
Abstract
Barrett’s esophagus is the precursor lesion for esophageal adenocarcinoma. Screening and surveillance of Barrett’s esophagus are undertaken with the goal of earlier detection and lowering the mortality from esophageal adenocarcinoma. The widely used technique is standard esophagogastroduodenoscopy with biopsies per the Seattle protocol for screening and surveillance of Barrett’s esophagus. Surveillance intervals vary depending on the degree of dysplasia with endoscopic eradication therapy confined to patients with Barrett’s esophagus and confirmed dysplasia. In this review, we present various novel techniques for screening of Barrett’s esophagus such as unsedated transnasal endoscopy, cytosponge with trefoil factor-3, balloon cytology, esophageal capsule endoscopy, liquid biopsy, electronic nose, and oral microbiome. In addition, advanced imaging techniques such as narrow band imaging, dye-based chromoendoscopy, confocal laser endomicroscopy, volumetric laser endomicroscopy, and wide-area transepithelial sampling with computer-assisted three-dimensional analysis developed for better detection of dysplasia are also reviewed.
Keywords
Introduction
Barrett’s esophagus (BE) is a well-established premalignant stage of esophageal adenocarcinoma (EAC) and is defined as an extension of salmon-colored mucosa into the tubular esophagus extending ⩾1 cm proximal to the gastroesophageal junction (GEJ) with biopsy confirmation of intestinal metaplasia (IM). 1 The incidence of EAC in patients with BE is 0.3–0.6% per patient-year. 1 The estimated prevalence of BE in the general population is 1–2%.2,3 As most patients with BE are asymptomatic, these rates likely underestimate the true prevalence of the disease. Esophagogastroduodenoscopy (EGD) with biopsy is the gold standard for the diagnosis and surveillance of BE. As there is an increasing incidence of EAC in the Western world, efforts focusing on the screening and surveillance of BE are of paramount importance. In this review, we examine the current strategies for the screening and surveillance of BE and recent advances in the field.
Screening
Should we screen for BE? Pros and cons
The rationale for screening for BE is early identification of patients who are at increased risk of developing EAC and timely intervention with the goal of decreasing mortality. Despite a lack of randomized controlled trials (RCTs), indirect evidence suggests that screening leads to detection of EAC at earlier stages, better outcomes and increase in 5-year survival rates from 17% to 74%. 4
The current screening strategies are inadequate as more than 90% of patients diagnosed with EAC do not have a prior diagnosis of BE and over 40% of patients with EAC do not have prior gastroesophageal reflux disease (GERD) symptoms. 5 It must be noted that even if all patients with chronic GERD are screened, a huge number of patients with BE (probably more than two-thirds) will remain undiagnosed because many among them do not have chronic GERD. Better targeting of the candidates for BE screening is necessary in order for a screening strategy to be useful. Sedated EGD (sEGD) cannot be used for large-scale screening of general population as it is expensive and has a very low yield owing to the small absolute risk of EAC in GERD patients. In addition, some studies with a long-term follow-up show no difference in survival.6,7 To address these limitations and to improve efficiency, novel techniques have been described but are yet to prove their ability to replace sEGD.
Who should we screen?
Guidelines of major societies recommend against screening of the general population and instead recommend screening patients with multiple risk factors for BE1,8–13 (Table 1). Chronic GERD is the most common risk factor for BE [odds ratio (OR) of 2.9; 95% confidence interval (CI) 1.86–4.54, p = 0.0001] and has a stronger association for long segment BE (OR 4.92; 95% CI 2.01–12.0; p = 0.30). 14
Screening guidelines for Barrett’s esophagus * .

All guidelines recommend that biopsy is taken using Seattle protocol (four quadrant biopsy every 2 cm or every 1 cm in cases of known/suspected dysplasia).
ACG, American College of Gastroenterology; AGA, American Gastroenterological Association; ASGE, American Society for Gastrointestinal Endoscopy; BE, Barrett’s esophagus; BSG, British Society of Gastroenterology; EAC, esophageal adenocarcinoma; EGD, esophagogastroduodenoscopy; ESGE, European Society of Gastrointestinal Endoscopy; GERD, gastroesophageal reflux disease; PPI, proton pump inhibitor.
Other risk factors for BE include male gender, increasing age, white race, central obesity, cigarette smoking, and family history of BE/EAC. Studies have shown that BE is twice as likely in men than women with the ratio increasing to 4:1 in patients younger than 50. 15 Men develop BE about 20 years earlier than women. 15 BE is usually diagnosed in sixth to seventh decade of life with a steep increase in prevalence from 2.1% in third decade to 9.3% in sixth decade and plateau thereafter. 16 In a large study of 280,075 procedures, white subjects were most likely to have suspected BE (5.0% in white, 2.9% in Hispanic, 1.8% in Asian/Pacific islander, 1.5% in black; p < 0.0001). 17 Waist circumference is also an independent risk factor for BE after adjustment for other risk factors (for every 5 cm increase, OR 1.14; 95% CI 1.03–1.27, p = 0.02). 18 This association persists even after adjustment for body mass index (BMI) and GERD symptoms. 19 Having ever-smoked is also associated with an increased risk of BE compared with non-GERD controls (OR 1.44; 95% CI 1.20–1.74) and population-based controls (OR 1.42; 95% CI 1.15–1.76). 20 Family history of BE has been identified as another potential risk factor for BE. BE is more common in first- or second- degree relatives of patients with BE compared to controls (24% versus 5%, p < 0.005) and the presence of family history of BE/EAC was strongly associated with BE (OR 12, 95% CI 3.3–44.8). 21 Even though these factors increase the relative risk of BE, the absolute risk of EAC remains low. In a prospective cohort of 355,034 subjects, a scoring system was developed using age, sex, smoking, body mass index, and history of esophageal conditions or treatments. The five-year risk of EAC was 0.16% for individuals with scores above the threshold and 0.02% for individuals with scores below the threshold. 22
How to screen?
Careful visual inspection during EGD and four quadrant biopsies at every 1–2 cm interval using Seattle protocol and biopsy of any mucosal irregularities in salmon-colored mucosa above the GEJ is the gold standard method for BE screening. 23 Standard brush cytology for detection of BE was also evaluated. Cytology has high diagnostic accuracy for high-grade dysplasia (HGD)/EAC (sensitivity 90%), moderate sensitivity for BE (60% versus 92%) and low sensitivity for low-grade dysplasia (LGD) (20% versus 97%) compared with histology. 24 The addition of brush cytology complements histology and increases cost without improvement in diagnostic yield. 25
Standard sEGD is expensive and associated with a small risk of complications such as cardiopulmonary events, aspiration, bleeding, perforation, and indirect patient-related costs. Therefore, sEGD is not an ideal tool for screening of large populations and there exists a need for alternative, cheap, widely available, and an accurate method of screening.26,27 Several modalities were developed and the current evidence is presented in the following.
Unsedated transnasal endoscopy (uTNE) is performed with an ultrathin endoscope using topical anesthesia obviating the need for sedation. Compared with sEGD, the sensitivity of uTNE for detection of columnar lined esophagus was 98% and of IM was 91% and specificity was 100%. 28 Procedure time ranged from 3.7 ± 1.8 min to 5.5 ± 1.7 min and the mean recovery time was quicker in uTNE compared with sEGD (18.5 versus 67.3 min; p < 0.001).29–31
When compared with sEGD, uTNE was safer with fewer procedure- and sedation-related complications and high acceptability with willingness to undergo repeat procedure in up to 93.2%.32,33 Minor complications (2.8%) included minimal choking, gagging, anxiety, nasal pain, sore throat, and minor epistaxis.28,29,34 No serious adverse events were reported.29,30,34 In a RCT, differences in mean costs for sEGD versus hospital-based uTNE was US$1386.72 (95% CI 1291.79–1486.07). 35 In addition, endoscopes with disposable sheaths such as EndoSheath® technology (Vision-Sciences Inc., Orangeburg, New York) reduce cost by eliminating need for disinfection and nonphysician providers can be trained to perform the procedure. Better acceptance and affordability allow consideration for uTNE as a screening test for BE for patients seen in the office. 29
Cytosponge is a mesh surrounded by gelatin capsule attached to a string passed transorally. 36 Five minutes after swallowing, the capsule dissolves in the proximal stomach, expanding the mesh to a sphere of 3 cm. The sample containing cytological specimen is stained with Trefoil Factor3 (TFF3) which is a biomarker for IM.
Three large-scale trials were undertaken to utilize cytosponge and TFF3 to develop an improved screening method for BE.36–38 In a prospective study of 504 patients with a prescription for acid suppressants, cytosponge with TFF3 had a sensitivity of 73.3% (95% CI 44.9–92.2%) and specificity of 93.8% (95% CI 91.3–95.8%) for detecting BE ⩾1 cm of circumferential length. 37 In a case-control study of 1110 GERD patients with or without BE comparing cytosponge and TFF3 with sEGD, sensitivity was 79.9% which increased to 89.7% when the device was swallowed twice and specificity was 92.4%. 36 BE Trial 3 (BEST3) is in the process of determining its efficacy and cost-effectiveness in primary care. 38 A cost-effectiveness analysis with cytosponge using microsimulation models calibrated for US Surveillance, Epidemiology, and End Results Program (SEER) data on EAC incidence and mortality was determined. 39 Screening GERD patients with cytosponge and following up positive results with EGD for confirmation reduced cost by 27–29% when compared with screening by EGD alone. In addition to TFF3, cytosponge sample can be used for detection of other additional biomarkers for BE such as TFPI2, TWIST1, ZNF345, and ZNF569, which can further improve the sensitivity. 40
A qualitative study showed high acceptability and comfort level in patients undergoing cytosponge procedure. 41 Visual analog scale determined favorable acceptability (p < 0.001) in 93.9–99% patients.36,37 Brief episodes of sore throat and site abrasion with oozing blood was noted in 16.7% of patients, which resolved without any intervention. 36 Cytosponge with TFF3 appears promising over endoscopy and can be utilized in the primary care clinic if applicable to the general population. Ongoing large-scale studies will guide further decisions.
A similar technology called a sponge on string device (EsophaCap, Capnostics, Doylestown PA) has been evaluated in pilot studies where it was swallowed and withdrawn in 98% of subjects and provided abundant DNA yield for the evaluation of BE markers. 42
In an earlier study, a prototype nonendoscopic balloon with spikes on the surface was passed transorally in patients with BE presenting for surveillance sEGD. Balloon cytology was positive in 52 of 63 (83%) patients with BE, in 6 of 8 patients with EAC, 2 of 2 patients with HGD, and 2 of 8 patients with LGD. 43 Balloon cytology was six-fold cheaper than sEGD, but only 49% of patients found it more tolerable. Recently, a swallowable nonendoscopic encapsulated balloon device with textured surface was developed. 44 In 86 patients who swallowed nonendscopic balloon, a biomarker panel consisting of CCNA1 DNA methylation and VIM DNA methylation detected BE metaplasia with 90.3% sensitivity and 91.7% specificity. As a nonendoscopic screening technique, the balloon sampling device was well tolerated and efficient. 44
Esophageal capsule endoscopy (ECE) is a noninvasive unsedated imaging technique that allows visualization of the esophagus using wireless or tethered cameras without obtaining a biopsy. In a meta-analysis of nine studies including 618 patients, the pooled sensitivity and specificity for diagnosis of BE were moderate, 77% and 86%, respectively. 45 ECE is safe and 80% preferred ECE to sEGD; however, it was not more cost-effective than sEGD (Table 2).46,47
Screening techniques.

From manufacturer.
A liquid biopsy utilizes a blood sample for detection of circulating microRNAs (miRNAs) in the blood, which are dysregulated and expressed in tissue-specific patterns in cancer. In a recent study of 41 patients with BE and 15 controls, a panel of 4 circulating miRNAs (miRNA-95-3p, -136-5p, -194-5p, and -451a) distinguished BE from controls with sensitivity and specificity of 78% and 86%, respectively. 48 In a recent meta-analysis, increased expression of miR-192, -194, and -215 and decreased expression of miR-203 and -205 was found in BE tissue when compared with normal controls. 49 However, assays with sufficient sensitivity and specificity need to be developed before these markers can be recommended for clinical use.
Exhaled volatile organic compounds (VOC) are products of metabolism which can be detected in the breath by ‘electronic nose’ devices and which may be altered in different disease states. In a recent study of 66 patients with BE compared with 56 patients without BE, the electronic nose distinguished the two groups with 82% sensitivity, 80% specificity, and 81% accuracy with an area under receiver operating characteristic curve (AUROC) of 0.79. 50 A study on 81 patients with EAC versus gastric cancer versus no controls identified 12 VOCs of which 8 were significant predictors for EAC compared with normal subjects. The AUROC to detect EAC from normal controls was 0.97. 51 As these are noninvasive tests, the patient acceptance rate is very high but needs to be validated in larger studies.
Oral microbiome is another area of research as dysregulation and alteration of the microbiome have been reported in several diseases. There appears to be a higher risk of EAC with Tannerella forsythia and Lactobacillus fermentum, and lower risk with fewer number of genus Neisseria and species Streptococcus pneumoniae.52,53 The efficiency of cytosponge as a sampling tool in retrieving microbiome DNA when compared with endoscopic methods found >10 times increased quantity (p < 0.0001). 54 However, the diagnostic accuracy and application for the general population, feasibility, and cost-effectiveness are yet to be determined.
Surveillance
Currently, surveillance involves early detection of dysplasia by high-definition white light endoscopy (WLE) with random four-quadrant biopsies every 2 cm (or every 1 cm if dysplasia is known or suspected) followed by biopsy of mucosal irregularity (nodules, ulcers, or visible lesions). Shared medical decision involving risks, benefits, limitations, and importance of adherence to periodic endoscopies along with the possibility of endoscopic therapy or surgery needs to be discussed with patient before enrolling in surveillance. The risk of EAC in BE depends on the degree of dysplasia. The annual risk of EAC with nondysplastic BE (NDBE) is estimated to be 0.33%, 0.54% in LGD, and 7% in HGD. 1 It should be noted that confirmed LGD by expert pathologists have higher rates of progression than those downstaged. In one study, the risk of HGD/EAC with LGD confirmed by expert pathologists was 9.1% per patient-year whereas for those downstaged to NDBE or indefinite for dysplasia, it was 0.6% and 0.9% per patient-year respectively. 54 Other factors known to be associated with neoplastic progression of BE are age (OR 1.47, 95% CI 1.01–1.05), male sex (OR 2.16, 95% CI 1.84–2.53), smoking (OR 1.47, 95% CI 1.09–1.98), and length of BE segment (OR 1.25, 95% CI 1.16–1.36). 55 How-ever, all societies recommend surveillance intervals taking into consideration the degree of dysplasia only (Table 3).1,8–13
Surveillance guidelines for BE * .
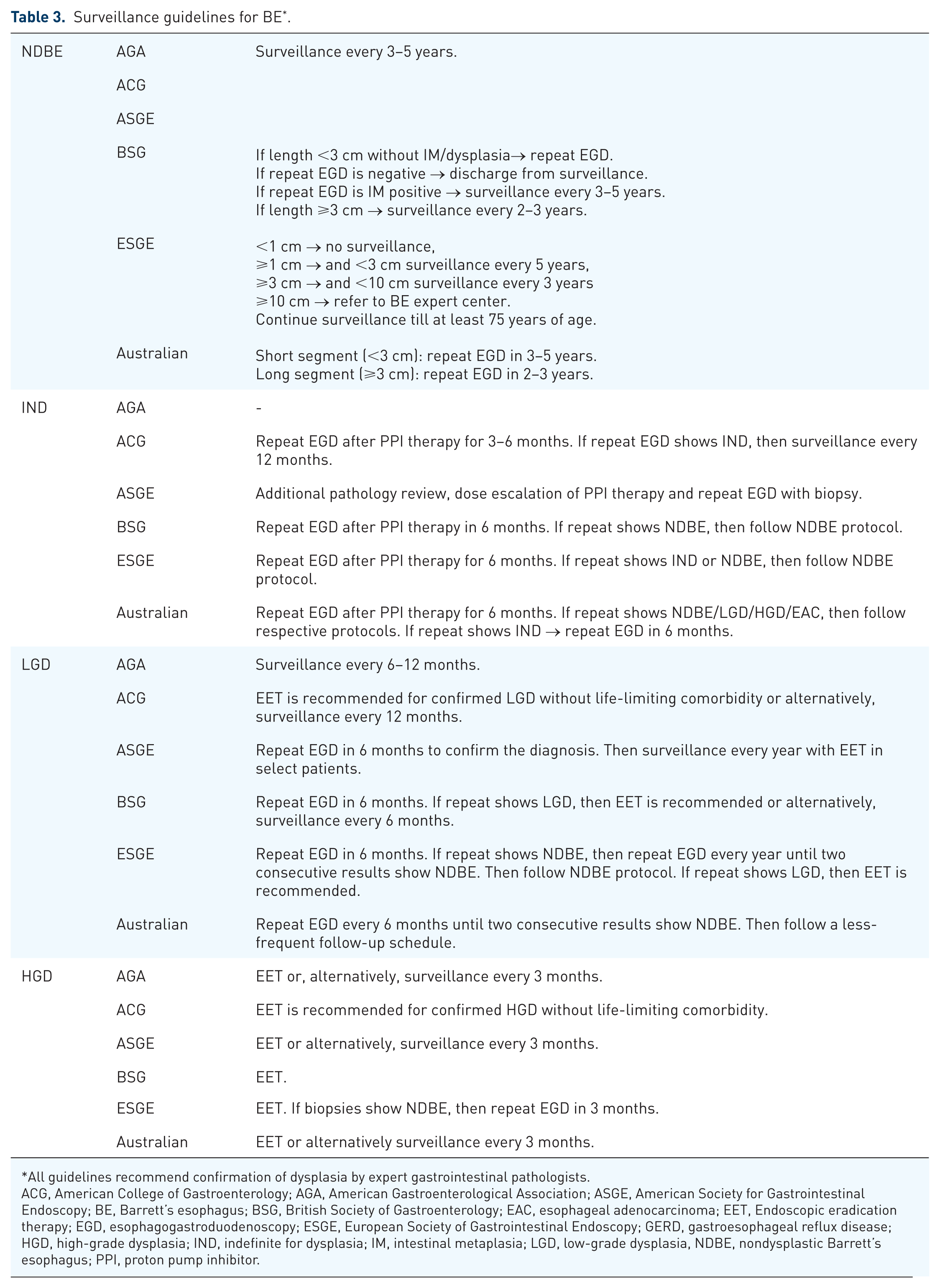
All guidelines recommend confirmation of dysplasia by expert gastrointestinal pathologists.
ACG, American College of Gastroenterology; AGA, American Gastroenterological Association; ASGE, American Society for Gastrointestinal Endoscopy; BE, Barrett’s esophagus; BSG, British Society of Gastroenterology; EAC, esophageal adenocarcinoma; EET, Endoscopic eradication therapy; EGD, esophagogastroduodenoscopy; ESGE, European Society of Gastrointestinal Endoscopy; GERD, gastroesophageal reflux disease; HGD, high-grade dysplasia; IND, indefinite for dysplasia; IM, intestinal metaplasia; LGD, low-grade dysplasia, NDBE, nondysplastic Barrett’s esophagus; PPI, proton pump inhibitor.
Studies show a survival advantage in patients with BE undergoing surveillance endoscopy. In a cohort study of about 30,000 patients with BE followed for over 5 years, patients diagnosed with EAC during surveillance, were detected at an earlier stage (stage 0 to 1: 74.7% versus 56.2; p < 0.001), survived longer (median 3.2 versus 2.3 years; p < 0.001), and had lower cancer-related mortality (34.0% versus 54.0%, p < 0.0001) compared with those not in surveillance. 59 Despite these advantages of earlier detection of EAC with surveillance, the current approach is invasive, time-consuming with concerns of lead and length time bias affecting the improvement in mortality.60,61 The natural course of progression in BE is unknown, and when compared with other cancers, EAC is relatively rare. 62 The cost–benefit analysis calculated per life-year gained compared with other cancer programs is expensive, and the overall survival of patients appears similar to age and gender-matched individuals. 63
Therefore, various advanced imaging technologies have been proposed to maximize efficiency and diagnostic yield of the current surveillance model. In a meta-analysis on 843 patients, advanced imaging techniques increased diagnostic yield of dysplasia/EAC by 34% (95% CI 0.13–0.56; p = 0.0001) when compared with WLE with random four-quadrant biopsy. 64 Whereas ASGE endorses the use of advanced imaging, AGA, ACG, BSG do not recommend routine use. 9 Most of the currently available techniques rely on the ability of endoscopist to detect the abnormalities.
ASGE released criteria for the preservation and incorporation of valuable endoscopic innovations (PIVI) for advanced imaging techniques. An imaging technique can replace random four-quadrant biopsy if their per-patient sensitivity is ⩾90%, specificity is ⩾80%, and negative predictive value (NPV) is ⩾98% for detecting HGD/EAC. The techniques evaluated for PIVI included chromoendoscopy by using acetic acid and methylene blue, narrow-band imaging (NBI), and confocal laser endomicroscopy (CLE). Targeted biopsies with acetic acid chromoendoscopy, NBI, and endoscope-based CLE meet these thresholds. 65
Dye-based chromoendoscopy utilizes chemicals such as methylene blue, indigo carmine, and acetic acid to provide wide-field imaging and mucosal enhancement during endoscopy. 65 Methylene blue and indigo carmine do not meet ASGE PIVI standards, and mixed reports in studies prevent routine use. A meta-analysis on acetic acid chromoendoscopy found high diagnostic accuracy for HGD/EAC (sensitivity 92% and specificity 96%). 66 Chromoendoscopy is simple, inexpensive, and improves detection rates. However, there is high interobserver variability owing to a lack of classification, unequal distribution of dye over the mucosa, and increased procedure time making this technique uncommon.65,67,68
Virtual chromoendoscopy involves advanced imaging of surface patterns without the use of dyes. NBI, available on Olympus endoscopes, allows real-time wide-field imaging using narrow wavelength range of light (filtering white into blue and green) in identifying early neoplastic lesions from irregular mucosal and subsurface vascular patterns. 65 Recognition of the mucosal and vascular patterns guides imaging targeted biopsies leading to fewer total biopsies and reduced cost of surveillance. 69 Barrett’s International NBI Group (BING) developed NBI classification to be more user-friendly than earlier classifications and has a good inter-observer agreement (κ = 0.681). 70 A meta-analysis showed pooled sensitivity, specificity, and NPV of 94.2%, 94.4%, and 97.5%, respectively. 71 Similar virtual chromoendoscopy techniques include I-Scan (Pentax), flexible spectral imaging color enhancement (FICE, Fujinon), and blue light imaging (Fujinon), which accentuate specific areas by wavelength and improve the detection of dysplasia in BE. 72
CLE allows in vivo histological assessment by 1000 times magnification using an integrated endoscope or probe insertion to obtain confocal images after exogenous fluorescein administration. Probe-based CLE has high specificity for detecting dysplasia and cancer (98%), low sensitivity (67%), and substantial inter-observer agreement (κ = 0.6) and aids in real-time therapeutic decision making. 58 Endoscope-based CLE is no longer in use despite meeting ASGE PIVI standards (pooled sensitivity, specificity, and NPV of 90.4%, 92.7%, and 98.3%, respectively). 71 CLE is expensive, 73 requires a correlation between imaging and histology, administration of intravenous fluorescein which increases sampling error from extravasation of fluorescein and near-field imaging. Probe-based CLE can be used to image only limited areas and cannot be used to image the entire esophagus. 73
Volumetric laser endomicroscopy (VLE) is an optical frequency domain imaging technique that provides high-resolution real-time cross-sectional images using a 3.7 mm probe located within the balloon that helically scans 360° circumference of esophageal surface up to 3 mm in depth. 65 A total length of 6cm is scanned starting 1 cm distal to the GEJ and moving proximally from distal end of the balloon. 65 The sizes of currently available balloons are 14, 17, and 20 mm. 74 VLE is sensitive in identifying mucosal lesions that are invisible under standard WLE, thus allowing targeted biopsy of dysplastic/cancerous lesions. 75 The novel VLE laser marking system further enables direct in vivo marking of suspicious areas for targeted biopsy. 76 Imaging features of VLE found to be independently predictive of BE neoplasia included lack of layering, higher surface than subsurface signaling, and irregularly dilated glands/ducts. Recently, a software upgrade called Intelligent Real-time Image Segmentation™ (IRIS) artificial intelligence has become available, which displays the three most common esophageal image features and colorizes the image to aid review. Sensitivity and specificity of VLE for dysplasia detection are 86% and 88%, respectively, and diagnostic accuracy is 87%. 77 A recent study reported incremental yield of dysplasia with laser marked targets in VLE (33.7%) when compared with random biopsies (5.7%), Seattle protocol biopsies (19.6%), and VLE without laser marking (24.8%). 78 The rate of overall yield of dysplasia compared to Seattle protocol was statistically higher (OR 2.1; p = 0.03). Another study demonstrated very high inter-observer agreement overall (esophageal mucosa, gastric mucosa, nonneoplastic BE, and neoplastic BE; κ = 0.81) and strong agreement for nonneoplastic BE and neoplastic BE (κ = 0.66 and 0.79, respectively). 79 The learning curve for VLE users after a brief training session of 31 novice clinicians showed that 71% were able to achieve interpretation competency during 96-slide review and half of the physicians achieved competency at 65 images. The median accuracy overall was 95%, 90% for nonneoplastic BE, and 96% for neoplastic BE. 80 VLE provides a large field of view and is fast requiring only 60–90 seconds for a complete scan. 65 Minor mucosal lacerations were reported in 2% of patients with the 25 mm balloon and hence it was discontinued. 81 An upcoming development is computer-aided detection of early Barrett’s neoplasia using an algorithm for automated analysis of ex vivo VLE images where a full scan including 1200 frames is analyzed in less than a minute. 82 This technology had a considerably high detection rate when compared with manual reads (AUROC 0.95 versus 0.81, respectively) thereby demonstrating a future potential to assist endoscopists in the early detection of neoplasia with VLE.
Wide area transepithelial sampling with computer-assisted three-dimensional analysis (WATS3D) uses esophageal brush biopsy that procures wide-area, full-thickness transepithelial tissue sample. In the laboratory, computer-assisted analysis synthesizes up to 100 two-dimensional optical slides into a single three-dimensional image for pathology review. Multicenter randomized trials or double-blinded crossover studies have been underway since 2010 evaluating the efficiency of WATS3D in the diagnosis of BE/dysplasia as an adjunctive to the Seattle protocol biopsies.83–86 A study on 160 patients with BE, using WATS3D in conjunction with biopsy yielded an additional 23 cases (14.4%; 95% CI 7.5–21.2%) of HGD/EAC compared with biopsy alone. 87 The inter-observer agreement among pathologists in the diagnosis of dysplasia using WATS3D was very high with a κ = 0.95 for HGD/EAC and κ = 0.74 for LGD and indefinite for dysplasia (IND). 88 The main advantage of this technique lies in large tissue sample size although it adds an additional 4.5 min to procedure time. 87 Even though glandular changes are better detected by WATS3D than with cytology, architectural changes cannot be detected as in histology and this leads to overestimation of dysplasia by WATS3D. 89 Furthermore WATS3D has been studied as an adjunctive to random biopsy without a direct comparison with surveillance biopsies per Seattle protocol. Only WATS-positive HGD/EAC slides were reviewed by two expert pathologists instead of all cases as only latter can give an idea of false-negative and false-positive rates. Studies on larger patient cohorts with longer follow up are needed before WATS3D is generalizable to community population.
Role of artificial intelligence
On the horizon is the use of artificial intelligence which will allow auto-analysis of medical images to detect dysplastic lesions within BE (computer-aided detection). Several studies have been performed in past the few years using WLE, high-definition WLE, and NBI images to automatically detect areas of abnormality within BE segment. These studies are based on use of mainly support vector machines and neural networks with other techniques such as k-nearest neighbors (k-NN), k-statistics, and decision trees. 90 The main limitations of the currently proposed techniques are the limited number of images these studies are based on, inordinate amount of time needed to process the images, and, finally, the accuracy.
Post-ablation surveillance
Endoscopic eradication therapy (EET) of BE is highly effective with eradication rates of up to 78% for metaplasia and 91% per dysplasia, but with recurrence rates of 4.8/100 person-years for IM and 2/100 person-years for dysplasia.91,92 Therefore, close surveillance is recommended after successful eradication of BE. ACG recommends surveillance every 3 months for the first year following complete eradication of intestinal metaplasia (CEIM), every 6 months in the second year, and annually thereafter for patients with HGD or IMC. 1 In patients with LGD before ablation, endoscopic surveillance is recommended every 6 months in the first year following CEIM and annually thereafter. 1 A recently published model based on US RFA registry and UK national Halo registry recommends surveillance at 1 and 3 years after CEIM for LGD and 0.25, 0.5, and 1 year for HGD or IMC. 56 Discontinuing surveillance is not recommended after multiple negative examinations as recurrences have been reported several years after EET. Another concern is the presence of subsquamous BE (buried BE) developing beneath the endoscopically normal appearing post-ablative epithelium, which cannot be adequately sampled by biopsy forceps. The clinical significance of subsquamous BE is not known but likely carries a low risk of progression as subsquamous EAC is infrequent. 67
In conclusion, although there are clear-cut guidelines on the screening and surveillance of BE, the current strategies are inadequate as more than 90% of patients diagnosed with EAC do not have a prior diagnosis of BE. The alternative nonendoscopic methods of screening that are in development may make screening available to the wider population while reducing the costs. Based on current evidence, uTNE is suitable for mass screening for BE. Cytosponge and Esocheck nonendoscopic balloon are being validated in larger studies before they can be implemented for clinical use. For better detection of dysplasia during surveillance, NBI is useful for recognition of subtle lesions as it is fast, easy to use, and accurate. VLE and WATS3D are commercially available and have high dysplasia detection rates and have potential for future use. Further studies are needed to evaluate their efficacy in decreasing EAC mortality rates and also to develop better biomarker panels for risk stratification of BE patients.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.