
Abstract
Background:
Pulmonary valve replacement is required for patients with right ventricular outflow tract (RVOT) dysfunction. Surgical and percutaneous pulmonary valve replacement are the treatment options. Percutaneous pulmonary valve implantation (PPVI) provides a less-invasive therapy for patients. The aim of this study was to evaluate the effectiveness and safety of PPVI and the optimal time for implantation.
Methods:
We searched PubMed, EMBASE, Clinical Trial, and Google Scholar databases covering the period until May 2018. The primary effectiveness endpoint was the mean RVOT gradient; the secondary endpoints were the pulmonary regurgitation fraction, left and right ventricular end-diastolic and systolic volume indexes, and left ventricular ejection fraction. The safety endpoints were the complication rates.
Results:
A total of 20 studies with 1246 participants enrolled were conducted. The RVOT gradient decreased significantly [weighted mean difference (WMD) = −19.63 mmHg; 95% confidence interval (CI): −21.15, −18.11; p < 0.001]. The right ventricular end-diastolic volume index (RVEDVi) was improved (WMD = −17.59 ml/m²; 95% CI: −20.93, −14.24; p < 0.001), but patients with a preoperative RVEDVi >140 ml/m² did not reach the normal size. Pulmonary regurgitation fraction (PRF) was notably decreased (WMD = −26.27%, 95% CI: −34.29, −18.25; p < 0.001). The procedure success rate was 99% (95% CI: 98–99), with a stent fracture rate of 5% (95% CI: 4–6), the pooled infective endocarditis rate was 2% (95% CI: 1–4), and the incidence of reintervention was 5% (95% CI: 4–6).
Conclusions:
In patients with RVOT dysfunction, PPVI can relieve right ventricular remodeling, improving hemodynamic and clinical outcomes.
Keywords
Introduction
The incidence of congenital heart disease (CHD) varies between 5 and 8 per 1000 live births.1,2 Approximately 20% of newborns with CHD have anomalies in the pulmonary valve or right ventricular outflow tract (RVOT), such as tetralogy of Fallot (TOF), truncus arteriosus, or pulmonary atresia. 3 For these patients, surgical repair of the RVOT is needed. Ultimately, however, these patients are subject to progressive RVOT dysfunction,4,5 which may take the form of pulmonary valve regurgitation (PR), pulmonary valve stenosis (PS), or both. Currently, surgical pulmonary valve replacement (SPVR) is considered the gold standard of treatment for PR and can be performed with a low mortality rate.6,7 However, valved conduits have a limited lifespan, often <10 years,8–12 thus necessitating an additional open-heart procedure.
In 2000, Dr Phillip Bonhoeffer performed the first percutaneous pulmonary valve implantation (PPVI) in a 12-year-old boy with stenosis and insufficiency of a prosthetic conduit from the right ventricle to the pulmonary artery. 13 Since then, the number of patients receiving PPVI has increased steadily because PPVI provides a nonsurgical and less invasive alternative for patients. To date, thousands of percutaneous pulmonary valve implantations have been performed worldwide 14 ; however, the timing of PPVI in patients with severe PR after TOF correction is still controversial. Until now, no meta-analysis has evaluated the effectiveness and safety of PPVI. Therefore, in this study, we aimed to evaluate the effectiveness and safety of PPVI in patients with RVOT dysfunction and to determine the optimal time for PPVI.
Methods
Study search and eligibility criteria
Two authors (L.Y.R. and W.W.W.), independently and in duplicate, searched the PubMed, EMBASE, Clinical Trial and Google Scholar databases for the period until May 2018. The terms used for the search were (‘transcatheter’ OR ‘percutaneous’) AND ‘pulmonary valve’ AND (‘implantation’ OR ‘replacement’), as well as ‘Melody valve’. The full electronic search strategy is presented in Supplementary File S1. We also manually checked reference lists of the identified reports and relevant reviews.
Studies meeting the following inclusion criteria were adapted: (1) Population: patients with RVOT dysfunction who received PPVI; (2) Intervention: PPVI; (3) Outcomes: changes in volume and function of both right and left ventricles, including valve function as assessed by echocardiography. Complications after PPVI were also estimated. Case reports were also considered. Reviews and studies including no recorded data were excluded. Publication language was not limited to English. To avoid overlapping information, when there were multiple studies from the same population, only one was included in each analysis.
Study selection
The selection procedure was performed in the following manner: (1) records were identified using a database; (2) duplicates were removed; (3) abstracts were screened and selected; (4) full-text articles were assessed for eligibility; and (5) finally, eligible studies were included.
The inclusion or exclusion criteria were unanimously selected; steps 1 to 3 were carried out by one reviewer, while step 4 was performed by two independent reviewers (L.Y.R. and W.W.W.). In cases of disagreement, a third reviewer (W.H. Shi) made the final decision.
Data extraction
The two independent reviewers reviewed the studies and extracted the following comparative data, which were also obtained for the pre- and post-replacement periods: RVOT gradient (mmHg); pulmonary regurgitation fraction (PRF; %); indexed right ventricular end-diastolic volume (RVEDV; ml/m²), indexed right ventricular end-systolic volume (RVESV; ml/m²), indexed left ventricular end-diastolic volume (LVEDV; ml/m²), indexed left ventricular end-systolic volume (LVESV; ml/m²), left ventricular ejection fraction (LVEF; %), and right ventricular ejection fraction (RVEF; %). Clinical outcomes [reintervention, infective endocarditis (IE), stent fracture, and procedure success] were also collected to evaluate procedure effectiveness and safety.
Methodological quality assessment
The Newcastle–Ottawa scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses 15 was used to assess the risk of bias from three aspects: selection, comparability, and outcome. All included studies were prospective or retrospective; therefore, we considered preimplantation patients to comprise a nonexposed cohort and post-implantation patients to comprise an exposed cohort to assess the risk of bias. Higher numbers of stars mean better quality; study quality was assessed as low (0–4 stars), moderate (5–6 stars), or high (7–9 stars).
Statistical analysis
Difference in means, 95% confidence interval (CI), and risk ratio were used to measure the outcomes. The p values were considered significant when p < 0.05. STATA software (version 12) was used to evaluate the outcomes. Heterogeneity was assessed based on the Cochrane Q-statistic and I² test (I² > 50 and p < 0.05 implying substantial heterogeneity). Across the studies, if no significant heterogeneity (defined as p > 0.10 or I2 < 50%) was found, the weighted mean differences (WMDs) were combined with the fixed-effects model (Mantel–Haenszel) 16 ; otherwise, the random effects model (DerSimonian–Laird) 17 was used. Moreover, a funnel plot was used to examine publication bias, and Begg and Mazumdar 18 and Egger’s tests 19 were used for statistical assessment. Linear regression was carried out to correlate the endpoint (e.g. RVOT changes) with the impact of independent variables (e.g. age at surgery, type of underlying disease).
Results
Study selection
A total of 4504 citations were identified, and 2095 duplicates were removed, leaving 2409 studies available for screening. After screening the abstracts, 408 studies were assessed as potentially relevant. After a full-text review, 388 studies were excluded primarily because they did not focus on the clinical outcomes or necessary data were unavailable; the remaining 20 studies were included.20–39 The study selection is shown in Figure 1.

Flow diagram of the study selection.
Study characteristics
Table 1 summarizes the main characteristics of these studies. A total of 1246 patients were enrolled, 1187 patients accepted PPVI for the treatment of RVOT dysfunction, and the sample sizes varied from 17 to 167. The mean age at PPVI ranged from 13.9 to 34 years old. A total of 574 (46%) patients were diagnosed with TOF. The mean follow up ranged from 1 to 55.2 months. Melody valve was utilized in 14 studies, Edwards Sapien was utilized in 3 studies, and both valve systems were chosen in 2 studies. In terms of study design, 16 studies were prospective (80%), and 11 (55%) were multicenter studies. Patient data from the United States (US) Investigational Device Exemption trial were included in three publications,22,31,39 and duplicated patients were observed in two publications.34,36 Among the included trials, the common primary indications for PPVI were PR and PS or both. All studies were judged to be of high quality with all scoring more than seven stars (Supplementary File S2), mainly due to the appropriate selection of participants.
Characteristics of the included studies.

MC, multicenter; NA, not available; P, prospective; PI, pulmonary insufficiency; PR, pulmonary regurgitation; PS, pulmonary stenosis; RP, retrospective; RVOT, right ventricular outflow tract; SC, single center; TOF, tetralogy of Fallot; US, United States.
Cardiac structure and function indices
RVOT
The mean differences of the Doppler RVOT gradient after PPVI in eight studies21,23,24,26,29–31,35 are shown in Figure 2(a). A significant reduction of RVOT gradient was observed in the patients after PPVI (WMD = −19.63 mmHg; 95% CI: −21.15, −18.11; p < 0.001). The fixed-effect model was used due to mild heterogeneity (I2 = 68.4%).

Forest plots of the clinical outcomes for the right side of the heart. Pooled differences in the means for (a) the mean Doppler RVOT, (b) the gradient of the indexed RVEDV.
RVEDV
Figure 2(b) shows the mean differences of indexed RVEDV after PPVI in 11 studies.20,22,24,25,28,29,32,35–37,40 A significant reduction was observed in the patients after PPVI (WMD = −17.59 ml/m²; 95% CI: −20.93, −14.24; p < 0.001). According to a subgroup analysis (Supplementary Figure S1), the RVEDV index was significantly lower in the PR group than in the PS group (−19.39; 95% CI: −29.52, −9.26; p < 0.001 versus −9.46; 95% CI: −17.02, −1.09; p = 0.014). After implantation, patients with preoperative index RVEDV > 140 ml/m² showed a greater reduction (−25.82 ml/m²; 95% CI: −41.64, −10.00; p < 0.001) than those with preoperative index RVEDV < 140 ml/m² (−16.55 ml/m²; 95% CI: −19.73, −13.37; p < 0.001; Supplementary Figure S2), but still higher than 100 ml/m².
RVESV
Figure 3(a) shows the mean difference of indexed RVESV after PPVI in seven studies.24,28,32,35–37,40 A significant reduction in indexed RVESV was observed in patients after PPVI (WMD = −11.10 ml/m²; 95% CI: −14.98, −7.22; p < 0.001). The fixed-effect model was used because there was no heterogeneity (I2 = 0).

Forest plots of the clinical outcomes for the (a) the indexed RVESV. Pooled differences in the means for (b) the PRF.
PRF
A total of 12 studies20–23,25,28,29,32,35,36,39,40 reported PRF. Figure 3(b) showed a significant reduction of PRF in the patients after PPVI (WMD = −26.27%; 95% CI: −34.29, −18.25; p < 0.001). The results showed severe heterogeneity: I2 = 98.40%. PRF decreased by 33.2% after PPVI (95% CI: −35.47, −30.93; p < 0.001) in the PR group. In the PS group, PRF decreased by 7.08% after PPVI (95%CI: −8.77, −5.39; p < 0.001). The results of the subgroup analysis are shown in Supplementary Figure S3. The regression analysis showed that PRF was corrected to diagnosis of TOF (p = 0.012), PRF decreased as TOF increased (Supplementary Figure S4).
LVEDV
Figure 4(a) shows the mean difference of indexed LVEDV after PPVI in eight studies.22,24,28,32,35–37,40 No heterogeneity was observed. Overall, a significant increase in the indexed LVEDV after PPVI was found (WMD = 7.13 ml/m²; 95% CI: 4.30, 9.96; p < 0.001).

Forest plots of the clinical outcomes for the (a) the indexed LVEDV, and (b) the indexed LVESV.
LVESV
Figure 4(b) shows the mean difference for indexed LVESV after PPVI in eight studies.20,24,28,32,35–37,40 However, no significant difference was observed in the patients after PPVI (WMD = 1.92 ml/m²; 95% CI: −0.05, 3.88; p = 0.056). No heterogeneity was found after pooling the data.
Ejection fraction
Figure 5(a) shows the mean difference of LVEF after PPVI in nine studies.20,24,28,32,35–37,40 A significant increase was observed in the patients after PPVI (WMD = 1.83%, 95% CI: 0.67, 3.00; p = 0.002) with no evidence of heterogeneity. RVEF [Figure 5(b)] showed a significant improvement in the PS group (WMD = 4.76%; 95% CI: 1.66, 7.85; p = 0.003), but no significant difference was found for the PR group (WMD = 1.09%; 95% CI: −3.01, 5.19; p = 0.603).
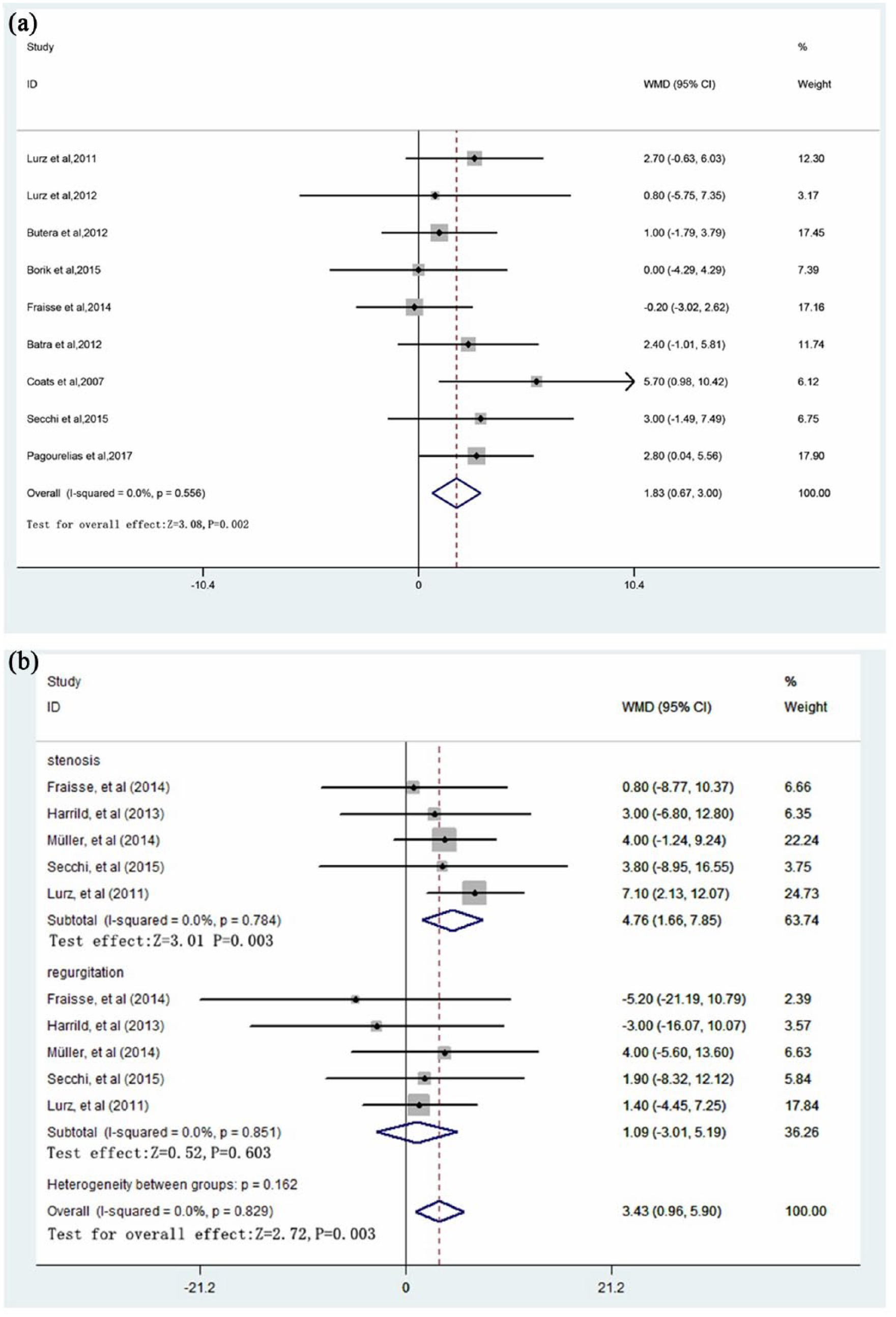
Forest plots of the clinical outcomes. Pooled differences in the means for (a) the LVEF and (b) the RVEF.
Procedure success and complications
Overall, 1003 of 1020 patients successfully underwent PPVI, and the pooled procedural success rate was 99% (95% CI: 98–99%). The mortality during the follow-up period was 2% (95% CI: 1–3%). Among 15 patients who died, 5 suffered sepsis/endocarditis, 2 were found to have arrhythmia, 1 was due to cardiac failure and 1 had compression of the left coronary artery. However, six patients died of causes unrelated to valve implantation. No patient died during the operation.
Table 2 shows the success rate and complications after the procedure. After PPVI, the most common complications were stent fractures during follow up, the pooled incidence of stent fracture was 5% (95% CI: 4–6%). Overall, the pooled incidence rate of IE was 2% (95% CI: 1–4%). In addition, the pooled incidence rate of reintervention in 12 studies was 5% (95% CI: 4–6%), and the surgical conversion rate was 1.2% (95% CI: 0.5–1.9%). Overall, three patients experienced coronary artery compression. Among them, one patient was performed, surgical conduit replacement, and another died due to severe compression. There were significant differences between various variables (except for endocarditis or bloodstream) and the date of publication (Supplementary File S3).
Pooled estimates for procedure success and complications.
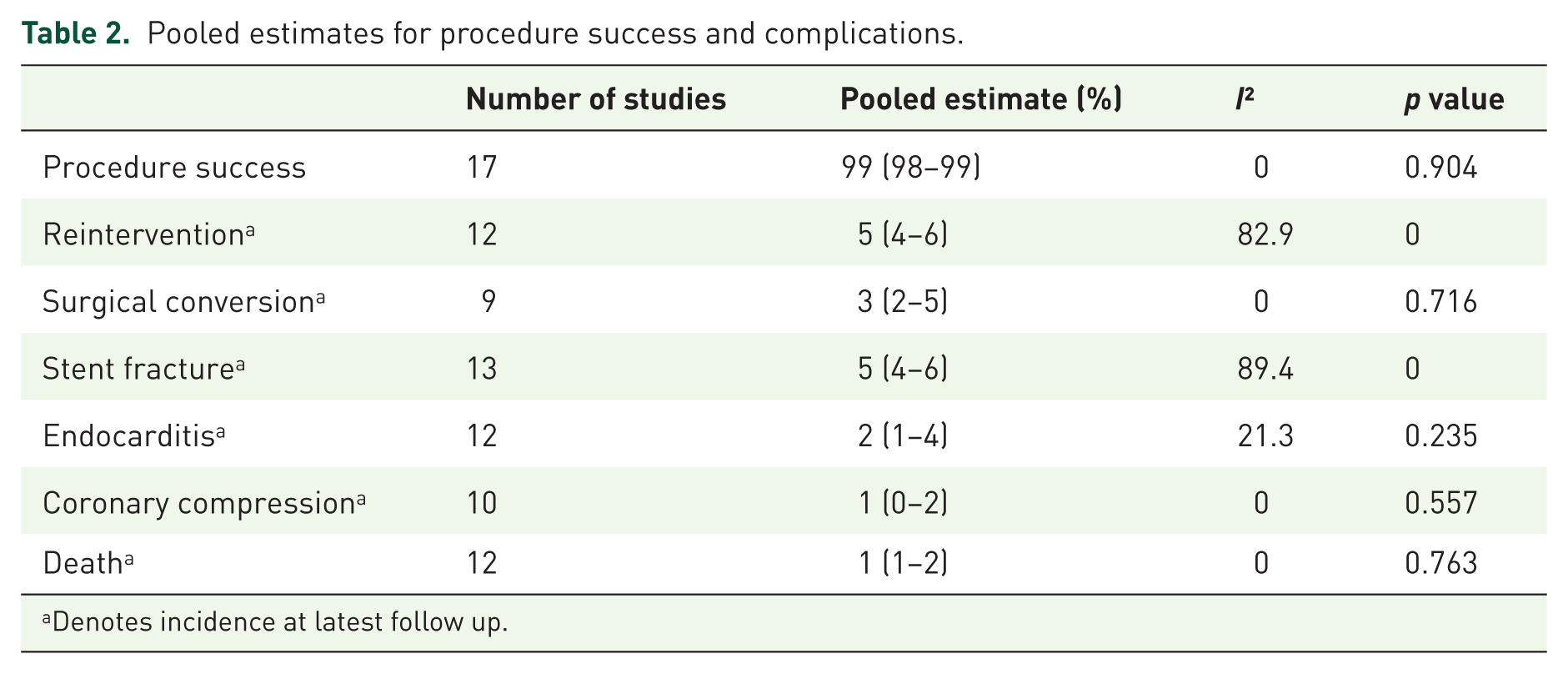
Denotes incidence at latest follow up.
Publication bias
Funnel plot analysis (Supplementary Figure S5A and S5B) revealed no potential publication bias among the included studies according to Begg’s rank correlation test and Egger’s linear regression test.
Discussion
The present study investigated the outcomes of PPVI in patients with RVOT dysfunction. The major findings are as follows: (1) the left and right ventricle structure were improved after PPVI, including ejection fraction; however, patients with a preoperative indexed RVEDVi > 140 ml/m² did not return to normal size; (2) RVOT gradient decreased; (3) PR decreased to normal; (4) stent fractures after PPVI were more likely to occur in patients with obstructed RVOT conduits, and IE was a threat to valve durability.
Previous study demonstrated that RVOT gradient is the only independent predictor of exercise capacity early after PPVI, 32 and significant RVOT obstruction reduces exercise capacity. The present study showed a significant reduction in RVOT gradient after PPVI. The exercise capacity was also improved.
In one study, 7–10 years after SPVR, the indexed RVEDV was significantly increased, and the value returned to 84% of the pre-SPVR volume. 41 This might be mainly because the preoperative indexed RVEDV of the patients was 200 ± 43 ml/m². A previous study found that patients with a preoperative indexed RVEDV >170 ml/m² did not show ‘normalized’ RV volumes after implantation. 42 The American College of Cardiology/American Heart Association guidelines (2014) recommend that in the absence of symptoms, magnetic resonance imaging criteria for severe pulmonary insufficiency include the following: indexed RVEDV > 150 ml/m²; PRF > 40%; and RV ejection fraction < 40%. 43 In the present study, four studies recruited patients with preoperative indexed RVEDV > 140 ml/m²; after valve implantation, the patients failed to return to the normal level (100 ml/m²). Early valve implantation is associated with more favorable RV reverse remodeling.28,37 Therefore, to prevent symptoms and RV damage becoming more apparent, we suggest PPVI to be performed before the RVEDV index reaches 140 ml/m².
PRF decreased to normal levels in all patients despite the severity of preimplantation pulmonary regurgitation, but the long-term function remains to be further evaluated. RVEDV decreased more in the PR group than in the PS group. However, no change was observed in RVEF among the PR patients. Further study needs to investigate whether PPVI could improve RVEF and the underlying mechanisms.
In the included studies, a significant increase in LVEDV was seen after PPVI. However, no change was found in LVESV. Left heart systolic function improved due to increased LVEF and LVEDV. The increase in LVEDV after PPVI may reflect late remodeling as a response to the noticeable improvement in filling over time. 35 It is worth noting that almost all included patients with RVEF > 40% and LVEF > 50%. Therefore, the results may not represent the actual effect for patients with poor ejection function.
Pre-stenting with a bare metal stent before PPVI provides a good solution for stent fracture, and it was frequently observed in studies with lower rates of pre-stenting prior to PPVI. 44 Nordmeyer and colleagues reported that patients presented a 65% reduction in the risk of stent fracture when a bare metal stent was implanted. 45
IE of the valve is a potential threat to long-term heart function46–48 and may result in valve explantation.21,34 This complication necessitates a repeat of PPVI and can result in sepsis-related mortality. 46 IE is an acute adverse event. Therefore, minimization of the infection rate is important. Antibiotic prophylaxis and adequate dental hygiene are recommended to prevent infectious events.27,46 Other severe complications including valve migration or embolization,23,27 pulmonary artery occlusion or rupture, 45 and coronary artery compression 49 are reportedly rare.
In addition, a previous study found shorter hospitalization and lower complication rates in patients who received PPVI compared with surgical replacement. 50 Therefore, PPVI seems to be a well-tolerated therapy for patients.
Some limitations of this meta-analysis should be noted. Firstly, all included studies were nonrandomized observational studies. Secondly, different studies had different follow-up periods. Long-term outcomes remain unclear. Thirdly, all publications reported data for both PR and PS. However, only five studies were available to perform a subgroup analysis in which outcomes were extracted separately from these two subgroups.
Few randomized controlled trials comparing PPVI with surgery have been published; thus, the meta-analysis was limited to perform the head-to-head comparison; however, PPVI has been found to be an effective treatment for patients with RVOT dysfunction. Thus, further long-term follow-up studies with large sample sizes are needed to evaluate the clinical outcomes of PPVI in patients with RVOT dysfunction.
Conclusions
In the present study, PPVI was found to improve RV and LV function in patients with RVOT dysfunction. PRF and RVOT gradient were decreased significantly, the complications after the procedure were within an acceptable range. Therefore, PPVI is considered an effective and well-tolerated treatment for patients with RVOT dysfunction.² This conclusion should be considered carefully and confirmed based on further, randomized, large-scale studies.
Supplemental Material
Supplementary_Figure_S1 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_Figure_S1 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_Figure_S2 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_Figure_S2 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_Figure_S3 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_Figure_S3 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_Figure_S4 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_Figure_S4 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_Figure_S5A – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_Figure_S5A for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_File_S1 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_File_S1 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_File_S2 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_File_S2 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Supplemental Material
Supplementary_File_S3 – Supplemental material for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis
Supplemental material, Supplementary_File_S3 for Percutaneous pulmonary valve implantation in patients with right ventricular outflow tract dysfunction: a systematic review and meta-analysis by Liyu Ran, Wuwan Wang, Francesco Secchi, Yajie Xiang, Wenhai Shi and Wei Huang in Therapeutic Advances in Chronic Disease
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant numbers 81170188 and 30971212), the Natural Science Foundation of Chongqing (grant number CSCT2009BB5069), and Chongqing Municipal Health and Family Planning Commission (grant numbers 2016HBRC001 and 2016XMSB0003767).
Conflict of interest statement
The author(s) declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.