis II: four NOACs subgroups
The efficacy and safety of each NOAC of rivaroxaban, dabigatran, apixaban, and edoxaban were respectively compared with warfarin in the subgroup analyses (Table 5). Outcome measures of the rivaroxaban subgroup showed a decreased risk of recurrent stroke of all types, of ischemic stroke, and of hemorrhagic stroke for the all-stroke population and ischemic stroke population at the baseline. In addition, the rivaroxaban subgroup showed no significant difference in outcomes of recurrent ischemic stroke compared with warfarin. The outcome pattern of the rivaroxaban subgroup was consistent with the entire NOAC group. For the dabigatran subgroup, the overall pattern was similar to the entire NOAC group except for the outcome of recurrent ischemic stroke (adjusted HR under IPTW: 1.67, 95% CI, 1.26–2.20, p < 0.001) in the baseline hemorrhagic stroke group. For the apixaban subgroup, outcomes for stroke of all types and ischemic stroke were similar to the entire NOAC group except for the hemorrhagic stroke population. The apixaban subgroup revealed no significant difference in outcomes of any type of stroke recurrence compared to warfarin. Lastly, the edoxaban subgroup showed consistently decreased risks for any type of recurrent stroke for all types of stroke, ischemic stroke, and hemorrhagic stroke at the baseline. The comparison between the four NOACs and warfarin were summarized in Figure 5 (5A and B). A further analysis for different dosing of four NOACs of rivaroxaban, dabigatran, apixaban, and edoxaban versus warfarin was conducted (Table XII, Supplemental material). Both the standard and low dosing of these four NOACs consistently showed lower risk for recurrent stroke development when compared with warfarin. Besides, low-dose edoxaban was shown to be more effective to prevent recurrent stroke when compared with the standard dose (Figure 5C).
Recurrent stroke among stroke patients using various NOACs [Adjusted † and Weighted Hazard Ratios (HRs)].

p < 0.05, ***p < 0.001.
Adjusted for age, gender, baseline stroke type, atrial fibrillation, peripheral arterial occlusion disease, coronary heart disease, chronic heart failure, hypertension, diabetes mellitus, use of warfarin, and use of antiplatelets.
NOAC, non-vitamin K antagonist oral anticoagulant.

Subgroup analyses for four NOACs. (A) Risk of recurrent stroke for comparing four NOACs with warfarin; (B) Comparison for the risk for recurrent stroke for NOACs with warfarin; and (C) Comparison for the risk for recurrent stroke between different doses and warfarin.
Subgroup analysis III: population of obesity
A total of 451 and 504 patients treated with warfarin and NOACs were identified in the population of obesity. The subgroup analysis for obese population showed no significant difference of recurrent stroke prevention between NOACs and warfarin (Table XIII, Supplemental material). Of subgroups of each NOAC, no significant difference for preventing recurrent stroke was observed as well. The HR for subgroup between edoxaban and warfarin was unavailable, as only one was patients treated with edoxaban was identified.
Sensitivity analyses
First, the days of medication use were analyzed (Table 6). For 1–30 days of prescription, no significant difference was found between NOACs and warfarin in preventing recurrent stroke (adjusted HR under IPTW: 0.98, 95% CI, 0.85–1.13, p < 0.01). For 31–90 days, the NOAC group showed a decreased risk for recurrent stroke (adjusted HR under IPTW: 0.77, 95% CI, 0.66–0.90, p < 0.001). For 91–180, 181–360, and >360 days of prescription, the NOAC group also showed consistently decreased risks for recurrent stroke in the crude and adjusted analyses (see Table XV in the Supplemental material for the number of stroke patients treated with NOACs and warfarin by days of prescription). Second, patients taking NOACs were divided into low-dose and standard-dose groups (see Table XIV in the Supplemental material for the number of patients). Compared with the warfarin group, both the low-dose and standard-dose groups consistently showed decreased risks for recurrent stoke. Third, for all various induction periods from 1 to 360 days, the NOAC group showed a uniformly decreased risk for recurrent stroke compared with the warfarin group in the crude and adjusted analyses. Fourth, with death as a competing risk, NOACs still showed a lower risk of recurrent stroke than the warfarin group (adjusted HR under IPTW: 0.74, 95% CI, 0.70–0.80, p < 0.001). Lastly, excluding patients enrolled before 1 January 2012, the results were consistent with the original model (adjusted HR under IPTW: 0.69, 95% CI, 0.64–0.75, p < 0.001).
Sensitivity analyses for Hazard Ratios (HRs) of recurrent stroke in stroke patients using NOACs versus warfarin.

**p < 0.01, ***p < 0.001.
Adjusted for age, gender, baseline stroke type, atrial fibrillation, peripheral arterial occlusion disease, coronary heart disease, chronic heart failure, hypertension, diabetes mellitus, use of warfarin, and use of antiplatelets.
IPTW, inverse probability of treatment weighting; NOAC, non-vitamin K antagonist oral anticoagulant.
Discussion
This study investigated previous stroke patients at the baseline who received medical treatment of either NOACs or warfarin to prevent recurrent stroke. Regardless of whether or not IPTW adjustment was performed, our results suggested that NOACs were superior to warfarin in preventing all types of recurrent stroke. For the ischemic stroke population, the results were the same as for all types of stroke. For the hemorrhagic stroke population, NOACs were shown to be equivalent to warfarin for preventing recurrent ischemic stroke, but NOACs were superior to warfarin in preventing hemorrhagic stroke.
Our study had a distinctive feature in analyzing stroke by employing previous stroke patients at the baseline. NOACs were found to be equivalent to warfarin in preventing ischemic stroke in the hemorrhagic stroke population at the baseline. In fact, a recent study analyzing a Danish nationwide cohort indicated that NOACs had a non-significantly lower risk of preventing ischemic and recurrent hemorrhagic stroke in previous hemorrhagic stroke patients. 19 However, our hemorrhagic stroke patients showed that NOACs were associated lower rates of recurrent hemorrhage stroke. We deduced that this was associated with the higher risk of bleeding with warfarin in Asians. On the other hand, for the ischemic stroke population, another recent study enrolling both previous transient ischemic attack and ischemic stroke patients found that NOACs of dabigatran and apixaban were not associated with better efficacy in preventing recurrent ischemic stroke except the rivaroxaban subgroup. 23 A major difference between our study and that previous study was that patients with a transient ischemic attack were excluded in our analyses. For our ischemic stroke population, all four NOACs were associated with a lower risk of recurrent ischemic stroke.
A recent network meta-analysis comparing three NOACs (rivaroxaban, dabigatran, and apixaban) and warfarin suggested different efficacy for secondary stroke prevention. 25 In the analysis, the priority rank for preventing ischemic stroke was listed as apixaban > rivaroxaban > warfarin > dabigatran, and the priority rank for hemorrhagic stroke was as dabigatran > apixaban > rivaroxaban > warfarin. 25 On considering the benefit and risk, this network meta-analysis 25 suggested apixaban was the first rank of choice for prevention of stroke. In our analyses, the newest NOAC edoxaban had the lowest risk for recurrent ischemic and hemorrhagic stroke when compared with warfarin. On excluding edoxaban, our analyses were similar to the network meta-analysis: apixaban had the lowest risk for preventing recurrent ischemic stroke and dabigatran had the lowest risk for hemorrhagic stroke when compared to warfarin (Figure 5A and B). However, we should not conclude edoxaban with the highest evidence for stroke prevention due to the short observation time (Table XVI, Supplemental material).
When compared with warfarin, both the standard and low dosing of four NOACs showed higher efficacy in prevent recurrent stroke. Besides, low-dose edoxaban was more effective in preventing recurrent stroke in comparison to its standard dose. However, this result should be cautiously interpreted, as our edoxaban subgroup had smaller sample size and shorter follow-up time. An earlier randomized clinical trial (RCT) comparing edoxaban and warfarin showed an unfavorable trend for low-dose edoxaban to prevent systemic embolism and stroke. 14 However, a recent published RCT for elderly Asian patients with AF favored low-dose edoxaban to prevent systemic embolism and stroke. 26 The optimal dose for Asian patients using edoxaban needs to be determined by further studies.
For the obese population, no significant difference for preventing stroke recurrence was observed between NOACs and warfarin in our enrolled patients. Previously, the “obese paradox” was described for AF patients of higher body weight or body mass index (BMI) treated with NOACs showed lower risks of systemic embolism and stroke when compared with those of normal weight. 27 The recent meta-analysis studies on analyzing the obese patients treated with NOACs showed two patterns: (1) the higher BMI subgroup was associated with lower thromboembolism risk in comparison to normal weight, and (2) no significant difference for stroke prevention was found between NOACs and warfarin in patients with extremely high BMI > 30 kg/m2.28–30 A major limitation for our analysis for the obese population was deficiency of exact body weight or BMI information in our database and limited sample size. To our mind, our analyses were still consistent with these meta-analysis studies. As our enrollment for patients with obesity was according to the disease codes of ICD-9-CM and ICD-10-CM, these patients were of morbid obesity (BMI > 35 kg/m2) in fact.
We performed several sensitivity analyses to verify the robustness for our findings. A distinguishing feature of the national cohort in Taiwan is that most stroke patients were treated with low-dose regimens of NOACs (Table X, Supplemental material). Physicians usually consider the body habitus of Asians patients to be relatively small, and are inclined to prescribe low doses of drugs. 31 Previous studies analyzing the NHIRD also found that >60% of AF patients were prescribed low doses of NOACS. 16 Both our study with stroke populations and other studies with AF populations consistently showed that NOACs were generally associated with lower risks of stroke recurrence. In addition, we noted a disparity in the number of stroke patients coded with AF between the NOAC and warfarin groups before IPTW adjustment.
Our study had strengths of a comprehensive investigation of outcomes of recurrent stroke in various model settings. An interesting finding was the days of prescription. For 1–30 days of prescription, no significant difference between the NOAC and warfarin groups was found in preventing recurrent stroke. We considered that this should not be attributed to decreased numbers of cases between the two groups (Table XI, Supplemental material). In fact, 7072 NOAC users and 8431 warfarin users were identified with 1–30 prescription days, which accounted for 20% of the total population and attained the needed sample size. These results suggested that NOACs were superior to warfarin in preventing stroke at least after 1 month of prescription. We also conducted another sensitivity analysis by prescription days after the index date. This analysis further confirmed the superiority of NOACs. In fact, most NOACs attain a biological therapeutic range within 4 h. For subgroup analyses, the four NOACs showed different outcomes. Although edoxaban seemed to be superior to warfarin for all kinds of outcomes of stroke recurrence in different stroke population sets, the number of cases was the smallest (n = 1941). As edoxaban was the last NOAC approved in Taiwan, this limited the number of available patients for outcome measures. This finding should be interpreted with caution.
This study has some limitations. The NHIRD contains no personal lifestyle information, and the risk factors of smoking, alcohol, and stroke severity were not adjusted for in this study. Most enrolled patients in the NHIRD are Asians. The study had an observational design. Some unmeasured residual confounders may have remained. In this study, the outcome of stroke recurrence was set with a strict definition. Patients with mild symptoms of stroke recurrence and treated in the outpatient department were not counted as an event in this study. For external generalizability, this study may extend the current recognition in selecting NOACs to prevent the recurrence of moderate to higher severity strokes.
Conclusion
In conclusion, NOACs were generally superior to warfarin in efficacy and safety in previous stroke patients. The sensitivity analyses verified the robustness of these findings. We also found that most stroke patients treated with NOACs were prescribed low-dose regimens. In fact, no significant difference was found between low-dose and standard-dose regimens in preventing stroke recurrence. Our results should add new information to current recommendations for Asian stroke patients in selecting NOACs for preventing stroke recurrence.
Supplemental Material
sj-pdf-1-taj-10.1177_2040622320974853 – Supplemental material for Risk of recurrent stroke for Asian stroke patients treated with non-vitamin K antagonist oral anticoagulant and warfarin
Supplemental material, sj-pdf-1-taj-10.1177_2040622320974853 for Risk of recurrent stroke for Asian stroke patients treated with non-vitamin K antagonist oral anticoagulant and warfarin by Sheng-Feng Lin, Yi-Hsuan Lu and Chyi-Huey Bai in Therapeutic Advances in Chronic Disease
Footnotes
Acknowledgements
Each author contributed to the conception and design of the study, acquisition, analysis, and interpretation of data. SF Lin wrote the first draft of the manuscript. The Ministry of Science and Technology (MOST) is s the governmental entity. The funder (MOST) had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ministry of Science and Technology (MOST) and the reference number was MOST 107-2314-B-038-072-MY3.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.