
Abstract
Background:
Posterior heel pain may occur after an Achilles insertional rupture reattachment procedure and could be attributed to an impingement between the calcaneal tuberosity and Achilles tendon, which could be observed using postoperative magnetic resonance imaging (MRI). Moreover, such impingement, which may be associated with postoperative pain symptoms, could be relieved by calcaneoplasty.
Methods:
Postoperative Visual Analog Pain Scale (VAS), American Orthopedic Foot and Ankle Society (AOFAS) score, Foot Function Index (FFI), Ankle Activity Score (AAS), and Tegner score were obtained and compared between 10 patients who underwent calcaneoplasty (calcaneoplasty group) and 11 patients who did not receive calcaneoplasty (non-calcaneoplasty group). Several signs of calcaneal tuberosity impingement identified in MRI were also compared between the two groups, which included retrocalcaneal bursitis, postoperative tendinopathy, tendon calcification, bone marrow edema, increased Achilles tendon diameter, and bony spurs.
Results:
The VAS score was 2.00 ± 1.41 and 2.18 ± 1.83 (p = 0.803), the AOFAS score was 90.60 ± 4.22 and 81.82 ± 7.77 (p = 0.005), the FFI was 5.00 ± 2.86 and 17.18 ± 15.92 (p = 0.028), the AAS was 5.50 ± 2.55 and 5.82 ± 2.04 (p = 0.750), and the Tegner score was 4.30 ± 1.49 and 4.45 ± 1.21 (p = 0.797) in the calcaneoplasty and non-calcaneoplasty groups, respectively. The AOFAS score and FFI were significantly different between the groups. MRI findings revealed that the non-calcaneoplasty group had significant signs of calcaneal impingement compared with the calcaneoplasty group.
Conclusions:
Secondary calcaneal impingement due to insertional tendon enlargement may occur, and prophylactic calcaneoplasty coupled with an insertional reattachment procedure could achieve promising postoperative outcomes for patients with insertional Achilles tendon rupture.
Keywords
Introduction
Insertional Achilles tendinopathy is a disorder with symptoms of pain and swelling in the Achilles tendon insertion. Its pathological characteristics include degeneration, disorganization of the tendon’s fibers, small hemorrhages, calcification, and the occurrence of a bony spur on the Achilles tendon insertion.1–3 For its etiology, overuse in sports activity and poor training habits could exert gradual repetitive traction forces that could result in microtrauma and a chronic inflammatory response on the Achilles tendon insertion. Moreover, the risk factors include corticosteroid use, diabetes, obesity, and old age. Enlarged calcaneal tuberosity, or Haglund’s deformity, is also associated with insertional Achilles tendinopathy.4,5
Haglund’s deformity is an abnormality of the posterosuperior calcaneal process in which a bony prominence is found at the attachment of the Achilles tendon.4,6 Evidence provided by Schepsis and Leach 6 revealed that this bony prominence causes impingement on the retrocalcaneal bursa and the insertion of the Achilles tendon, and induces inflammation, degeneration, and even partial or complete rupture of the Achilles tendon insertion. 7 Several radiological measurement methods were developed to describe the calcaneal prominence and its relationship to the Achilles tendon and bursae: Haglund’s deformity height and peak angle, Bohler’s angle, Fowler–Philip angle, and parallel pitch sign. 8 Other researchers presented reliable objective criteria for the diagnosis of Haglund’s deformity, including parallel pitch lines, Chauveaux–Liet angle, ill-defined retrocalcaneal recess, superficial tendo-Achilles bursa, and anteroposterior Achilles tendon diameter of >9 mm (approximately 2 cm above the insertion). 9 However, the morphological measurements of the calcaneal tuberosity in insertional Achilles tendinopathy remain controversial. Bulstra et al. 10 found that the radiographic characteristics of the superior–posterior calcaneal tuberosity are not associated with any clinically relevant symptoms; moreover, no significant differences in the radiographic measurements were noted between the symptomatic Haglund’s deformity group and the control group.
A recent literature also questioned the utility of calcaneal tuberosity measurements and suggested that Haglund’s deformity is not associated with insertional Achilles tendinopathy. 11 Those studies have found no differences in the Fowler–Phillip angle or the Bohler’s angle between persons with, and those without, insertional Achilles tendinopathy. Although statistically the Chauveaux–Liet angle differed between persons with insertional Achilles tendinopathy and those without heel pain in one case-control study, the clinical relevance of the difference was unclear because of the high variability in the measurement.8,11,12 Kang et al. 8 suggested that Haglund’s deformity is not indicative of insertional Achilles tendinopathy, because it could also be found in asymptomatic patients. Moreover, difference in radiological measurements of Haglund’s deformities between patients with, and those without, insertional tendinopathy showed little significance; thus, they suggested that excision of Haglund’s deformity may not be necessary in the operative treatment of insertional Achilles tendinopathy. However, relying solely on the radiographic evaluations of the lateral ankle joint may not be recommended because of inconsistent findings and thus data may be insufficient for the decision to perform calcaneoplasty for insertional Achilles tendinopathy.8,11,12
Resection of the superior–posterior prominence of the calcaneal tuberosity using open or mini-invasive procedures has been a routine practice for insertional Achilles tendinopathy, which is always combined with debridement of the Achilles insertion, excision of calcified tissue, and reattachment procedures, depending on the severity of the disorder.3,12–14 In a previous study, 16 of 21 patients were found to have excellent or good outcomes after tendon debridement without excision of Haglund’s deformity.15,16
We therefore ask the following questions: is it necessary to measure Haglund’s deformity before an insertional tendinopathy operation, and is it valuable to perform calcaneoplasty during insertional Achilles tendon reattachment procedure? We hypothesized that a pre-existing calcaneal tuberosity prominence and an enlarged Achilles tendon diameter postoperatively may play an important role in the development of a secondary impingement of the posterosuperior calcaneal tuberosity and may contribute to postoperative pain symptoms. 17 Thus, in this study, we aimed to compare the postoperative clinical outcomes and retrocalcaneal impingement signs based on magnetic resonance imaging (MRI) between patients with insertional Achilles tendon ruptures who underwent reattachment procedures with calcaneoplasty and those without calcaneoplasty.
Methods
We retrospectively reviewed 21 acute insertional Achilles tendon ruptures (19 males, two females) between January 2015 and April 2018, with a follow up of a minimum of 20 months. Several subjective outcome scales were documented, and MRI scans were performed in all patients in the outpatient department. All patients had no previous history of fracture, infection, surgery, or congenital ankle deformity. The diagnosis of insertional Achilles tendon rupture was confirmed radiologically and with MRI. 18 The diagnosis was further confirmed by intraoperative findings. Standard lateral radiographs of the ankle were obtained, which showed the fragment of the avulsed fracture and the bony spur on the insertion of the calcaneal tuberosity. Several radiological parameters that determine the features of Haglund’s deformity were also measured,8,13,19 including the pitch line, Haglund’s height, Chauveaux–Liet angle, and Fowler–Philip angle. A total of 11 patients with insertional Achilles tendon rupture underwent reattachment procedures without calcaneoplasty (non-calcaneoplasty group) and were followed up from 2015 to 2017, while 10 patients had reattachment procedures with calcaneoplasty (calcaneoplasty group) and were followed up from 2017 to 2018 (Figure 1). All study protocols were approved by the local ethics committee (Peking University Third Hospital Medical Science Research Ethics Committee, M2018040).

Reattachment procedures for insertional Achilles tendon ruptures, without and with calcaneoplasty.
Surgical technique and postoperative rehabilitation
The surgical procedure was performed as described previously. 18 A longitudinal lazy-L incision was made in the medial border of the Achilles tendon. The stump of the Achilles tendon was fixed to the insertional site of the calcaneal tuberosity by suture anchors or the bone tunnel technique. In the calcaneoplasty group, the bony prominence at the posterosuperior aspect of the calcaneum was osteotomized prior to Achilles tendon reattachment. Postoperatively, the ankle was immobilized daily for 4 weeks by a short-leg cast at 10° plantarflexion, which was followed by removable ankle brace immobilization with passive range of motion from 20° plantarflexion to 0° dorsiflexion once a day. At 6 weeks after the operation, the patients gradually started weight bearing, which included walking in a walk boot with a heel lift for 4 weeks.
Patient demographics and outcome assessments
Several characteristics of the patients who were followed up, including age, sex, body mass index (BMI), follow-up time, and history of Achilles tendinopathy, were recorded.
Moreover, subjective outcome scores were recorded during follow up, including Visual Analog Pain Scale (VAS-pain), American Orthopedic Foot and Ankle Society (AOFAS) score, Foot Function Index (FFI), Tegner score, and Ankle Activity Score (AAS). All scores were compared between the calcaneoplasty and non-calcaneoplasty groups. All complications, including deep vein thrombosis, sural neuritis, superficial wound problems, re-rupture, foreign-body reaction to the suture anchor, requiring reoperation, and deep infection requiring reoperation, were documented.
MRI measurements for postoperative impingement of Achilles tendon insertion
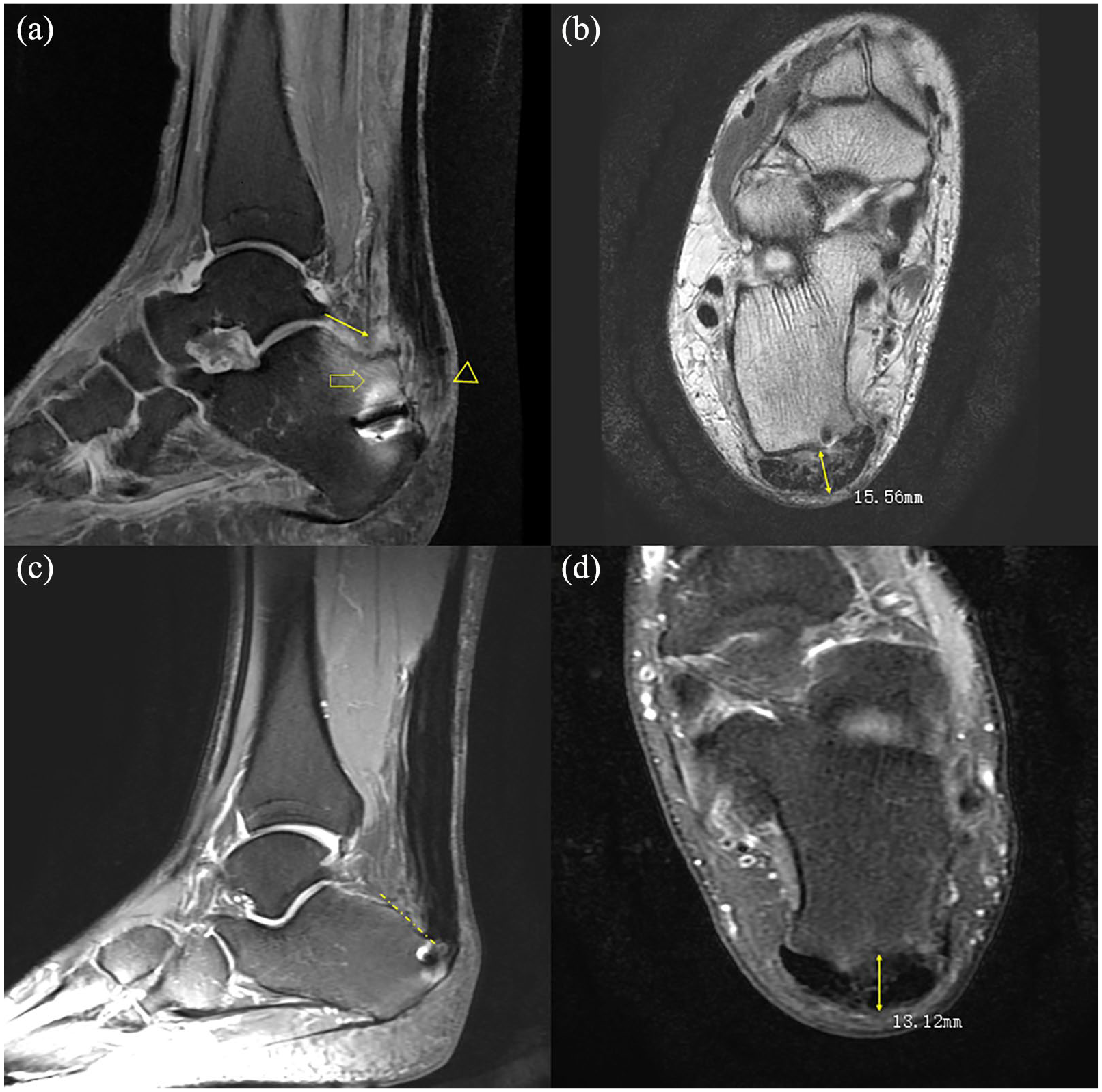
After the operation, MRI of the Achilles tendons was performed and the scans were analyzed by Centricity RIS-IC software (Centricity RIS-IC, Radiology Information Systems, GE Healthcare, Boston, USA). The following signs of impingement between the calcaneal tuberosity and Achilles tendon were identified in the axial and sagittal views of the T2-weighted images (Figure 2):11,20,21 (a) retrocalcaneal exudation or bursitis; (b) degeneration or inflammation of the Achilles tendon opposite to the posterosuperior calcaneal tuberosity; 22 heterogeneous intratendinous hyperintensity of tendons was assessed using MRI and classified into five categories according to the Pomranz system 23 [i.e. grade 0, homogeneous hypointensity (normal) ± peritendinous fluid; grade IA, hypointense signal on T1 that disappears on T2; grade IB, intratendinous isointensity on T1 (<50% tendon) and intratendinous iso- or hyperintensity on T2; grade II, intratendinous isointensity on T1 (>50% tendon), intratendinous hyperintensity on T2, attenuated size; grade III, tendon transection with retraction and peritendinous, hypointensity on T1, and hyperintensity on T2]; (c) bone-marrow edema, osteophytosis, or erosion of the posterosuperior calcaneal tuberosity; (d) enlarged anterior–posterior diameter of the Achilles tendon 2 cm above the insertion, which was measured in the horizontal view (Figure 3);15,21 and (e) bony spur on the calcaneus insertion. 1
Reattachment procedures for insertional Achilles tendon ruptures, without calcaneoplasty and with calcaneoplasty.

Achilles tendon diameters after the non-insertion rupture operation and insertional rupture operation.
Statistical analysis
SPSS 19 software (IBM, New York, USA) was used for statistical analysis. Continuous variables were compared and analyzed using Wilcoxon rank-sum test. Fisher’s exact chi-square test analysis was used for the comparison of categorical variables. A significant difference was defined as p < 0.05.
Results
Demographic characteristics of patients with insertional Achilles tendon rupture
Baseline characteristics, including age, BMI, local corticosteroid administration, history of tendinopathy, and follow-up time, were compared between the calcaneoplasty and non-calcaneoplasty groups (Table 1), and no significant differences were noted between the groups.
Baseline characteristics of the calcaneoplasty and non-calcaneoplasty groups.

p < 0.05 indicates a significant difference.
BMI, body mass index.
Comparison of Haglund’s deformity between patients with and those without calcaneoplasty
Haglund’s deformity in the calcaneoplasty and non-calcaneoplasty groups was analyzed. The degree of Haglund’s deformity was compared between the groups. Haglund’s deformity height was significantly different between the groups (Table 2).
Haglund’s deformity measurements between the calcaneoplasty and non-calcaneoplasty groups.

p < 0.05 indicates a significant difference.
Bold numerals, normal values.
Comparison of postoperative outcomes and MRI characteristics between patients with and those without calcaneoplasty
Postoperative outcomes were recorded and compared between the calcaneoplasty and non-calcaneoplasty groups. VAS score was 2.00 ± 1.41 and 2.18 ± 1.83 (p = 0.803); the AOFAS score was 90.60 ± 4.22 and 81.82 ± 7.77 (p = 0.0005); the FFI was 5.00 ± 2.86 and 17.18 ± 15.92 (p = 0.028); the AAS was 5.50 ± 2.55 and 5.82 ± 2.04 (p = 0.755); and the Tegner score was 4.30 ± 1.49 and 4.45 ± 1.21 (p = 0.797) in the calcaneoplasty and non-calcaneoplasty groups, respectively. The AOFAS score and FFI were significantly different between the groups (p < 0.05). No complications were reported in both groups.
Several signs indicating Haglund’s deformity were measured postoperatively. Most of the signs were more commonly observed in the non-calcaneoplasty group than in the calcaneoplasty group. Except for Achilles tendon calcification, which was not observed in both groups, significant differences in the signs indicating Haglund’s deformity on MRI were found between the non-calcaneoplasty and calcaneoplasty groups (Figures 4 and 5, Table 3).

Secondary impingement signs identified by MRI between the non-calcaneoplasty and calcaneoplasty groups.
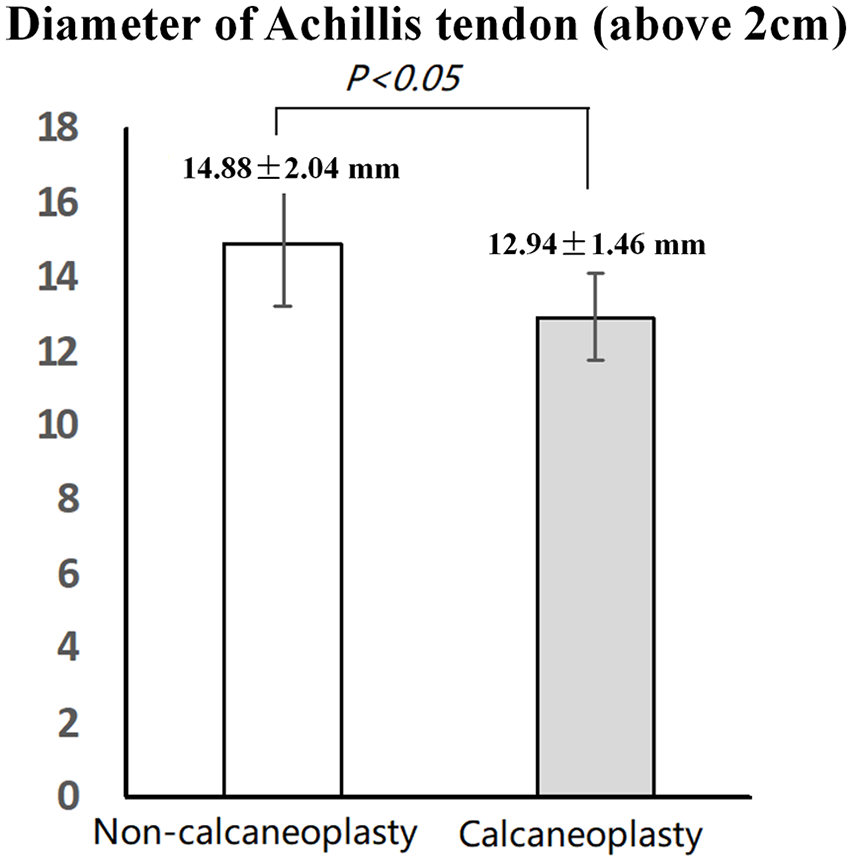
Achilles tendon diameter 2 cm above the insertion was compared between the non-calcaneoplasty and calcaneoplasty groups.
Comparison of MRI signs between the non-calcaneoplasty and calcaneoplasty groups.

p < 0.05 indicates a significant difference.
MRI, magnetic resonance imaging.
Discussion
In our study, acute insertional Achilles tendon ruptures were managed surgically by insertional reattachment procedure. In the follow up, regardless of preoperative history of insertional Achilles tendinopathy, some patients experienced postoperative retrocalcaneal pain and exhibited posterosuperior calcaneal tuberosity impingement on the Achilles tendon insertion on MRI. Although the value of Haglund’s deformities in these patients was much different compared to that in patients with acute non-insertional Achilles tendon rupture (Supplemental 1, Table 4), the former failed to meet the diagnostic criteria of Haglund’s deformities. Moreover, the diameters of the Achilles tendons in the patients with insertional Achilles tendon ruptures were found to be enlarged (Supplemental 1).
Haglund deformity measurements between insertional and non-insertional rupture of Achilles tendons.

p < 0.05 indicates a significant difference.
Bold nunerals, normal values.
To determine whether resecting the enlarged prominence of the calcaneal tuberosity for the insertional tendinopathy reattachment procedure is still necessary, we evaluated 21 patients who had a reattachment procedure for acute insertional Achilles tendon rupture, which was considered the end-stage of insertional tendinopathy. 18 We found that the pitch line, Haglund height, Chauveaux–Liet angle, and Fowler–Philip angle were significantly larger in acute insertional Achilles tendon rupture than in non-insertional Achilles tendon rupture. However, the abnormally enlarged calcaneal tuberosity in insertional Achilles rupture did not meet the diagnostic criteria for Haglund’s deformity and had not correlated with preoperative symptoms. Nonetheless, we suspect that such enlargement may potentially be associated with postoperative clinical outcomes.
To prove our hypothesis, patients with insertional rupture were divided into two groups: calcaneoplasty and non-calcaneoplasty groups. The groups had similar baseline characteristics. Postoperative outcomes were measured and compared, and we found that the AOFAS score and FFI were significantly different between the groups. The signs of retrocalcaneal impingement on MRI were also significantly different between the groups. Moreover, based on MRI, an increased Achilles tendon diameter may apply pressure against the pre-existing enlarged prominence of the calcaneal tuberosity. Thus, patients without calcaneoplasty may be diagnosed as having Achilles impingement tendinopathy, which in turn could result in postoperative pain.
Limitations
This study has some limitations, which include its retrospective study design, a small sample size and lack of sample size calculation, and a short follow-up time.
Conclusion
Therefore, regardless of the radiological findings of Haglund’s deformity, prophylactic calcaneoplasty coupled with an insertional reattachment procedure could achieve promising postoperative outcomes in patients with insertional Achilles tendinopathy.
Supplemental Material
supplement – Supplemental material for Calcaneoplasty coupled with an insertional Achilles tendon reattachment procedure for the prevention of secondary calcaneal impingement: a retrospective study
Supplemental material, supplement for Calcaneoplasty coupled with an insertional Achilles tendon reattachment procedure for the prevention of secondary calcaneal impingement: a retrospective study by Yanbin Pi, Yuelin Hu, Qinwei Guo, Dong Jiang, Xin Xie, Feng Zhao, Linxin Chen, Yingfang Ao and Chen Jiao in Therapeutic Advances in Chronic Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study is funded by Peking University Medicine Seed Fund for Interdisciplinary Research and the Fundamental Research Funds for the Central Universities No.BMU2020MX020; Key Clinical Projects of Peking University Third Hospital No. Y72484-02.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.