
Abstract
Background:
Observational studies suggest that patients with immunoglobulin A nephropathy (IgAN) showed good responses to corticosteroids (CS) but experienced severe adverse effects. The authors conducted a cohort study to evaluate the effectiveness and safety of half-dose CS plus renin-angiotensin system blockers (RASB) (CS + RASB) versus full-dose CS in IgAN patients.
Methods:
A total of 162 kidney biopsy-confirmed IgAN patients with protein excretion levels ⩾0.75 g/d and an estimated glomerular filtration rate (eGFR) >30 ml/min/1.73 m2 were included. A total of 89 patients received half-dose CS + RASB (half CS + RASB), and 73 patients received full-dose CS (full CS). The primary outcomes were the complete remission rates and incidence of adverse events (AEs). The secondary outcomes included 24 h urinary protein (UP) levels and a combined event.
Results:
Over the 18 months follow-up, the complete remission rates were 59% (53/89 patients) and 57% (42/73 patients) in the half CS + RASB and full CS groups (p = 0.88), respectively. A total of five patients suffered from serious AEs (SAEs) in the full CS group during the observation period, and no SAEs were observed in the half CS + RASB group (p = 0.012). The incidences of total AEs (p = 0.003) and infections (p = 0.01) were lower in the half CS + RASB group than in the full CS group.
Conclusions:
Although half CS + RASB versus full CS did not differ in terms of reducing proteinuria, therapy with half CS + RASB resulted in fewer AEs in the IgAN patients.
Introduction
As a widespread glomerular disease, immunoglobulin A nephropathy (IgAN) is an important cause of end-stage renal disease (ESRD) worldwide.1,2 The 2012 Kidney Disease Improving Global Outcomes (KDIGO) guidelines regarding IgAN suggested that patients with persistent proteinuria ⩾1.0 g/d despite 3–6 months of intensive supportive care and an estimated glomerular filtration rate (eGFR) >50 ml/min per 1.73 m2 should use systemic glucocorticoids. 3 Therefore, the control of blood pressure, the use of a renin-angiotensin system blockade (RASB), and in selected patients, the use of corticosteroids (CS) is an important part of disease management. 4 Various treatments, aimed at improving the long-term renal outcome, have been applied in IgAN patients, including RASB, CS, immunosuppressive agents, antiplatelet agents, and tonsillectomy. However, to the best of the authors’ knowledge, there are no specific disease-targeted and standardized treatments for IgAN currently due to the insufficiency of clinical guidance. 5
A retrospective analysis including 1147 patients from the European Validation Study of the Oxford Classification of IgAN (VALIGA) cohort 6 for those with proteinuria ⩾3.0 g/d demonstrated that only 4% of the individuals with supportive RASB treatment reached a level of <1.0 g/d compared with 64% of those receiving CS, while for those patients with proteinuria ⩾1 to <3 g/d, the rate of patients reaching a level of <1.0 g/d were 63%, and 88% in those receiving RASB and CS, respectively. This finding supported that patients with IgAN demonstrated a good response to CS. A recent network meta-analysis 7 demonstrated that RASB + CS is probably the best therapeutic choice not only for reducing proteinuria but also for stabilizing renal function. A multicenter randomized control trial (RCT) 4 suggested that mycophenolate mofetil (MMF) + half-dose CS versus full-dose CS did not differ in reducing proteinuria. However, the findings regarding the benefit of MMF therapy in patients with IgAN have been contradictory. A meta-analysis demonstrated that MMF treatment did not have statistically significant effect on reducing proteinuria or protecting renal function in patients with IgAN. 8
The present cohort study was performed to evaluate the effectiveness and safety of half CS + RASB versus full CS in patients with IgAN.
Methods
Ethics committee statement
This study was approved by the Regional Ethics Committee of the Second Affiliated hospital of Nanchang University, and the approval number was No. [2011] 013. Due to the retrospective nature of the study, informed consent was not required. The design of the study fully took the safety and fairness principle into account. The research did not harm the subjects and protected the privacy right of the subjects. There was no conflict of interest in this research.
Patients
This study was a retrospective cohort study that was carried out in ‘real-world’ conditions via an observational design. We collected all kidney biopsy-confirmed IgAN patients between March 2011 and April 2017 in the Department of Nephrology, the Second Affiliated Hospital of Nanchang University, Jiangxi Province, China. Then, by analyzing their medical records, we screened out the standard–compliant patients. The inclusion criteria were: IgAN confirmed by renal biopsy, aged between 16 and 60 years old, 24 h urinary protein (UP) level >0.75 g, eGFR >30 ml/min per 1.73 m2, and a follow-up time of up to 18 months. The exclusion criteria were included: malignancy, diabetes mellitus, systemic lupus erythematosus, or any other systemic disease known to be associated with secondary IgAN, infections (including hepatitis B and C virus, and HIV), pregnancy or lactation; treatment with CS or immunosuppressive therapy within the 6-month period before enrollment; and life-threatening complications including heart failure or severe infection.
Treatment protocol
In China, most IgAN patients have serious concerns with the AEs associated with full-dose CS. For the IgAN patients who were concerned about the adverse reactions to full-dose CS, we conventionally use half CS ± RASB therapy to reduce the occurrence of AEs. Therefore, the treatment protocol (at the time of treatment) was based on a combination of patient preference and routine clinical practice at the hospital. Among all collected kidney biopsy-confirmed IgAN patients, one cohort (n = 89) included the standard–compliant patients who received half CS + RASB, and the second cohort (n = 73) included the standard–compliant patients who received full CS. In the half CS + RASB cohort, all patients were treated with RASB during the study, and the daily oral CS dosage was initiated at 0.4–0.6 mg/kg/d every morning for 2 months and then tapered by 20% each month for the next 4 months.
In the full CS group, the daily dosage of oral CS was initiated at 0.8–1.0 mg/kg/d taken every morning for 2 months and then tapered by 20% each month for the next 4 months. Subsequently, the dose was reduced slowly until it was withdrawn.
Follow-up and outcomes
Follow-up visits were scheduled at months 6 and 18 after the initiation of the immunosuppressive therapy described above. We predefined the potential baseline indexes, including sex, age, standard complete blood count, serum albumin level, 24 h UP level, serum creatinine (Scr) level, eGFR, total cholesterol level, and triglyceride level. In addition, the use of other immunosuppressive therapies, including azathioprine, cyclophosphamide or mycophenolate mofetil, was not allowed.
The primary outcomes included: time to complete remission (CR) defined as a 24 h UP level <0.4 g with a stable Scr level (defined as not >30% above the baseline) and the incidence of any AEs.
The secondary outcomes included: the rates of overall response [CR plus partial remission (PR)] at months 6 and 18, with PR defined as 0.4 g ⩽ 24 h UP < 0.75 g with a stable Scr level; relapse rates after stopping the treatments (relapse was defined as an overall response followed by proteinuria with protein excretion >0.75 g/24 h on two consecutive measurements); the change in the 24 h UP level at months 6 and 18 compared with baseline, and the incidence of a combined event (defined as eGFR decreased ⩾30%, ESRD or renal replacement therapy).
Statistical analysis
Normally distributed variables are presented as the mean ± standard deviation and were compared using an independent or paired t test, as appropriate. Nonparametric continuous variables are presented as the median with the interquartile range [(IQR) 25th and 75th percentile] and were compared using nonparametric tests, as appropriate. Categorical variables are summarized using proportions and were compared using the Pearson’s chi-square test. Time-to-event data are described using Kaplan–Meier curves, and the between–group difference was compared using the log-rank test. Repeated measures data were analyzed by the longitudinal data analysis method. At the same time, multivariable-adjusted Cox proportional hazards analysis was performed to assess the probability of CR. Statistical analysis was performed using Graph Pad Prism (version 7.0, San Diego, California, USA) and SPSS (version 23.0, Chicago, USA). Differences were considered statistically significant when the two-sided p value was <0.05.
Results
Study participants
A flow chart of the patient’s selection is shown in Figure 1. Preliminary screening enrolled 498 patients, and 162 subjects were finally included in this study. A total of 89 patients received half CS + RASB, and 73 patients with a similar risk profile with regard to progression received full CS. There were four censored patients among the standard–compliant patients who received half CS + RASB who were missing important data (24 h UP) during follow-up. Among the standard–compliant patients who received full CS, seven lacked important data (24 h UP level and medication administration record) during follow-up. These patients were excluded from the study. At baseline, patient characteristics were similar between the two cohorts (Table 1). The 24 h UP, serum albumin, Scr, total cholesterol, and serum triglyceride levels, eGFR, and histological information from the renal biopsy were comparable between the two groups. No patient included in the study had undergone a fundamental angiotensin converting enzyme inhibitors (ACEI) or angiotensin receptor blocker (ARB) treatment months preceding the start of follow-up. In the half CS + RASB group, five patients used calcium channel blockers (CCBs), and three patients used β-receptor antagonists to control their blood pressure. A total of eight patients used CCBs, and six patients used β-receptor antagonists in the full CS group. There was no significant difference in other antihypertensive drug use between the two groups.
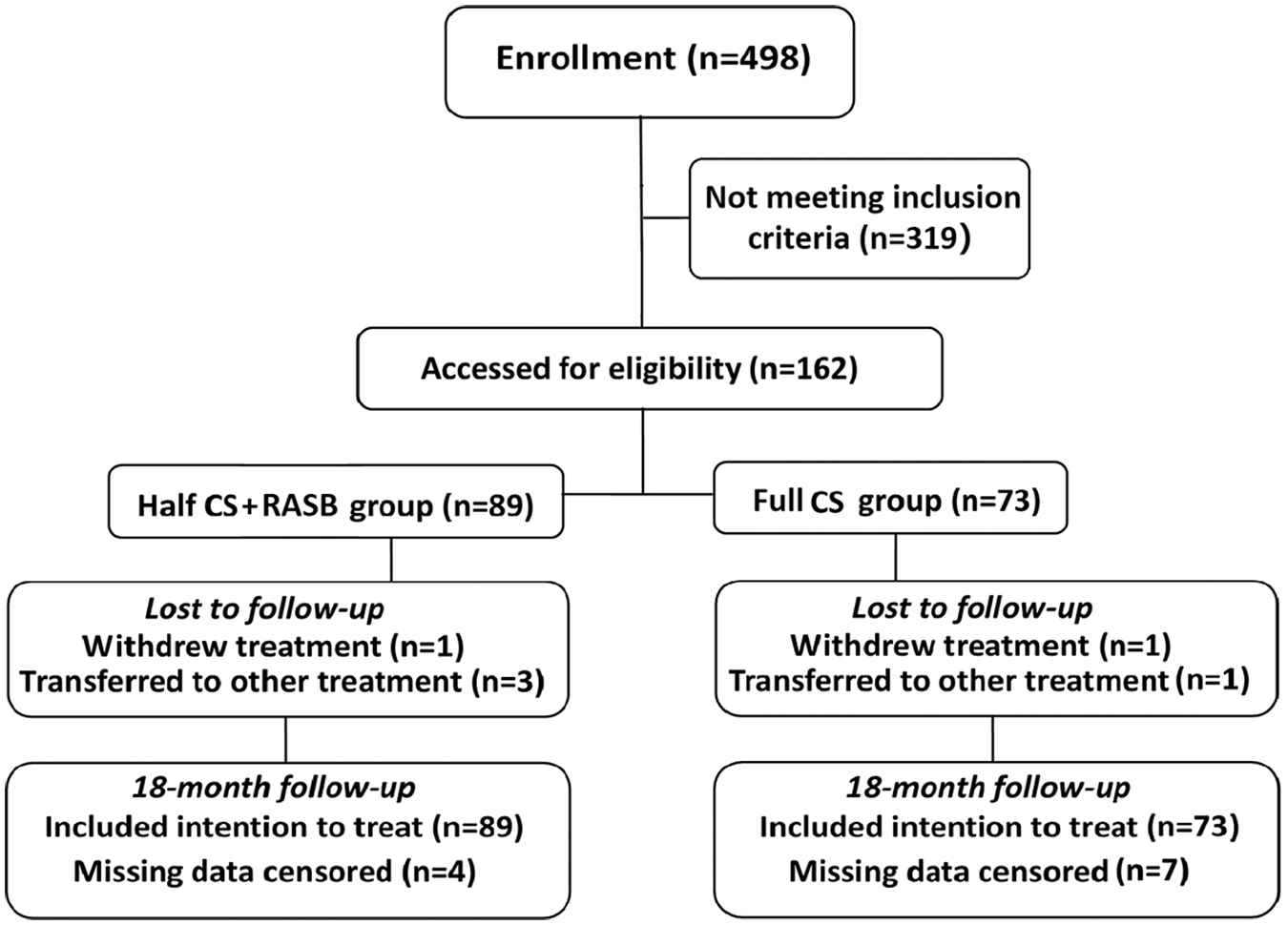
Flow diagram for inclusion of participants.
Clinical features of participants at baseline.

Note: Values for categorical variables were given as count (percentage); values for continuous variables, as mean ± standard deviation or median inter quartile range [IQR].
CCB, calcium channel blocker; CS, corticosteroid; eGFR, estimated glomerular filtration rate; IQR, interquartile range; RASB, renin-angiotensin system blockers.
Effectiveness
At 6-month follow-up, the CR rates were 38% (34/89) in the half CS + RASB group and 37% (27/73 patients) in the full CS group. There was no significant difference between the two groups (p = 0.87, Table 2). At the follow-up at 18 months, the CR rates were 59% (53/89) and 57% (42/ 73 patients) in the half CS + RASB and full CS groups (p = 0.88), respectively. The median times to CR were 6.6 and 5.8 months in the half CS + RASB and full CS groups, respectively. The Kaplan–Meier analysis for the probability of CR was not significantly different between the two groups (p = 0.92, Figure 2). We performed multivariable-adjusted Cox proportional hazards analysis for the probability of CR with SPSS (version 23.0) (p = 0.26, Figure 2). The outcome of the Cox proportional hazards analysis was similar to the outcome of the Kaplan–Meier analysis.
End points on the basis of the available patients at the end of the study phase.

CS, corticosteroid; ESRD, end-stage renal disease; RASB, renin-angiotensin system blockers. aLast-first available proteinuria; a negative value indicated a reduction in proteinuria over time.

Kaplan–Meier analysis (right) and multivariable-adjusted Cox proportional hazards analysis (left) for the probability of complete remission in patients with IgA nephropathy treated with full-dose versus half-dose corticosteroid plus renin-angiotensin system blockers.
The proportion of patients with overall remission in the half CS + RASB group and full CS group was 62% versus 56% at 6 months (p = 0.47) and 76% versus 73% at 18 months, respectively (p = 0.58). The relapse rates for this 18-month period were 2% (2/89) and 4% (3/73) in the half CS + RASB and full CS groups (p = 0.50), respectively.
Proteinuria decreased by a median of 1.39 g/d (IQR −2.22 to −0.4 g/d) and 1.44 g/d (IQR −2.07 to −0.54 g/d) at 6 months in the half CS + RASB and full CS groups, respectively (difference −0.5 g/d, p = 0.81, Table 2). At the follow-up at 18 months, proteinuria decreased by a median of 1.42 g/d (IQR −2.41 to −0.68 g/d) and 1.39 g/d (IQR −2.63 to −0.99 g/d) in the half CS + RASB and full CS groups, respectively (difference 0.3 g/d, p = 0.38, Table 2).
In the half CS + RASB group the eGFR of only one patient (1%) decreased >30% compared with the baseline. The eGFR of three patients (4%) decreased >30% in the full CS group. No patient developed ESRD or required renal replacement therapy in either group until the end of the study, and there was no significant differences in the cumulative incidence curves for the combined outcome (p = 0.22, Figure 3) between the two groups. This might be due to the short follow-up time.
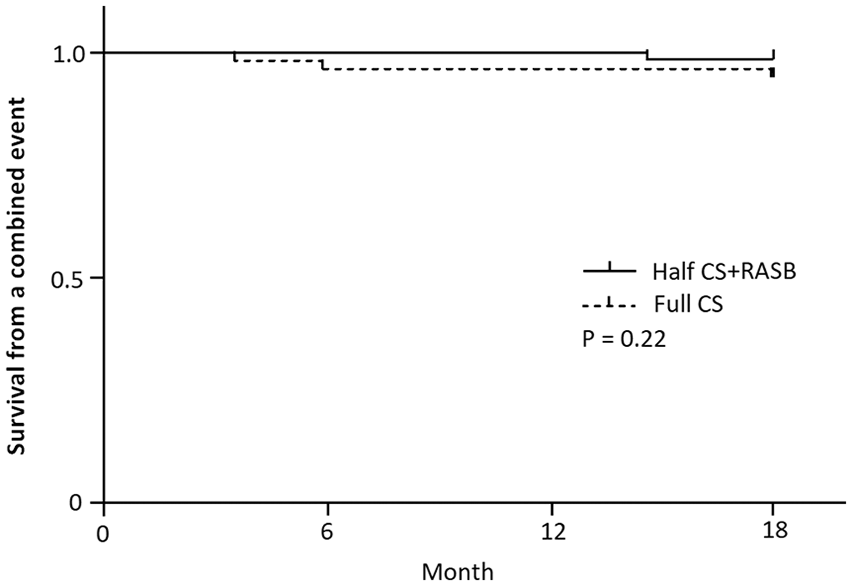
Cumulative incidence curves for the combined outcome in patients with IgA nephropathy treated with full-dose versus half-dose corticosteroid plus renin-angiotensin system blockers.
AEs
Over the 18 months of follow-up, 14 patients (16%) with at least one first AE were observed in the half CS + RASB group, and 26 patients (36%) were observed in the full CS group (p = 0.003, Table 3). Overall, the hazards of any first AEs considered separately were approximately two-fold lower in the half CS + RASB group than in the full CS group. Among these serious adverse events (SAEs), four patients in the full CS group suffered from pneumonia during the observation period. One single case of serious femoral head necrosis was observed in the full CS group, and no SAEs were observed in the half CS + RASB group. Among the AEs reported in the two groups, more than half of the events were related to infections. The incidence of infection [13% (12/89) versus 30% (22/73) p = 0.01] was significantly lower in the half CS + RASB group than in the full CS group. The incidence of new-onset diabetes mellitus, hepatotoxicity, and gastrointestinal symptoms accounted for a proportion of all AEs. This might be related to steroid exposure during the course of immunosuppression.
Summary of adverse events (AEs).
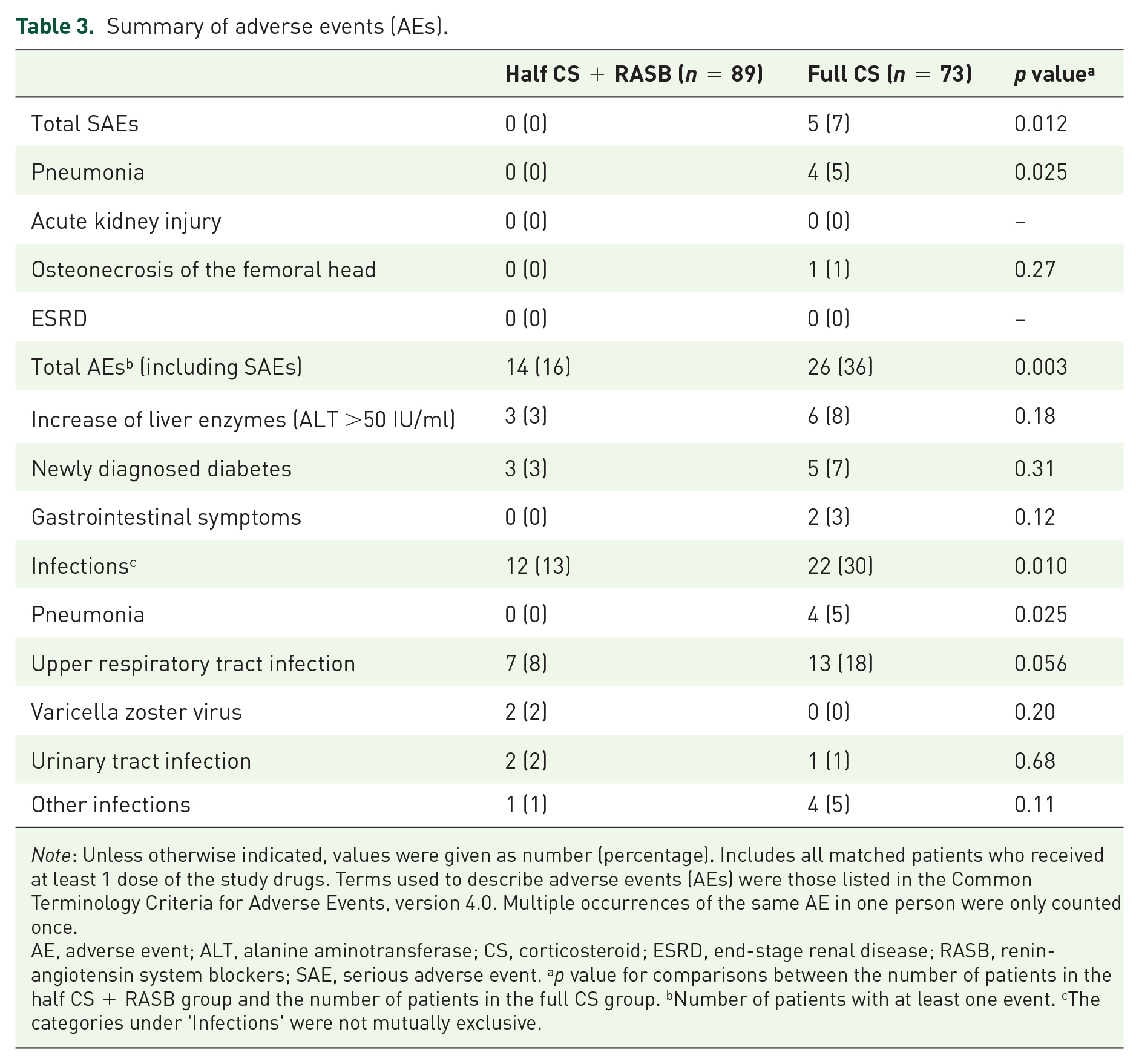
Note: Unless otherwise indicated, values were given as number (percentage). Includes all matched patients who received at least 1 dose of the study drugs. Terms used to describe adverse events (AEs) were those listed in the Common Terminology Criteria for Adverse Events, version 4.0. Multiple occurrences of the same AE in one person were only counted once.
AE, adverse event; ALT, alanine aminotransferase; CS, corticosteroid; ESRD, end-stage renal disease; RASB, renin-angiotensin system blockers; SAE, serious adverse event. ap value for comparisons between the number of patients in the half CS + RASB group and the number of patients in the full CS group. bNumber of patients with at least one event. cThe categories under ‘Infections’ were not mutually exclusive.
Discussion
As an autoimmune renal disease, IgAN has a variable clinical course ranging from proteinuria to rapidly progressive kidney failure and can result in a variety of histological lesions. Although the etiology and pathogenesis of IgAN remain unclear, IgA-dominant deposition in the mesangial area has been proposed as the critical factor in the onset of IgAN,9,10 which might promote the active and potentially reversible use of immunosuppressive treatment. 4 However, the benefit of immunosuppression therapy is controversial. The STOP-IgAN (Supportive versus Immunosuppressive Therapy for the Treatment of Progressive IgAN) trial 11 suggested that adding immunosuppression to intensive supportive care demonstrated no superiority in the improvement of clinical remission and in the development of ESRD and, in addition, increased AEs were observed. This conclusion might relate to the fact that histologic findings were not taken into consideration.
Several RCTs that have tested the efficacy of a CS regimen compared with a no CS control in IgAN found that full-dose CS resulted in better clinical outcomes in terms of remission and long-term outcomes.12–14 The network meta-analysis, 7 that included patients with IgAN with 24 h UP >0.75 g/d, demonstrated that RASB + CS was the most effective treatment to prevent ESRD or the doubling of Scr, was effective in reducing proteinuria, and strongly supported the efficacy and long-term renal protective value of RASB + CS treatment.
As an effective treatment for patients with IgAN, CS is associated with many SAEs, including inducing or aggravating infection, metabolism disorders, gastrointestinal symptoms, and neurological symptoms. Therefore, it is worth discussing the dose of CS. Hou and colleagues 4 proposed that among patients with proteinuria ⩾1.0 g/d, 48% of the individuals receiving half-dose CS+ MMF reached CR compared with 53% of those receiving full-dose CS (p > 0.05), and the group with half-dose CS had fewer AEs. These studies suggest the feasibility of half CS + RASB therapy.
We first compared the efficacy and safety of half CS + RASB with full CS in patients with IgAN. Patients with proteinuria ⩾0.75 g/d who received half CS + RASB and full CS were included. Both treatments had high CR rates (59% versus 57%) in our study. Although we observed no difference in the treatment outcomes between the two groups, the half CS + RASB group appeared to have some advantages over the full CS group. A total of four patients suffered from pneumonia, and one patient suffered from serious femoral head necrosis during the observation period in the full CS group, and no SAEs were observed in the half CS + RASB group. The hazards of any first infection considered separately were approximately two to three-fold lower in the half CS + RASB group than in the full CS group. In summary, the regimen of half CS + RASB provided a better option for patients with IgAN.
RASB + CS had lower risks for worse renal function and long-term renal protection. 7 In our study, the eGFR of only one patient decreased >30% compared with the baseline in the half CS + RASB group, while three patients were observed in the full CS group during the observation period. No patients progressed to ESRD or required renal replacement therapy. Although there was no significant difference between the two groups in the cumulative incidence curves, the incidence of these renal adverse outcomes was lower in the half CS + RASB group.
As for the limitations of the present study, missing data was inevitable. However, this would tend to bias the results toward the null hypothesis. Second, despite the use of a rigorous statistical methods, 15 there were no means to adjust for unmeasured variables.
Conclusion
There was no difference between half CS + RASB versus full CS in reducing proteinuria, but half CS + RASB resulted in fewer AEs and might be a better option for treating IgAN.
Footnotes
Acknowledgements
Li Wang performed the data collection, reviewed articles, and wrote the manuscript. Daijin Ren, Xin Liu, and Tianlun Huang completed the data analysis and provided the second views during the manuscript preparation. Gaosi Xu designed the study and revised the manuscript. All the authors read and approved the final version of the manuscript
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81970583/81560132), the Nature Science Foundation of Jiangxi Province (No. 20181BAB205016), and the “5511” Innovative Drivers for Talent Teams of Jiangxi Province (No. 20165BCB18018).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.