
Abstract
Background:
Exercise intolerance is a common phenotype observed in patients with cystic fibrosis (CF). Treatment with sildenafil, a phosphodiesterase type 5 (PDE5) inhibitor, has previously been shown to improve exercise capacity (VO2 peak) in other patient populations. Thus, the present study sought to determine the acute and subacute effects of sildenafil on exercise capacity in patients with CF.
Methods:
The present investigation utilized a randomized, double-blind, placebo-controlled, crossover study with an acute dose of either sildenafil (50 mg) or placebo (n = 13, age 25 ± 10), followed by a 4 week open-label extension with sildenafil (20 mg, TID; n = 15, age 23 ± 11). A comprehensive evaluation of pulmonary function and a maximal exercise test were each performed at every visit.
Results:
A significant increase in VO2 peak was observed after the acute sildenafil dose with no changes following placebo (77 ± 13 versus 72 ± 13% predicted; p = 0.033). In addition, after 4 weeks of treatment, patients showed a significant increase in exercise capacity (72 ± 12 versus 75 ± 12% predicted; p = 0.028) and exercise duration (409 ± 98 versus 427 ± 101 s; p = 0.014). A robust correlation (r = 0.656; p = 0.008) between baseline FEV1 (% predicted) and the change in exercise capacity following 4 weeks of treatment was identified.
Conclusions:
This proof-of-concept clinical trial demonstrates that sildenafil treatment can improve exercise capacity in patients with CF and that pulmonary function may play an important role in the effectiveness of treatment. Future investigations of sildenafil treatment in patients with CF are certainly warranted.
Introduction
Cystic fibrosis (CF) is the most common fatal genetic disease, caused by a mutation in a gene responsible for encoding the cystic fibrosis transmembrane conductance regulator (CFTR) protein. Due to the ubiquitous expression of CFTR in many different tissues, patients with CF not only present with pulmonary dysfunction but also many systemic manifestations, such as gastrointestinal, immune, endocrine, and musculoskeletal dysfunctions.
Exercise intolerance is a common phenotype observed in patients with CF.1,2 Maximal oxygen consumption (VO2 peak) is an objective assessment of exercise tolerance and has been shown to predict mortality in patients with CF, independent of lung function.3,4 A common assumption is that pulmonary dysfunction is the main factor contributing to exercise intolerance in patients with CF. However, nutrition status, muscle dysfunction, genotype, physical activity status, gender, and psychosocial influences 5 have all been shown to contribute to exercise intolerance in this patient population.
In vitro experiments using sildenafil, a phosphodiesterase type 5 (PDE5) inhibitor, have demonstrated improvements in chloride channel function6,7 at the apical membrane by rescuing F508del-CFTR trafficking. 8 Clinically, sildenafil decreases sputum neutrophil elastase activity, a biomarker of pulmonary inflammation, in patients with CF. 9 In addition, sildenafil increases blood flow to and within skeletal muscles 10 and improves exercise performance in patients with chronic heart failure (CHF).10,11 Whether or not patients with CF can benefit from sildenafil treatment is unknown. Accordingly, the present study sought to test the hypothesis that sildenafil treatment would improve exercise capacity in patients with CF.
Materials and methods
Ethical approval
All study protocols were approved by the Human Assurance Committee at Augusta University (No. 10-07-019), and written and verbal informed assent/consent was obtained from all patients and parents of minors prior to participation. The study followed the principles of the Declaration of Helsinki.
Experimental design
There were two phases to this investigation [ClinicalTrials.gov identifier NCT02057458; registered 4 February 2014]: (1) a randomized, double-blind, placebo-controlled, crossover study with an acute dose of either sildenafil (50 mg) or placebo; and (2) a 4-week open-label extension with 20 mg of sildenafil thrice daily. The dosing for both phases of the current study was selected based on the prevailing literature evaluating sildenafil in other populations.12–14
Participants were asked to report to the Laboratory of Integrative Vascular and Exercise Physiology (LIVEP) at Augusta University for a preliminary visit and three separate experimental visits. The preliminary visit (baseline) consisted of the informed consent process, body composition assessments, a comprehensive pulmonary function test (PFT), and a maximal exercise capacity test. For phase I, patients reported to LIVEP on two separate experimental visits, separated by at least 1 week, and received an acute oral dose of either sildenafil or placebo. Exercise capacity was assessed 1 hour following the acute treatment. All treatments were blinded and dispensed by the Augusta University Medical Center Pharmacy following a randomization scheme with a block size of two. The details of the series were unknown by any of the investigators involved in the study. Importantly, the plasma half-life of sildenafil is approximately 4 h. Accordingly, at least 1 week between doses is sufficient to ensure that there are no carry-over effects.
For phase II, patients were instructed on the use and adverse events of a prolonged treatment with sildenafil, and started the 4-week open-label extension the following day. Within 48 h of the first open-label dose, research staff conducted a follow-up phone call. Following 4 weeks of treatment with sildenafil, follow-up testing of the same baseline assessments was again conducted within 48 h of the patient’s last treatment dose. Throughout the intervention, patients were instructed to adhere to the timing of their daily airway clearance and inhaled treatments as well as to maintain their daily routine for physical activity.
Patients
An initial power calculation was performed based on the anticipated effect size estimated for the primary outcome variable (exercise capacity) from previous studies.12,14 The initial proposed sample size yielded power ⩾0.87 in all the primary outcomes for the present study. It is noteworthy that the studies upon which we based our initial sample size calculations used similar protocols to evaluate the impact of sildenafil on exercise capacity, but in a different population (patients with heart failure with an average of 12 ml/kg/min less than our cohort) and using different dose and/or length of treatment. Power analysis and sample size were recalculated before initiating the study, considering that under most circumstances an α = 0.05 and a statistical power ⩾0.85 is well accepted.
Figure 1 illustrates the clinical trial flow chart. A total of 19 participants were recruited from the patients that attend Augusta University Cystic Fibrosis Center using study flyers and word of mouth. All interested patients completed a screening visit to verify inclusion and exclusion criteria. Recruitment was limited to clinically stable patients with a clinical diagnosis of CF (both positive sweat tests and genotype analysis) and a forced expiratory volume in one second (FEV1) greater than 30% predicted. Potential participants were excluded if they had a resting oxygen saturation (SpO2) lower than 85%, were diagnosed with pulmonary hypertension, sleep apnea, sleep disorders, migraine headaches, cardiovascular disease, hypertension, or CF-related diabetes, and they were prescribed any vasoactive medications (i.e. nitrates, beta-blockers, angiotensin-converting enzyme inhibitors, etc.). Potential participants were also excluded if they self-reported to be smokers. Inclusion and exclusion criteria were evaluated by study physicians. From the initial 19 participants, all were eligible to participate with the exception of 1.
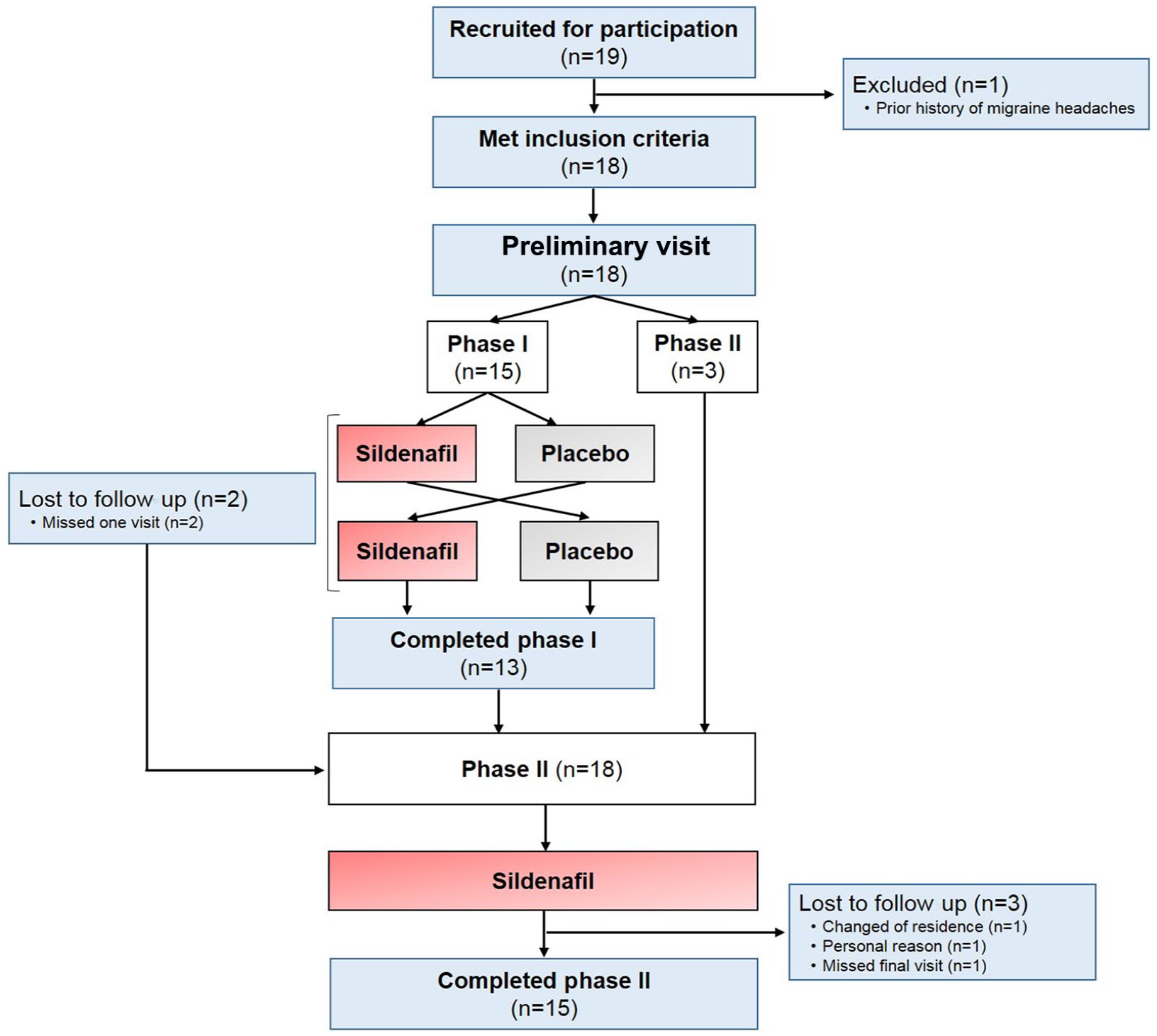
Clinical trial flow chart.
Of the 18 patients recruited, only 15 enrolled in the phase I study, of which 13 completed the acute protocol. All 18 patients were enrolled in the phase II open-label extension; however, 3 withdrew from the study, resulting in a total of 15 patients completing the 4 weeks of treatment.
Body composition
Patient testing included standard anthropometric assessments of height, weight, and calculated body mass index (BMI). Detailed body composition, including fat mass, fat-free mass (FFM), and bone mineral content, was determined using dual-energy X-ray absorptiometry (DXA; QDR-4500W; Hologic Inc. Marlborough, MA, USA).
Pulmonary function test
A comprehensive evaluation of pulmonary function testing was conducted in all patients using the EasyOne Pro LAB (ndd Medical Technologies, Andover, MA, USA) according to the American Thoracic Society/European Respiratory Society guidelines. Ultrasonic sensor spirometry was conducted to obtain FEV1, forced vital capacity (FVC), FEV1/FVC ratio, and forced expiratory flow at 25–75% (FEF25–75). In addition, at baseline and at the end of the 4 weeks of treatment with sildenafil, diffusing capacity for carbon monoxide (DLCO; EasyOne Pro LAB), lung clearance index (LCI; EasyOne Pro LAB, Zurich Switzerland), and exhaled nitric oxide (eNO; NIOX MINO®, Niox, Solna, Sweden) were also evaluated. The European Respiratory Society Global Lung Function Initiative spirometric reference standards 15 were used to determine the percentage predicted data set.
Maximal exercise test
On each experimental visit, patients completed a maximal exercise test using the Godfrey protocol on an electronically braked cycle ergometer (Lode Corival or Lode Corival Pediatric; Lode BV, the Netherlands). Briefly, following 2 min of rest and 2 min of subsequent unloaded cycling (warm-up), exercise intensity was increased by 15–20 watts (based on patient’s height) every 1 min until volitional fatigue. Heart rate via chest strap (Polar, Lake Success, New York, NY) and fingertip SpO2 (Nonin Avant 4000, Nonin, Plymouth, MN) were monitored continuously. Blood pressure was measured on the left arm during each stage of the protocol (Suntech Tango+, Suntech Medical, Morrisville, NC). Expired gases were collected breath by breath by the TruOne 2400 metabolic cart (Parvo Medics, Sandy, UT) and 30 s averages were utilized to obtain VO2 peak. Maximal exercise capacity was verified using the American College of Sports Medicine exercise testing criteria. 16 Specifically, a test was considered maximal if the patient met three out of the four following criteria: (1) volitional fatigue (>17 on ratings of perceived exertion); (2) a plateau in oxygen uptake; (3) achieving >85% of predicted heart rate max; and (4) a respiratory exchange ratio (RER) greater than 1.1.
Data analysis
All analyses were performed using SPSS, version 23.0 (IBM Corporation, Armonk, NY). The Shapiro–Wilk test was used to assess the normality of distribution of the data. Two-tailed paired t tests were performed on all variables to identify differences between sildenafil and placebo and between baseline and 4 weeks of sildenafil treatment. Two-tailed independent group’s t tests were performed to identify differences in the change in exercise capacity between disease severity groups. For the data obtained from the second phase, an analysis of covariance (ANCOVA) was used to control exercise capacity for lung function. Pearson correlation analyses were performed to identify associations among primary outcome variables. Values are presented as mean ± SD unless otherwise noted. A p < 0.05 was considered statistically significant for all analyses. Cohen’s d or partial eta squared (ηp2) were used to report effect sizes of the primary outcomes for t tests and ANCOVA respectively, to represent small (Cohen’s d = 0.2; ηp2 = 0.01), medium (Cohen’s d = 0.5; ηp2 = 0.06), and large (Cohen’s d = 0.8; ηp2 = 0.13) effect sizes.17,18
Results
Participant characteristics and body composition
A total of 13 patients completed phase I, while 15 completed phase II. The majority of patients were homozygous ∆F508del; however, one patient was ∆F508/621+1G->T and another was ∆F508/G551D. Due to time commitment and travel distance, three patients decided to participate only in phase II. Sildenafil therapy was well tolerated among all patients throughout the entire study. No serious adverse events were reported and the side effects were usually mild and consistent with those previously reported and indicated on the label. Patients’ characteristics for both phases are presented in Table 1. Characteristic data collected during the preliminary visit are presented under Baseline. Data obtained at each acute treatment day are presented under phase I, whereas the patient characteristics following 4 weeks of treatment with sildenafil are reported under phase II. No differences in any of the participant characteristics were observed between visits. DXA analysis was only conducted at baseline due to the unanticipated changes in body composition with short-term treatment.
Patient characteristics.

Values are mean ± standard deviation. BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Pulmonary function testing
Results from a comprehensive assessment of pulmonary function for both phase I and II are presented in Table 2. Baseline FEV1 ranged from 49% to 103% predicted, representing preserved to moderate lung disease severity. For phase II, no significant (p = 0.272) changes in spirometric function were identified following 4 weeks of sildenafil treatment. Similarly, no changes were observed for DLCO, LCI, or eNO.
Pulmonary function at baseline and following treatment.

Values are mean ± standard deviation. DLCO, diffusing capacity for carbon monoxide; eNO, exhaled nitric oxide; FEF25–75, forced expiratory flow; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; LCI, lung clearance index; LLN, lower limit of normality.
Maximal exercise test parameters
Maximal exercise test parameters for both phase I (sildenafil versus placebo) and phase II (baseline versus 4 weeks) are presented in Table 3. Given that one participant did not achieve a true maximal test following the criteria defined by the American College of Sport Medicine, 19 all values are expressed as VO2 peak. Figure 2 illustrates a significant (p = 0.033; Cohen’s d = 0.67) improvement in VO2 (% predicted) after the acute dose of sildenafil when compared with placebo.
Peak exercise test parameters.

Values are mean ± standard deviation. RER, respiratory exchange ratio; VCO2, volume of carbon dioxide; VE, Ventilation; VO2, volume of oxygen consumption; VT, ventilatory threshold. CI = 95% confidence interval for difference. * Significant (p < 0.05) difference between sildenafil and placebo. † Significant (p < 0.05) difference between baseline and 4 weeks of sildenafil treatment. ‡ Significant (p < 0.05) after controlling for baseline FEV1 (% predicted).
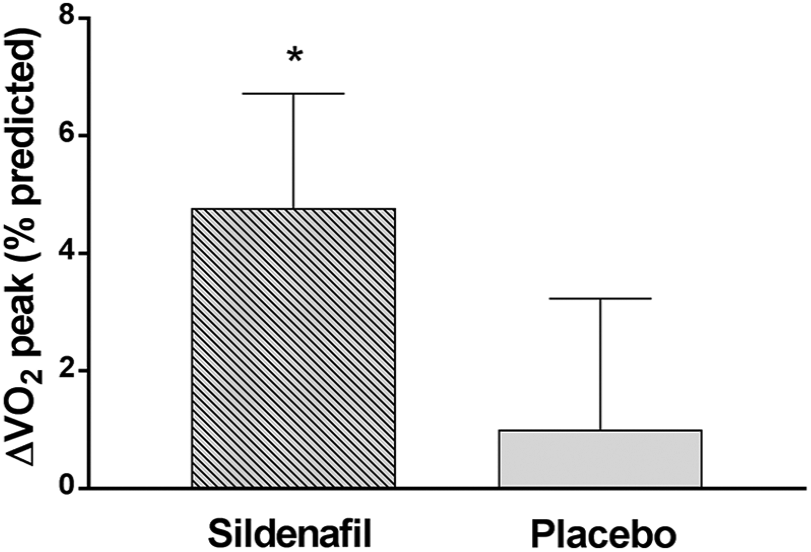
Change in exercise capacity in patients with cystic fibrosis after an acute dose of either sildenafil or placebo (N = 13).
Furthermore, after 4 weeks of treatment with sildenafil, a significant (p = 0.028; ηp2 = 0.319) increase in VO2 peak (% predicted) after controlling for lung function (baseline FEV1; Figure 3(a)) was observed. Specifically, as illustrated in Figure 3(b), nine patients showed a marked increase in exercise capacity after 4 weeks of treatment (+0.4 to +6.5 ml/kg/min), three patients showed similar VO2 peak (−0.1 to 0.2 ml/kg/min), while the other three exhibited a decrease in exercise capacity after completing phase II (−1.1 to −4.4 ml/kg/min). No order effect (p = 0.384) from phase I impacting results of phase II was identified. Exercise duration (p = 0.014; Cohen’s d = 0.73) and peak pulmonary ventilation (p = 0.008; Cohen’s d = 0.80) were both significantly greater after completing the 4 weeks of treatment. Moreover, peak RER during maximal exercise was significantly (p = 0.036; Cohen’s d = 0.60) lower following 4 weeks of sildenafil treatment. No differences (p ⩾ 0.895) in SpO2 were observed during maximal exercise before and after any treatment from phase I and after completing phase II.

Exercise capacity in patients with cystic fibrosis (a) at baseline and following 4 weeks of sildenafil (N = 15); and (b) individual change after 4 weeks of treatment with sildenafil (N = 15).
Relationship among exercise parameters and pulmonary function
A significant, strong, positive relationship was observed between baseline FEV1 (% predicted) and the change in relative VO2 peak after 4 weeks of treatment with sildenafil ( r = 0.656; p = 0.008; Figure 4). In a subsequent analysis, patients who completed phase II were equally separated into two groups based on initial status of disease severity:20,21 FEV1 ⩾85% predicted (N = 8) and FEV1 <85% predicted (N = 7). Those patients with a preserved pulmonary function exhibited a significantly (p = 0.012) greater improvement in VO2 peak compared to patients with mild-to-moderate pulmonary function (3.0 ± 2.7 versus −0.61 ± 2.0 ml/kg/min, respectively). The same analysis was completed separating patients into two groups based on lower limit of normality (LLN). 22 FEV1 ⩾ LLN (N = 8) and FEV1 < LLN (N = 7). Similarly, patients that exhibited a lung function above LLN also had a significantly (p = 0.026) greater improvement in exercise capacity than those with a nonpreserved lung function (2.9 ± 2.8 versus −0.45 ± 2.1 ml/kg/min, respectively). Importantly, age was not associated with the change in VO2 peak (r = −0.324; p = 0.259) and does not impact the aforementioned results.

Relationship between baseline FEV1 (% predicted) and changes in exercise capacity following four weeks of sildenafil on patients with cystic fibrosis (N = 15, r = 0.656, p = 0.008).
Discussion
Lower exercise capacity, an independent predictor of mortality in CF, is a common phenotype observed in this patient population.3,4 The efficacy of sildenafil to rescue CFTR function8,23 and improve its activity6,7 has previously been documented in preclinical studies. To our knowledge, this is the first study to identify an increase in exercise capacity following either an acute dose or a 4-week treatment with sildenafil in patients with CF. In addition, the change in exercise capacity following subacute treatment was positively associated with baseline spirometric function. Findings from the present study offer proof-of-concept for the use of sildenafil to improve exercise capacity in patients with CF and support the need for longer interventions and larger clinical trials using PDE5 inhibitors to improve longevity in this patient population.
Exercise capacity and sildenafil therapy
Maximal exercise testing in patients with CF can add substantial prognostic value over traditional assessments of pulmonary function due to its integration of multiple biological systems (i.e. pulmonary, cardiovascular, and neuromuscular). Additionally, exercise capacity has been established as an independent predictor of mortality in CF.3,4 Accordingly, interventions that improve, or even slow the declining rate of, exercise capacity over time are needed in CF to help contribute to increased survival rates in this patient population.
Sildenafil has been proposed as a potential therapy for CF due to its dual role increasing blood flow to and within muscles 10 and improving CFTR function.6,7 Sildenafil is safe 9 and has demonstrated efficacy in exercise tolerance related manifestations of a patient with advanced CF. 24 Findings from the present study extend those results and for the first time document a significant increase in exercise capacity after a single dose of sildenafil, with a sustained improvement following 4 weeks of treatment with sildenafil. Even more significant, the observed improvement after sildenafil treatment is equivalent to a 60% increase above the expected annual decline in exercise capacity in patients with CF. 3 These data highlight the clinical impact that sildenafil treatment may have on counteracting exercise intolerance in this patient population. Our results are in agreement with a previous study that reported a 13% increase in VO2 peak following 4 weeks of sildenafil treatment in patients with CHF. 11 In the present study, exercise capacity increased an average of 4.7% after 4 weeks of treatment; however, it is important to note that the change in VO2 peak following the subacute sildenafil treatment ranged between −14.8% and +29.5%. Two distinct differences exist between the present study and the one conducted in patients with CHF: (1) the patient population and (2) the treatment dose of sildenafil. In our study, patients with CF exhibited a considerably higher baseline exercise capacity (~28 ml/kg/min) compared to what has previously been reported in patients with CHF (~16 ml/kg/min). 11 Disparity in disease may impact baseline exercise capacity, and given the concept of a basement effect, patients with CHF may have had more to gain following treatment with sildenafil than our patients with CF. Additionally, in the present study, patients with CF were prescribed a single dose of 50 mg of sildenafil for phase I that was followed by a treatment with 20 mg of sildenafil, three times daily based on clinical indications for pulmonary artery hypertension. Notably, this open-label dose was 1.5 times less than the dose of sildenafil that was given to patients with CHF (50 mg of sildenafil, three times daily). Consequently, it is conceivable that a higher dose of sildenafil could result in greater improvements in exercise capacity in CF; however, future studies are needed to test this hypothesis.
The metabolic response and sildenafil therapy
The duration of the cardiopulmonary exercise testing (CPET) also represents an important criterion when measuring exercise tolerance. 25 Bearing in mind that patients with pulmonary diseases typically exhibit an early onset of lactic acid accumulation, 26 the ability to exercise longer may be a result of less lactic acid accumulation, reduction in expired VCO2, lower peak RER, and an overall improvement in VO2.27,28 A reduction in RER at peak exercise, a marker of metabolic response in patients with reduced exercise tolerance, 27 has been associated with improvements in exercise capacity. 29 Indeed, patients with CF exhibit a decreased lipid metabolism 30 associated with mitochondrial dysfunction and impaired cellular oxygen consumption.31,32 Our findings are in agreement with a previous in vitro study that demonstrated the improvements of fatty acid β oxidation and mitochondrial protein expression in skeletal muscle tissue with sildenafil. 33 Moreover, a lower RER during exercise is related with improved muscle performance due to the ability to match fatty acid and glucose oxidation. 27 Taken together, the present findings indicate that treatment with sildenafil contributes to a greater proportion of lipid metabolism during maximal effort, improving skeletal muscle metabolism and oxygen uptake and resulting in later onset of fatigue.27,34
Improvement in exercise capacity and pulmonary function
Changes in pulmonary function do not always result in changes in exercise capacity and vice versa. Thus, clinical evaluation of both pulmonary function and exercise capacity is essential in monitoring disease severity in patients with CF, especially in those with preserved lung function. 35 In the current study, although an improvement in exercise capacity was observed, there were no changes in spirometric function between the different visits. In addition, no changes were observed for DLCO, LCI, or eNO, supporting that 4 weeks of sildenafil therapy did not impact pulmonary hemodynamics. 36 Notwithstanding, a strong significant correlation between baseline spirometric function and the change in exercise capacity following 4 weeks of treatment was identified. Therefore, those patients with a better pulmonary function exhibited a greater improvement in exercise capacity following sildenafil treatment. These findings are somewhat paradoxical because one might expect a greater treatment response in patients who have worse disease severity, as previously observed in patients with CHF. 11 However, different mechanisms for exercise intolerance exist among patients with CF of varying disease severity and it is not surprising that those patients with a more severe disease status have already developed other dysfunctions that may contribute to exercise intolerance. Indeed, in severe CF phenotypes, FEV1 has previously been reported as the primary predictor of exercise intolerance. 37 On the other hand, in patients with mild-to-moderate disease the extent of the ventilator response (excessive dynamic hyperventilation) during exercise influences central (cardiovascular) and peripheral (muscle) factors that influence exercise intolerance.37,38 Thus, the relationship between baseline spirometric function and exercise capacity demonstrates that disease severity plays an important role in the effectiveness of sildenafil treatment in CF. Importantly, controlling for age did not impact this relationship, indicating that early intervention in CF may be more beneficial and therapy should be initiated at first signs of diminishing exercise capacity when lung function is still preserved. Longer duration and larger clinical trials, however, are certainly warranted to investigate the effectiveness and safety of sildenafil in patients with CF of varying genotypes and disease severity because of the limited sample size in the present study.
Effectiveness of sildenafil treatment versus exercise training interventions
Many studies have investigated the effectiveness of exercise training as a therapy to improve exercise capacity in CF. In fact, both aerobic and anaerobic exercise training have been shown to improve exercise tolerance in patients with CF;39–42 however, a wide range of efficacy has been reported. Specifically, children with CF (ages 9–18 years) exhibited a 5% increase in maximal exercise capacity following 12 weeks of anaerobic training, 41 similar to the ~5% improvement observed in the present study after 4 weeks of sildenafil. In contrast, after a 12-week aerobic training program, younger adults with CF (mean age 21 years) showed an increase in maximal exercise capacity of 16.2%. 42 Although the improvement in VO2 peak after this aerobic exercise training was greater compared with the modest increase we observed following sildenafil treatment, it is important to note that the duration of exercise training was much longer than our protocol, and treatment duration could certainly play an important role. Interestingly, both sildenafil (through improvement in CFTR expression and activity6–8,23) and exercise training (through multiple mechanisms such as improved cardiovascular function and greater vascular transport capacity of skeletal muscle 43 ) can improve muscle perfusion and function. Perhaps including sildenafil therapy at the commencement of an exercise training program will not only reduce fatigue, but also boost the blood flow and energy metabolism and contribute to greater improvements in exercise capacity compared with each therapy alone. 44 Nonetheless, future investigations into the effect of chronic treatment of sildenafil on muscle function and resultant exercise capacity are warranted.
Clinical application
Considering that patients used to exhibit an annual decline in exercise capacity of ≈2.1 ml/kg/min, 4 any alternative to diminish this deterioration or even to improve exercise capacity strongly benefit the patient’s quality of life and survival. 4 Exercise training is effective at improving exercise capacity/tolerance; however, the average adult patient with CF spends ~90 min/day on CF-related therapies and airway clearance, regardless of age or disease severity. 45 Accordingly, many patients (1) may perceive exercise as an additional treatment burden reducing compliance; 46 and/or (2) may feel earlier and more severe fatigue during physical activity and lead to a more sedentary lifestyle. 44 According to Harter, 47 the greater degree of perceived ability could play an important role in better compliance with exercise training. Based on the present findings, sildenafil could potentially be prescribed as an initial treatment to patients with CF, promoting the willingness to be active through a reduced perception of dyspnea. Additionally, using the Cystic Fibrosis Questionnaire Revised (CFQ-R), a disease-specific tool to measure the overall perceived health, patients reported positive changes in five domains describing quality of life and disease perception after 4 weeks of sildenafil. Specifically, from eight adult patients that completed the CFQ-R, a significant improvement was reported in the emotion domain (∆ = 4.2 ± 1.8; p = 0.049) along with an improvement in the digestion domain (∆ = 5.6 ± 2.9; p = 0.104) after just 4 weeks of treatment. Although results are positive, future studies are warranted to investigate the long-term impact of sildenafil therapy and to determine if treatment in this patient population can (1) sustain the increase in exercise capacity, (2) enhance the results of exercise training, and (3) result in greater compliance with exercise training interventions. The ultimate goal will be to improve quality of life and longevity in patients with CF.
Experimental considerations
The present study represents an initial step toward understanding the potential role that sildenafil may play in improving exercise tolerance in patients with CF. However, as many other preliminary investigations, there are some limitations to consider when interpreting the data. For example, the present investigation utilized a randomized, placebo-controlled, crossover experimental design with an acute dose of sildenafil or placebo followed by an open-label extension. Although the lack of placebo treatment in phase II has to be considered when understanding the results of the present study, we have included additional analyses to reinforce our interpretation and rule out the possibility of inherent variations during phase II. Specifically, reproducibility of exercise capacity in CF has previously been reported over a 28-day period. 48 In addition, VE/VCO2 ratio, a marker of reliability between exercise tests that is effort-independent, 49 was also reproducible between the different visits of the present study. Perhaps more importantly, we have demonstrated the reliability of the maximal exercise test protocol in our laboratory using a separate observational cohort of 16 patients with CF (10 of whom also participated in the current study) at baseline and after 3 months. The intraclass coefficient of variation (0.983; p < 0.001), correlation coefficient (r = 0.969; p < 0.001), coefficient of variation (18.6), and mean difference (0.137 ± 0.574; p = 0.817) for VO2 peak between both visits indicate no change in exercise capacity in patients with CF throughout a 3-month period. In addition, no significant changes in exercise duration (p = 0.337), RER peak (p = 0.318), or VE peak (p = 0.202) were observed. Similarly, no changes were observed in pulmonary function parameters as well as in DLCO, LCI, or eNO, suggesting that sildenafil therapy did not impact pulmonary hemodynamics. 36 Although similar results have been previously observed, future studies may need to evaluate the role that disease severity as well as CF genotype play in the treatment effect of sildenafil on exercise tolerance.
Conclusion
In conclusion, for the first time our data documents an improvement in exercise capacity following both an acute dose and 4 weeks of sildenafil treatment in patients with CF. Indeed, pulmonary function prior to treatment could play a role in the efficiency of sildenafil to improve exercise capacity in CF. The present findings support proof-of-concept for the use of sildenafil to improve exercise tolerance in CF. These results could possibly represent an initial therapeutic approach to improve exercise capacity in patients with CF with the use of an already FDA-approved treatment. Future studies are certainly needed to evaluate the most effective dose, duration, and impact of PDE5 inhibition to better understand the treatment efficacy on exercise capacity in CF.
Footnotes
Acknowledgements
The authors would like to thank all of the patients and patients’ families for their commitment to this research investigation. Special acknowledgment goes to the Pediatric and Adult CF Center teams at Augusta University for assisting with patient recruitment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Health/National Institute of Diabetes and Digestive and Kidney Diseases (NIH/NIDDK R21DK100783, RAH).
Conflict of interest statement
The authors declare that there is no conflict of interest.