
Abstract
Background:
D-dimer has predictive value for mortality in some diseases. This study aimed to evaluate the correlation between D-dimer and mortality in patients undergoing percutaneous coronary intervention (PCI).
Methods:
We examined 10,724 consecutive patients who underwent PCI between January 2013 and December 2013. The primary endpoint was all-cause mortality, and the secondary endpoint was cardiac mortality. Patients were divided according to the median D-dimer level of 0.28 μg/ml. Multivariable model were including age, sex, and risk factors after stepwise selection.
Results:
After a 2-year follow up, 8565 patients with D-dimer data were analyzed. There were 116 (1.35%) all-cause deaths and 64 (0.75%) cardiac deaths. D-dimer levels were significantly higher in the all-cause mortality group [0.42 (0.29, 0.68) μg/ml] and cardiac mortality group [0.48 (0.30, 0.81) μg/ml] than in the survival group [0.28 (0.20, 0.41) μg/ml] (both p < 0.001). Multivariate-adjusted Cox hazard analysis showed that high D-dimer levels (⩾0.28 μg/ml) were significantly associated with all-cause mortality in the total population [hazard ratio (HR): 2.35, 95% confidence interval (CI): 1.44–3.84, p = 0.001], acute coronary syndrome (ACS) subgroup (HR: 1.91, 95% CI: 1.08–3.38, p = 0.027), and stable coronary artery disease (SCAD) subgroup (HR: 3.82, 95% CI: 1.45–10.10, p = 0.007). High D-dimer levels were significantly associated with cardiac mortality in the total population (HR: 3.44, 95% CI: 1.61–7.36, p = 0.001) and the ACS subgroup (HR: 3.33, 95% CI: 1.38–8.03, p = 0.007), but not in the SCAD subgroup (HR: 3.68, 95% CI: 0.80–16.91, p = 0.094).
Conclusions:
D-dimer levels are independently associated with 2-year all-cause mortality and cardiac mortality in patients undergoing PCI.
Introduction
Despite recent development of percutaneous coronary intervention (PCI) technology and standardized use of dual antiplatelet and statin drugs, some patients still experience cardiovascular events. Residual risk after PCI may be conferred by pathways not optimally controlled with antiplatelets and statins, including particles other than low-density lipoprotein [such as high-density lipoprotein (HDL), very low-density lipoprotein (VLDL), triglycerides] as well as mediators of inflammation and thrombosis. Lipoprotein is used as a lipid marker, while high-sensitivity C-reactive protein is used as an inflammatory marker, but there is a lack of markers for predicting the risk of thrombosis.
D-dimer is a cross-linked, fibrin-specific, degradation product. Elevation of D-dimer levels is a sensitive marker for thrombosis, 1 and D-dimer is one of the most commonly used coagulation marker in clinical practice. Increased D-dimer levels are independently associated with the adverse clinical outcomes, 2 such as pulmonary embolism, 3 venous thromboembolism, 4 tumors,5,6 stroke, 7 and aortic dissection. 8 Recent, relatively small sample size, studies have shown that D-dimer levels are independently associated with the risk of death in patients with acute coronary syndrome (ACS).9–11 In addition, Simes and colleagues showed that D-dimer was a significant long-term predictor of cardiovascular and cancer mortality in stable coronary artery disease (SCAD) patients. 12 The association of D-dimer and mortality after PCI needs to be documented.
Therefore, this study aimed to evaluate the association of D-dimer levels with mortality in a large sample of patients who had PCI, as well as in ACS and SCAD subgroups. We hypothesize that coagulation markers could help identify high-risk patients who undergo PCI, and provide more precise antithrombotic therapy to these patients.
Methods
Study design
We performed an observational, prospective, single-center study. A total of 10,724 consecutive patients who underwent PCI in Fuwai hospital (National Center for Cardiovascular Diseases, Beijing, China) were enrolled, and data were collected between January 2013 and December 2013. After excluding 2109 patients with missing D-dimer data and 50 patients lost to follow up, a total of 8565 patients were included in the final analysis (Figure 1). All patients underwent electrocardiogram (ECG), X-ray, echocardiography, and blood tests in the morning within 24 h of admission. Clinically relevant baseline data were collected in detail. This study was approved by the Fuwai hospital Ethics Committee (approval number 2013-449), and all patients provided written informed consent.

Patient Flowchart of patients enrolled for the study cohort.
The PCI strategy and stent type were left to the treating physician’s discretion. If patients with selective PCI were not taking long-term aspirin and P2Y12 inhibitors, they received 300 mg aspirin and clopidogrel orally (loading dose: 300 mg) or ticagrelor (loading dose: 180 mg) at least 24 h before the procedure. After PCI, patients were prescribed aspirin 100 mg once daily indefinitely, and either clopidogrel 75 mg once daily or ticagrelor 90 mg twice daily for at least 1 year.
D-dimer measurements
Blood samples were obtained after an overnight fast in the morning within 24 h of admission. Blood samples were drawn into tubes containing sodium citrate 3.2% and sent to the laboratory for D-dimer testing as soon as possible. We used the Stago-R Evolution (France) automatic coagulation analyzer for detecting plasma D-dimer levels. The normal range of D-dimer levels is <0.5 μg/ml. Patients were divided into the high D-dimer group (⩾0.28 μg/ml) and low D-dimer group (<0.28 μg/ml) according to the median D-dimer level of 0.28 μg/ml.
Endpoints and follow up
The primary endpoint was all-cause mortality, and the secondary endpoint was cardiac mortality. The ACS subgroup included acute myocardial infarction and unstable angina pectoris. Myocardial infarction was defined by the third universal definition of myocardial infarction. 13 The SCAD subgroup was defined as patients without ACS, and the indication for inclusion criteria and PCI was that patients with evidence of ischemia or fractional flow reserve ⩽0.8, and coronary angiography showed a lesion with a coronary stenosis greater than 70% (left main stem greater than 50%). All endpoints were adjudicated centrally by two independent cardiologists, and disagreement was resolved by consensus. All patients were evaluated at 1, 6, 12, and 24 months of follow up through clinical visits or by phone. Patients were advised to return for coronary angiography if clinically indicated by symptoms or documentation of myocardial ischemia. Patients who reported any ischemic or bleeding events were required to submit related source documents. All adverse events were thoroughly analyzed and adjudicated by two separate cardiologists, and disagreement was resolved by consensus.
Statistical analysis
Continuous variables with a normal distribution are expressed as mean ± standard deviation, and non-normally distributed continuous variables as median with quartiles. Continuous variables were compared by the Student’s t test. Categorical variables are expressed as number (%) and were compared using the Pearson chi-squared test or Fisher’s exact test. D-dimer levels were expressed as median (Q1, Q3), and compared by Wilcoxon methods in different groups. D-dimer levels were categorized into two groups by the median value. Survival curves were generated in each D-dimer group by the Kaplan–Meier method, and differences were compared with the log-rank test. To evaluate the effect of different levels of D-dimer on mortality, hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated from the Cox proportional hazards regression model. Model 1 was a univariate model of D-dimer. Model 2 was adjusted for age and sex. Model 3 was adjusted for age, sex, and other available risk factors that remained significant after stepwise regression (entry probability = 0.05 and deletion probability = 0.10), including body mass index, hypertension, diabetes, current smoking, previous myocardial infarction, previous PCI, previous coronary artery bypass grafting (CABG), previous stroke, peripheral vascular disease, anemia, creatinine clearance (CrCl) <60 ml/min, left ventricular ejection fraction (LVEF), and the baseline Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (SYNTAX) score. The value of risk prediction of D-dimer was evaluated using C-statistics, and we calculated the C-statistic from the area under the curve (AUC) by logistic model adjusted for variables in model 3. Two-sided p values of 0.05 were considered statistically significant. All statistical analyses were performed with SAS 9.2 software (SAS Institute, Cary, NC, USA).
Results
Patient characteristics
Of the 10,724 consecutive patients who underwent PCI, after excluding 2109 patients with missing D-dimer data and 50 patients lost to follow up, a total of 8565 patients were included in the final analysis (Figure 1). After a 2-year follow up, 116 all-cause deaths (1.35%) and 64 (0.75%) cardiac deaths occurred. The mean age of the patients was 58.48 ± 10.37 years and 23.48% were women. There were 5110 patients with ACS (including 3618 with unstable angina and 1492 with acute myocardial infarction) and 3455 with SCAD. Almost all of the patients received dual antiplatelet (8442, 98.56%) and statin (8227, 96.05%) therapy. Only 11 (0.13%) patients received oral anticoagulant. All of the patients underwent PCI therapy; among them, 8094 (94.50%) patients were successfully implanted with drug-eluting stents.
According to the median D-dimer level of 0.28 μg/ml, the patients were divided into high (⩾0.28 μg/ml) and low (<0.28 μg/ml) D-dimer groups. Table 1 shows that patients in the high D-dimer group were older, and there was a higher proportion of females, a lower body mass index, and lower current smoking rate compared with those in the low D-dimer group. Patients in the high D-dimer group had significantly higher rates of hypertension, previous myocardial infarction, previous CABG, stroke, previous peripheral vascular disease, anemia, CrCl <60 ml/min, a history of heart failure, and lower LVEF compared with those in the low D-dimer group. The high D-dimer group had a significantly higher rate of bridge vascular lesions, higher baseline SYNTAX scores, more patients required IABP, and more patients received femoral artery puncture compared with the low D-dimer group.
Baseline clinical characteristics in patients who underwent PCI with high and low D-dimer levels.

Values are mean ± SD or n (%).
BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CrCl, creatinine clearance; IABP, intra-aortic balloon pump; LM, left main; LVEF, left ventricular ejection fraction; MI, myocardial infarction; OAC, oral anticoagulation; PCI, percutaneous coronary intervention; SD, standard deviation.
D-dimer levels and clinical endpoints
For all-cause mortality, D-dimer levels were significantly higher in patients who died than in those who survived in the total population [0.42 (0.29, 0.68) μg/ml versus 0.28 (0.20, 0.41) μg/ml, p < 0.001], in the ACS subgroup [0.40 (0.28, 0.86) μg/ml versus 0.28 (0.20, 0.42) μg/ml, p < 0.001], and in the SCAD subgroup [0.47 (0.29, 0.66) μg/ml versus 0.28 (0.20, 0.39) μg/ml, p < 0.001].
For cardiac mortality, D-dimer levels were significantly higher in patients who died than in those who survived in the total population [0.48 (0.30, 0.81) μg/ml versus 0.28 (0.20, 0.41) μg/ml, p < 0.001], in the ACS subgroup [0.45 (0.29, 0.93) μg/ml versus 0.28 (0.20, 0.42) μg/ml, p < 0.001], and in the SCAD subgroup [0.52 (0.31, 0.72) μg/ml versus 0.28 (0.20, 0.40) μg/ml, p = 0.001].
Kaplan–Meier survival curve analysis of all-cause mortality
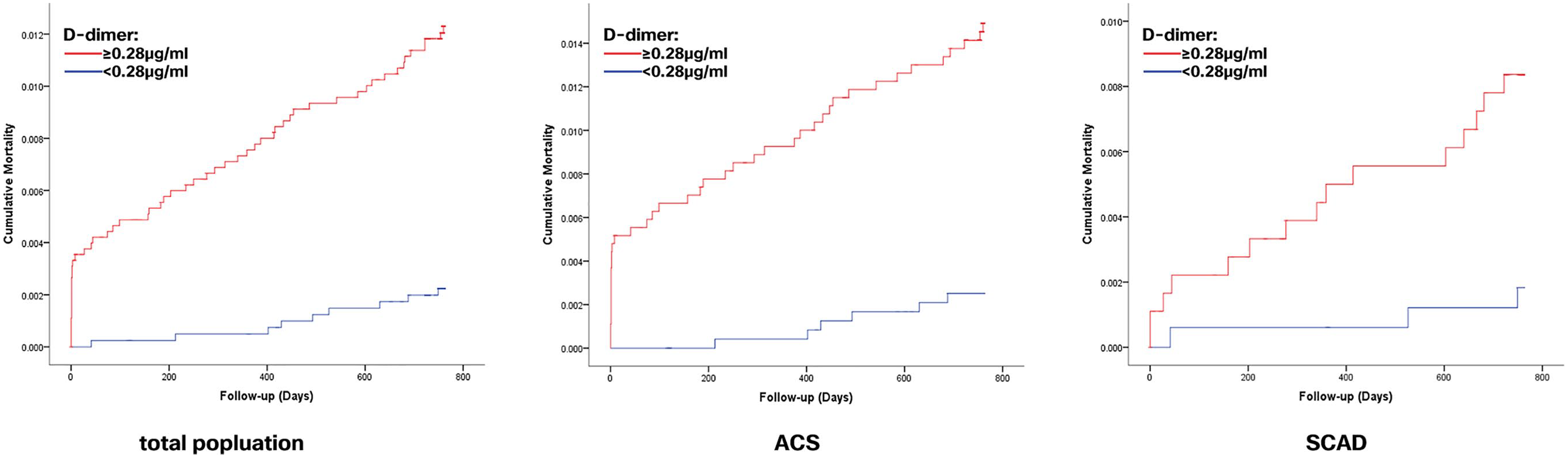
Kaplan–Meier survival curve analysis showed that, in the total population, ACS and SCAD subgroups, patients with high D-dimer levels had higher cumulative all-cause mortality according to the median D-dimer level (0.28 μg/ml) respectively (log-rank test, all p < 0.001, Figure 2).

Kaplan–Meier curves for all-cause mortality according to D-dimer levels. Kaplan–Meier curves show a significant difference in cumulative all-cause mortality rates when D-dimer levels had a cutoff point of 0.28 μg/ml in the total population, the ACS subgroup, and the SCAD subgroup (log-rank test, all p < 0.001).
Kaplan–Meier survival curve analysis of cardiac mortality
In the total PCI population, ACS and SCAD subgroups, the cumulative cardiac mortality rate between the two groups according to the median D-dimer level (0.28 μg/ml) was significantly different respectively (log-rank test, all p < 0.001, Figure 3).
Kaplan–Meier curves for cardiac mortality according to D-dimer levels. Kaplan–Meier curves show a significant difference in cumulative cardiac mortality rates when D-dimer levels had a cutoff point of 0.28 μg/ml in the total population, the ACS subgroup, and the SCAD subgroup (log-rank test, all p < 0.001).
COX regression analysis for assessing the risk of all-cause mortality
In Model 1, univariate analysis showed that high D-dimer levels were associated with a significantly higher rate of all-cause mortality (HR: 3.85; 95% CI: 2.42–6.12, p < 0.001). In Model 2, when adjusted for age and sex, D-dimer levels were still associated with mortality (HR: 2.52; 95% CI: 1.56–4.07, p < 0.001). In Model 3, age, sex, and risk factors after stepwise selection (only previous PCI, peripheral vascular disease, and LVEF were independently associated with all-cause death) were added to D-dimer levels, we found that D-dimer levels were still associated with all-cause mortality events (HR: 2.35; 95% CI: 1.44–3.84, p = 0.001) (Table 2).
Univariate and multivariate cox model analysis between D-dimer levels and all-cause mortality.

Model 1: Univariate Cox model analyses.
Model 2: The variables of age and sex were adjusted.
Model 3: Model 2 + previous PCI, peripheral vascular disease, and LVEF. Using stepwise regression, entry probability=0.05 and deletion probability = 0.10. The variables of age, sex, and D-dimer levels were forcedly introduced. With screening of body mass index, hypertension, diabetes, current smoking, hyperlipidemia, previous myocardial infarction, previous PCI, previous coronary artery bypass grafting, previous stroke, peripheral vascular disease, anemia, CrCl < 60 ml/min, LVEF, and the baseline SYNTAX score, only previous PCI, peripheral vascular disease and LVEF remained in the model.
ACS, acute coronary syndrome; CI, confidence interval; CrCl, creatinine clearance; HR, hazard ratio; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; SCAD, stable coronary artery disease.
For subgroup analysis, both in the ACS subgroup and SCAD subgroup, D-dimer levels were significantly associated with all-cause mortality in all of these models (Table 2).
COX regression analysis for assessing the risk of cardiac mortality
In Model 1, univariate analysis showed that D-dimer levels were associated with cardiac mortality (HR: 5.50; 95% CI: 2.72–11.13, p < 0.001) (Table 3). In Model 2, D-dimer levels remained significantly associated with mortality events, when adjusted for age and sex (HR: 3.61; 95% CI: 1.75–7.44, p < 0.001). In Model 3, we found that D-dimers were still significantly associated with cardiac mortality (HR: 3.44; 95% CI: 1.61–7.36, p = 0.001).
Univariate and multivariate Cox model analysis between D-dimer levels and cardiac mortality.

Model 1: Univariate Cox model analyses.
Model 2: The variables of age and sex were adjusted.
Model 3: Model 2 + previous PCI, peripheral vascular disease, and LVEF. Using stepwise regression, entry probability=0.05 and deletion probability=0.10. The variables of age sex, and D-dimer levels were forcedly introduced. With screening of body mass index, hypertension, diabetes, current smoking, hyperlipidemia, previous myocardial infarction, previous PCI, previous coronary artery bypass grafting, previous stroke, peripheral vascular disease, anemia, CrCl < 60 ml/min, LVEF, and the baseline SYNTAX score, only previous PCI, peripheral vascular disease, and LVEF remained in the model.
ACS, acute coronary syndrome; CI, confidence interval; CrCl, creatinine clearance; HR, hazard ratio; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; SCAD, stable coronary artery disease.
For subgroup analysis, in the ACS subgroup, D-dimer levels were associated with cardiac mortality events in all three models. In the SCAD subgroup, D-dimer levels were associated with cardiac mortality events in Model 1 (p = 0.016), but lost statistical significance in Models 2 (p = 0.086) and 3 (p = 0.094).
C-statistic analysis for assessing the value of risk prediction
The C-statistic of D-dimer for all-cause mortality was 0.69 (95% CI: 0.64–0.74), while that of cardiac mortality was 0.72 (95% CI: 0.66–0.78).
Discussion
To the best of our knowledge, this is the first large-sample systematic analysis of association of D-dimer levels and mortality in the PCI population. In patients who underwent PCI, higher baseline D-dimer levels were significantly associated with the risk of all-cause mortality and cardiac mortality. This association was independent of multiple traditional factors. In subgroup analysis, D-dimer levels were independently associated with all-cause mortality in the ACS and SCAD subgroups. D-dimer levels were independently associated with cardiac mortality in the ACS subgroup, but lost statistical significance in the SCAD subgroup.
Our study showed that patients who underwent PCI with higher D-dimer levels at admission were significantly associated with a risk of all-cause mortality and cardiac mortality, and D-dimer levels had prognostic value in assessing the risk of mortality in the PCI population. Previous studies have shown that D-dimer levels have prognostic value in patients with pulmonary embolism and deep vein thrombosis.3,4 Specifically, elevated D-dimer was associated not only with a higher risk of deep vein thrombosis, but also the extent of involvement (i.e. thrombus burden) in hospitalized patients. 14 Furthermore, in light of its prognostic value, D-dimer measurement has been incorporated into risk assessment models for venous thromboembolism to enhance the accuracy of VTE prediction. 15 Recently, D-dimer levels were found to be useful for prognosis in atrial fibrillation, 16 cancer,5,6,17 infection, 18 peripheral vascular disease, 19 aortic dissection, 8 and stroke. 7 Our study showed that D-dimer levels had prognostic value for the risk of all-cause and cardiac mortality in patients with PCI. This finding suggests that clinicians should pay more attention to patients with high D-dimer levels who might face a high mortality risk. D-dimer is a convenient, economical, and routinely tested blood parameter in clinical practice, which can help clinicians identify high-risk patients with PCI, thus having potential clinical practical value.
The mechanism of how D-dimer can predict mortality is unclear. D-dimer levels reflect increased coagulation and fibrinolytic activity. 1 Elevation of D-dimer levels is associated with some pathological processes, including thrombosis, 1 plaque necrosis, 20 infection, 18 and cancer metastasis, 5 which may make it an independent risk marker for all-cause mortality and cardiovascular mortality.
Using our large-sample database, further analyzed results showed that D-dimer levels predicted all-cause mortality in the ACS and SCAD subgroups. While D-dimer levels predicted cardiac mortality in the ACS subgroup, they lost statistical significance in the SCAD subgroup. Previous studies on D-dimer focused mostly on patients with ACS. Most studies supported the association of higher D-dimer levels with a poor prognosis. Sarli and colleagues (266 patients) 9 and Kikkert and colleagues (461 patients) 10 reported that D-dimer levels were an independent predictor of major adverse cardiac events in patients with ST segment elevated acute myocardial infarction (STEMI); Akgul and colleagues showed that admission D-dimer levels were associated with increased in-hospital cardiovascular mortality and 6-month all-cause mortality in 453 patients with STEMI. 11 However, Tello-Montoliu reported that there was no correlation between D-dimer levels and adverse events in 358 patients with non-ST elevation ACS after 6 months of follow up. 21 In a recent study of the ATLAS ACS-TIMI 46 trial, 22 D-dimer was positively related to the risk of cardiovascular death, MI, and stroke at 6 months of follow up. Additionally, the study suggested that administration of the factor Xa inhibitor rivaroxaban was associated with lower D-dimer levels compared with placebo. Using a large sample size, our study was consistent with the result that D-dimer was an independent risk marker for all-cause and cardiac mortality in patients with ACS who underwent PCI.
Previous studies of D-dimer in SCAD are limited. A recent study by Simes and colleagues investigated a large sample in the LIPID study for SCAD. 12 They showed that D-dimer was a significant long-term predictor of cardiovascular and cancer mortality. However, there are differences in some aspects between our study and that of Simes and colleagues. 12 Our study was in the PCI population, while that of Simes and colleagues did not indicate whether the patients received PCI or CABG revascularization therapy. 12 Although the patients in the LIPID study were defined as having SCAD, the criteria for inclusion were only those who had acute myocardial infarction, or had a hospital discharge diagnosis of unstable angina between 3 and 36 months before study entry. 12 The LIPID study was performed 20 years ago and does not accurately reflect current treatment levels of coronary heart disease. 23 Our study showed that D-dimer levels still had a good independent association with prognosis of 2-year all-cause mortality in patients with SCAD who received PCI, dual antiplatelet therapy, and statin therapy in the modern drug-eluting stent era. However, after multivariate adjustment, D-dimer levels lost statistical significance for cardiac mortality. This finding may be related to the relatively low rates of cardiac death in patients with SCAD, and PCI revascularization treatment further reduces the incidence of events. The predictive value of D-dimer levels for cardiac mortality in SCAD requires further study.
Previous studies have shown that age and smoking can affect D-dimer levels.24–26 D-dimer levels also increase in stroke, 27 diabetes, 28 renal insufficiency, 29 and other diseases. However, whether D-dimer levels can predict the risk of mortality independent of these factors is unknown. Our study included multiple traditional clinical risk factors and the baseline SYNTAX score. We found that, after multivariate analysis, D-dimer levels were still independently associated with all-cause and cardiac mortality.
Precise therapeutics is currently a hot topic. Previous studies have shown that use of anticoagulant therapy in patients with ACS reduces D-dimer levels, reduces death and myocardial infarction events, but also increases the risk of bleeding.30–32 Our study showed that patients who underwent PCI with high D-dimer levels had a significantly increased risk of mortality, this suggests that D-dimer is a potential marker of poor prognosis in patients with PCI. In the future, whether D-dimer levels can be used to identify high-risk patients undergoing PCI and provide more precise new oral anticoagulants treatment based on antiplatelet therapy, thereby reducing the risk of mortality in patients with PCI, should be further studied.
Limitations
Some potential limitations of our analysis should be considered. First, our study was a single-center, observational study, which may limit the generalizability of its findings. Second, we measured D-dimer levels only at the time of admission to hospital and did not further test D-dimer levels after treatment or discharge. Therefore, the predictive value of dynamic detection of D-dimer levels for mortality requires further study. Third, as mentioned in study protocol, 2109 were excluded from current analysis because of the missing D-dimer data, which might affect the results. Fourth, the findings here may be affected by unmeasured confounders. Although we tried to control for multiple variables, there may still be some that could have been missed. Fifth, in the future, more research is needed to validate these results.
Conclusion
In this real-world large sample study, elevation of D-dimer levels is a strong independent risk factor for all-cause and cardiac mortality in patients with PCI, thus having potential clinical practical value. Whether D-dimer levels can be used in clinical practice to guide precise anticoagulation therapy in patients with PCI requires further study.
Footnotes
Author contributions
ZXY, CJ, QSB, YYJ, GRL, XB, and YJQ contributed to the conception or design of the work. LJX, TXF, and JL contributed to the acquisition, analysis, or interpretation of data. ZXY drafted the manuscript. XB and YJQ critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
This study was supported by grants from the National Key Research and Development Program of China (No. 2016YFC1301300 and No. 2016YFC1301301).
Conflict of interest statement
The authors declare that there is no conflict of interest.