
Abstract
Haemorrhoids are common, affecting up to one quarter of all adults according to some estimates. Numerous interventions exist for their management, ranging from topical and medical therapies to outpatient treatments and surgical interventions that aim to fix or excise. Given the polysymptomatic nature of the disease, it is difficult to effectively judge which treatment option is best. Recently introduced novel haemorrhoid management techniques, such as stapled haemorrhoidopexy, Ligasure™ excision and haemorrhoidal artery ligation, aim to reduce harm whilst maintaining or improving on outcome. These new techniques are universally more expensive, and available good quality data suggest the additional cost does not necessarily equate to universally better outcomes compared with traditional older interventions, such as rubber band ligation and excisional haemorrhoidectomy. Whatever the intervention selected for treatment, it is clear that this should be tailored to the individual based on patient choice, convenience and degree of haemorrhoids.
Keywords
Introduction
Haemorrhoids represent pathological changes in the anal cushions, a normal component of the anal canal involved in aiding evacuation of stool and fine-tuning of anal continence. These pathological changes include rupture of the supporting connective tissue within the cushions, resulting in enlargement of the vascular plexus. The pathogenesis of haemorrhoids explains the symptoms associated with the condition: bleeding, swelling and prolapse, seepage due to the disruption of the fine tuning of continence and consequent irritation of the perianal skin. More severe symptoms may include thrombosis leading to pain.
Haemorrhoids are very common, affecting as many as 1 in 4 of the population and resulting in a significant community and hospital practice burden. Over 20,000 haemorrhoidal procedures are carried out in the UK each year. 1
Treatment options for haemorrhoids are varied; however, the evidence base for many of these options has, until recently, been poor. Despite the poor scientific substantiation, some of these treatment options have stood the clinical test of time. However, many new options have been introduced since the turn of the century. There is recent scientific support for some of these newer options that allow an evidence-based update to management.
The aim of this article is to present this evidence for both the traditional and newer interventions and provide the reader with an algorithm for the modern treatment of the disease.
Conservative management
Given haemorrhoids are such a common condition, first-line therapy should be prevention and minimally interventional therapy particularly in the community setting. Diet and lifestyle undoubtedly play an important role in haemorrhoid management. Fibre has traditionally been thought to both prevent and treat haemorrhoidal symptoms. Evidence for benefit comes from a meta-analysis of seven clinical trials which showed that fibre supplement relieved symptoms and minimized risk of bleeding by approximately 50% 2 but with no effect on prolapse. Further advice to increase oral fluids, exercise regularly, avoid straining and constipation-inducing medications makes logical sense but there is unfortunately little evidence.
Drug therapy
A vast industry has evolved around preparatory creams and suppositories for treating haemorrhoids. These combinations of steroids, anaesthetics, antiseptics and barrier creams may be effective in temporarily relieving the acute symptoms of haemorrhoidal disease. Patients often return to these agents if symptoms recur, not realizing that symptoms fluctuate with time and may have resolved with simple hygiene alone.
Unlike for these over-the-counter remedies, there is some evidence for effectiveness of venotonic therapies. Oral flavonoid medication can control acute bleeding. 3 They increase vascular tone, reduce venous capacity, decrease capillary permeability, facilitate lymphatic drainage and have anti-inflammatory effects. A large meta-analysis showed that venotonics have significant beneficial effects on bleeding, pruritus, discharge and overall symptom improvement. 4
Outpatient interventions
Rubber band ligation
Various outpatient treatments for symptomatic haemorrhoids exist. In the UK and many other countries, rubber band ligation (RBL) is the most commonly performed of these therapies. 5 RBL uses a device that allows a rubber band to be applied to each haemorrhoid via a proctoscope. This band constricts the blood supply causing the haemorrhoid to become ischaemic before being sloughed approximately 1–2 weeks later. The resultant fibrosis reduces any element of haemorrhoidal prolapse that may have been present. Although easy to perform, and with a short learning curve, care has to be taken to place the bands correctly to reduce the potential for severe pain.
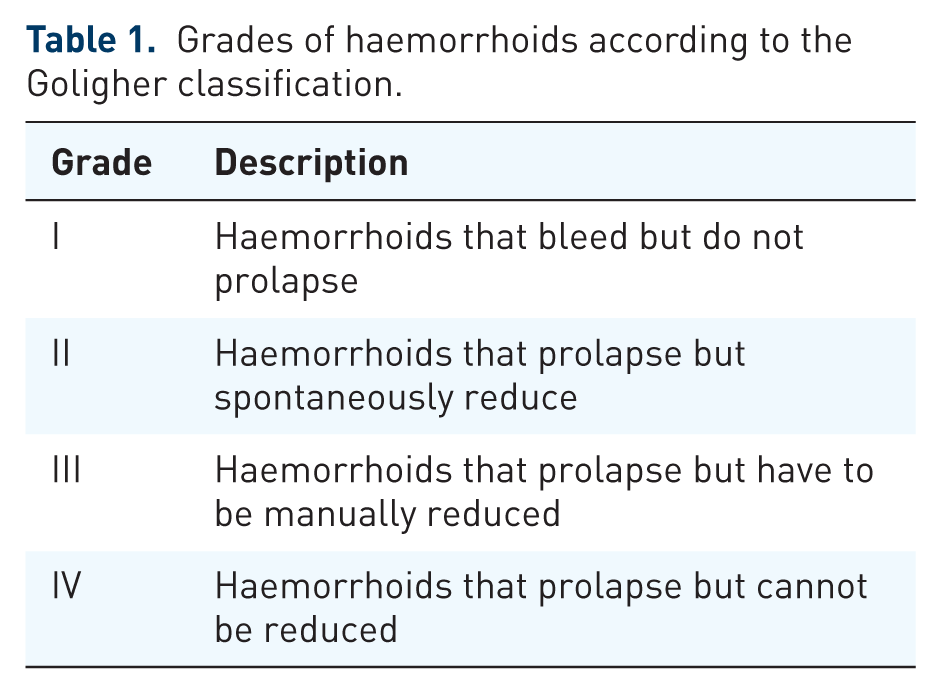
The literature concerning efficacy and safety of RBL is substantial. 6 Reported recurrence rates are broad (from 11% to over 50%). This variability reflects the poor definition of recurrence, the grade of haemorrhoids (see Table 1), the number of treatment episodes and the length of follow up. In most studies, recurrence is >30% and is more likely with increasing prolapse. Recurrences can be treated by re-banding or by surgical intervention.
Grades of haemorrhoids according to the Goligher classification.
Immediate pain is common, although it often only lasts a few hours after the procedure. In 1% of patients undergoing RBL, pain is severe enough to warrant admission. 7 Other complications include bleeding and vaso-vagal symptoms. Rarely the bleeding is severe enough to require admission and blood transfusion. There have been reports of severe pelvic sepsis with a few instances leading to death. 6
The procedure meets several criteria for the optimum outpatient therapy. It is certainly cheap, quick and easy to carry out. It also seems to be very safe in the majority of people. Efficacy may not be as high as some operative interventions but improves with repeat procedures. 8 The common symptom of short-lived pain may be reduced with local anaesthetic injection. 9
Injection sclerotherapy
Various sclerosant solutions have been used for injecting piles. The comparative efficacy of these solutions is unclear. Less potent solutions such as 5% phenol in almond oil are more commonly used and probably have a lower risk of mucosal necrosis. Injection treatment is simple, safe and rapid, but probably not as effective as RBL. 10 This treatment modality should probably be reserved for patients where bleeding is the main symptom and conservative therapy has not improved the symptoms (and other causes having been excluded). Other indications possibly include patients with a high risk of secondary haemorrhage (patients on anticoagulants and patients with advanced cirrhosis) and those who are immunocompromized.11,12
Complications include bleeding (either immediate or secondary), pain (which can be localized or rarely liver pain due to porto-systemic injection), or prostatic symptoms if the injection is placed too deeply. Injection of the prostate can result in urinary retention (often resolving spontaneously), epididymitis, prostatitis (presenting as pain in ejaculation and haemospermia) and even prostatic abscess. 10
Infrared coagulation
Infrared coagulation consists of a direct application of infrared waves to the haemorrhoidal pedicle resulting in necrosis and sloughing of the pile. Several applications are required per haemorrhoid but each takes a few seconds. Complications and efficacy are similar to RBL with some suggesting less pain presumably related to the lower volume of tissue necrosis.13–16 Although a potential alternative to RBL, the equipment is expensive and there is a longer learning curve.
Other therapies
Bipolar, direct current and radiofrequency ablation therapy
Application of low wattage bipolar diathermy results in tissue coagulation. The process takes up to 30 s and multiple applications to the same site are often required. 17 Complications, including pain, bleeding and fissuring, occur in around 10% of patients.
Direct current therapy has gained recent favour in the form of Ultroid therapy, although the reasons for its popularity, other than aggressive marketing, are unclear. The procedure involves application of a probe onto the haemorrhoidal cushion and application of a low direct current for around 10 min per haemorrhoid. Results are at best equivalent to injection sclerotherapy 18 and RBL, but with the procedure taking significantly longer.
Radiofrequency ablation cuts and coagulates haemorrhoidal tissue using less power (and hence less temperature) than other electrical equipment. A comparison with RBL suggested similar efficacy to RBL with less pain. 19 Again equipment is expensive and the procedure has not gained universal acceptance.
Combination therapy
Numerous combinations of therapies have been described and include RBL with injection sclerotherapy 20 or infrared coagulation. 21 Again, the studies are of poor quality. Indeed, the description of some therapies involves almost daily outpatient visits over a few weeks. Such an intense therapy negates the advantage of an outpatient procedure, particularly as efficacy is not clear. With this caveat, the combination of RBL with injection sclerotherapy does make practical sense. Not only is the double therapy a ‘belt and braces’ approach but also the bolus of sclerosant below the band ligation may act to secure the band, reducing failure due to premature slippage.
Surgical therapy
Haemorrhoidectomy
Surgical excision of haemorrhoids is perhaps one of the oldest operations ever performed. Although there are numerous variations of the technique two essential operations exist; open excision (Milligan–Morgan) and closed haemorrhoidectomy (Ferguson). For the open technique, the skin-covered external element of the haemorrhoid is excised together with the mucosal element with ligation to the haemorrhoidal pedicle, taking care to preserve the intervening mucosal bridges. Ferguson haemorrhoidectomy also removes the vascular haemorrhoidal tissue but preserves the anoderm, theoretically limiting post-operative discharge and accelerating the healing process.
More recent ‘advances’ in the open technique have involved different technologies to excise the haemorrhoid including diathermy, lasers and ultrasonic dissectors. A variation of the Ferguson technique involves the Ligasure™ (Medtronic Minn, USA) coagulator which is postulated to seal the tissue with minimal thermal spread resulting in less post-operative pain.
All of these techniques have potential complications, including pain, bleeding, urinary retention, infection, iatrogenic fissuring, stenosis and incontinence. Manouvres to reduce all of these complications have been described. Metronidazole theoretically reduces pain by reducing the potential for micro-abscess formation. A total of five trials including more than 350 patients have shown that either oral or topical metronidazole reduces post-operative pain after open haemorrhoidectomy.22–26 Commencing laxatives prior to operation seems appropriate to prevent post-operative constipation but has been shown to be of direct benefit in one small low quality trial. 27
Procedure for prolapsed haemorrhoids
The procedure for prolapsed haemorrhoids, or stapled haemorrhoidopexy, utilizes a circular stapling device to excise a doughnut of mucosa immediately above the haemorrhoidal complex. In doing so the procedure not only disrupts the blood supply to the plexus, reducing engorgement, but also pulls any redundant mucosa into the anal canal reducing any prolapse. As there is no incision in the sensitive anal mucosa, theoretically pain is reduced and recovery enhanced; indeed, good evidence supports this idea.28–30
Some complications such as bleeding, discomfort and urinary retention are similar to other haemorrhoidal operations. However, there are some more unique potential complications that may be serious. These include rectovaginal fistulae, rectal perforation and retroperitoneal sepsis. A unique syndrome of pain, urgency and tenesmus has been described and may respond to topical nifedipine.31–32
Haemorrhoidal artery ligation
A recent intervention that has gained in popularity is haemorrhoidal artery ligation (HAL). This utilizes a modified proctoscope, which incorporates a Doppler probe. The device allows accurate detection of the haemorrhoidal arteries feeding the anal cushions. Targeted ligation of the vessels reduces haemorrhoidal engorgement whilst at the same time allowing fixation of the cushion reducing the potential for prolapse. The suture may be modified to incorporate a ‘pexy’ suture and enhance reduction of any existing prolapse. The procedure is simple and easy to learn. As there is no surgical wound and the sutures are applied above the dentate line, pain is theoretically reduced and recovery enhanced. Significant literature has suggested this is the case. Pain tends to be moderate and recedes in the first few days after surgery such that there is minimal to no pain by 1–3 weeks. 6 Complications include (usually mild) bleeding, urinary retention, thrombosis and fissure formation. 33
Which is surgery most effective and causes the least harm?
The question of which surgical therapy is most effective is the crux to any summary of management. The question is not easy to answer. Haemorrhoidal disease is a multisymptomatic condition and as such it is difficult to define cure or recurrence. For instance, one intervention may stop bleeding in one patient, but leave an element of prolapse. If the patient is not bothered by the prolapse, is he or she ‘cured’? Severity of haemorrhoidal disease and duration of follow up will also influence the estimate of efficacy. The literature is generally poor in defining all of these parameters. These drawbacks combined with the multiple interventions and variations of interventions that are reported make any pooled meta-analysis extremely difficult. Nevertheless, there have been attempts to define which procedure is best with a general consensus that treatment probably needs to be tailored to the individual depending on symptoms, grade of haemorrhoids and patient expectation.34,35
A total of two meta-analyses have been published regarding outpatient treatment of grade I and II haemorrhoids, both in the 1990s.36,37 Infrared coagulation is stated in one as the outpatient treatment of choice, whereas the other, more extensive article concludes that RBL is the most efficacious, although this review does note the association with more pain than the other options.
A more recent network meta-analysis has examined the interventions for grade III and IV haemorrhoids. This analysis compared 12 variations of potential interventions and included an analysis of 98 papers. 38
In terms of harm they found the following: open, closed and radiofrequency haemorrhoidectomies resulted in an increased likelihood of complications compared with HAL, Ligasure™ and ultrasonic techniques. HAL resulted in less bleeding potential than open and stapled haemorrhoidopexy and resulted in fewer urgent reoperations than open, closed, stapled and Ligasure™ procedures. Open and closed haemorrhoidectomies were more painful in the first 24 h than stapled, HAL, Ligasure™ and ultrasonic techniques.
In terms of recovery, normal activities were resumed earlier in the stapled, Ligasure™ and ultrasonic groups than the open and closed haemorrhoidectomies.
In terms of recurrence this was more common after stapled haemorrhoidectomy and HAL than after open, closed and Ligasure™ haemorrhoidectomy.
None of these meta-analyses have included the most recent series of randomized controlled trials (RCTs) on haemorrhoidal disease. The first was a comparison of RBL with HAL for grade II or early grade III haemorrhoids. 39 In this trial, recurrence was very carefully defined using a simple patient reported outcome backed up by hospital records. HAL was found to be more effective than RBL at 1 year. However, HAL was as effective as ‘a course’ of RBL (1 or 2 sessions of banding). All other parameters were the same except cost. HAL was significantly more expensive.
A second high-quality RCT compared stapled haemorrhoidopexy with conventional haemorrhoidectomy for grade II–IV haemorrhoids. 40 In agreement with many trials, stapled haemorrhoidopexy was found to be less painful than conventional haemorrhoidectomy in the short term and complication rates were similar. However, quality of life was significantly better in the conventional group over the 2-year follow up, and the cost of the stapled haemorrhoidectomy procedure was significantly greater.
A third trial compared HAL with stapled haemorrhoidopexy 41 and found that although the HAL resulted in less pain, the procedure took longer, was more expensive and probably resulted in a higher recurrence rate.
The general conclusion of the most recent series of large high quality RCTs appears to be that the newer techniques for haemorrhoidal treatment are not delivering improved efficacy compared with the more traditional procedures despite the increased cost.
Proposed algorithm of care
With the three most recent trials, there is probably enough data to produce an up-to-date network meta-analysis to define the best treatment for all degrees of haemorrhoidal disease. This would require complex statistical confirmation but it is possible to try to predict what such an analysis would show.
There is no doubt that tailoring of treatment to at least to the grade of haemorrhoids should be a priority. Conservative management in the form of diet and lifestyle should be introduced to all patients, and may reduce symptoms to a satisfactory level in those with grade 1 haemorrhoids. Flavonoids may also be helpful. For those where symptoms persist, and those with grade II haemorrhoids, a course of RBL appears to be the most effective therapy. Failure of treatment may justify surgical intervention, with the least invasive procedure being HAL. For grade III and IV haemorrhoids, the most effective therapy appears to be conventional haemorrhoidectomy with the method of haemorrhoidectomy being unclear other than scissor or diathermy excision being the most cost effective. If open haemorrhoidectomy is carried out there is reasonable evidence for the use of metronidazole postoperatively. Stapled haemorrhoidopexy should not be completely dismissed as an option. It should probably be used for those cases of circumferential prolapse where an excisional haemorrhoidectomy technique that preserves adequate mucosal bridges is difficult.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The author declares that there is no conflict of interest.