
Abstract
Dementia is a common and debilitating syndrome with enormous impact on individuals and societies. Preventing disease onset or progression would translate to public health and societal benefits. In this review, we discuss the latest evidence on interventions that may show promise for the prevention of cognitive decline. We appraise existing evidence primarily drawn from randomized controlled trials, systematic reviews, and meta-analyses, but also highlight observational studies in humans and relevant work in model organisms. Overall, there is currently limited evidence to support a cause–effect relationship between any preventive strategy and the development or progression of dementia. However, studies to date suggest that a multifactorial intervention comprising regular exercise and healthy diet, along with the amelioration of vascular risk factors, psychosocial stress, and major depressive episodes may be most promising for the prevention of cognitive decline. We discuss the challenges, future directions, and implications of this line of research.
Keywords
Introduction
Dementia encompasses a wide range of neuropsychiatric and medical conditions characterized by cognitive deficits that interfere with daily life. The most common form of dementia is Alzheimer disease (AD), which accounts for approximately two thirds of all cases. 1 The remaining cases result from a number of conditions with diverse etiologies. 2 Importantly, the pathological brain processes that underlie AD and other dementias commence long before clinical manifestation and progress slowly this creates the prospect for developing interventions that aim at early identification and treatment of the preclinical stages of the disease.
In 2015, 47 million people were estimated to be living with dementia globally, and this number is projected to rapidly increase, reaching 75 million by 2030 and 135 million by 2050. 3 The estimated global cost (direct and indirect financial burden on healthcare) for dementia is $818 billion and is expected to increase to $2 trillion by the year 2030. 4 Recognizing this challenge, the World Health Organization has declared dementia prevention and treatment a public health priority, 5 and simulation studies suggest that even delaying disease onset by 2 years would have substantial public health, economic, and societal benefits.6,7
In this article, we review and critically appraise the latest evidence on interventions with potential role in the prevention of cognitive syndromes. In particular, we discuss strategies that target modifiable risk factors that have the potential to act before disease onset, increasing the cognitive reserve of healthy individuals and delaying the development of neuropathological changes characteristic of dementia. Early prevention strategies include lifestyle factors such as nutrition, exercise, stress reduction, amelioration of vascular risk factors like hypertension and diabetes mellitus, treatment of major depressive disorder (MDD), and immunomodulators. The review also highlights the latest evidence on strategies that examine later stages of cognitive syndromes, including interventions that aim at preventing the progression of mild cognitive impairment (MCI) to dementia. These include optimal control of vascular risk factors, stress reduction, and treatment of MDD, but also immunomodulators, vaccines, cognitive retraining, and non-invasive brain stimulation. Lastly, we discuss the challenges, future directions, and implications of this line of research.
Review criteria
The aim of this article is not to comprehensively review the entirety of the literature, but to highlight and critically appraise studies examining strategies that may hold promise for dementia prevention. The included studies were identified in Pubmed, EMBASE, and PsycINFO, using the following combinations of search terms: dementia, cognitive impairment, cognitive decline, Alzheimer’s disease, diet, nutrition, exercise, physical activity, vascular risk, hypertension, diabetes mellitus, cognitive training, stress reduction, MDD, antidepressants, immunomodulators. Although we included studies from all time periods, particular emphasis was placed on high-quality studies published in the last 5 years, including randomized controlled trials (RCTs), systematic reviews, and meta-analyses, but also observational studies in humans and relevant work in animal models.
Mild cognitive impairment and dementia: strategies for prevention
Evidence supports the existence of prodromal stages of dementia, including preclinical disease and the early clinical stage of MCI.8,9 The hallmark of MCI is the presence of cognitive deficits beyond what is expected for age but not severe enough to cause disruption of daily life.10,11 MCI represents a common prodrome of dementia with an annual conversion rate to clinically definite dementia of 10–15%.12,13 Given that different stages and trajectories of cognitive decline may vary in their response to distinct interventions, 14 distinguishing the various stages of the disease and the underlying pathogenic processes will be essential for the development of personalized prevention programs.
Epidemiological studies have highlighted the concept of ‘cognitive reserve’: individuals with a higher number of years of education and cognitive functioning status show symptoms of dementia later than those with lower educational status. However, once individuals with higher cognitive reserve exhibit symptoms of dementia, they show more rapid disease progression than individuals at the other end of the spectrum. This observation speaks to the complex relation between cognitive reserve and cognitive deterioration. 15
Existing literature, including the World Alzheimer Report, advocates for a multipronged approach to dementia prevention, given the role played by multiple risk factors for the disease. A total of 48.4% of dementia cases can be attributed to seven modifiable lifestyle risk factors: smoking, midlife obesity, physical inactivity, low educational attainment, diabetes mellitus, hypertension and MDD. 16 The World Alzheimer Report 2014 details an inverse relationship between physical activity and dementia, with pooled relative risk (RR) for dementia of 0.66 when comparing high versus low physical activity, whereas the pooled RR for AD is 1.52 when comparing smokers versus nonsmokers. The report also summarized benefits for cognitive stimulation on improvement in several cognitive domains, including executive function, attention and processing speed, and memory; but not working memory. 17
Nutrition and prevention of dementia
Evidence suggests that diet interventions may show promise for the prevention of cognitive decline. A recent systematic review that included 18 studies, 5 of which were RCTs showed that Mediterranean diet, a nutritional style based on fruits, vegetables, and fish can delay cognitive decline, as measured across multiple domains of memory and executive function. 18 These findings were consistent with an independent review that included only RCTs and found beneficial effects of Mediterranean diet on both global cognitive functioning, as well as memory, language, and domains of executive function. 19 Despite these effects on neuropsychological outcomes, however, there was overall no significant impact of Mediterranean diet on incident dementia and controversial impact on incident MCI. 19 Notably, the beneficial impact of the Mediterranean diet on cognition may be enhanced when combining this dietary style with the Dietary Approach to Systolic Hypertension (DASH) diet. Studies suggest that this hybrid diet is associated with delayed age-related cognitive decline and decreased risk for incident AD.20,21
Other nutritional components examined to date include omega-3 fatty acids, vitamins of the B complex, and vitamin E. However, a systematic review and meta-analysis, which included 24 RCTs, found no significant effects for any of these nutrients on cognitive function. 22 Beneficial effects have been reported by isolated studies for other nutrients, including green tea extract, 23 concord grape juice, 24 chromium picolinate, 25 vitamin D,26,27 and beta carotene. 28 The effect of vitamin B supplementation on progression of MCI to dementia was assessed by the VITACOG study. Significant delay of brain atrophy was observed with a combination of vitamin B12, folate, and pyridoxine compared with placebo, especially in people with high homocysteine levels. 29 In the Finnish Diabetes Prevention Study, lower intake of saturated fatty acids, as well as frequent physical activity, correlated with better cognitive performance measured over a period of 13 years.30,31 This preliminary evidence requires further examination by future studies.
In summary, Mediterranean diet, both alone and in combination with DASH, may be beneficial for the prevention of cognitive decline. Future studies will need to rule out potential confounders and better characterize the mechanisms underlying the role of nutrition in cognitive outcomes. For example, it will be important to characterize whether dietary modifications may influence dementia risk via effects on biological processes relevant for neuronal function, including the amelioration of oxidative stress and the maintenance of neuronal membrane integrity, 32 or to what extent this influence results indirectly from the attenuation of other risk factors for dementia, such as hypertension or excessive body weight. 33
Physical exercise and dementia prevention
Association between physical activity/exercise and cognition
Evidence suggests that physical exercise may improve cognition in older adults with normal cognitive function, but also in individuals with different levels of cognitive impairment. Beneficial effects on cognition have been shown for aerobic and resistance exercise in both humans and rodent studies.34–37 Multiple long-term follow-up studies have explored the connection between physical activity and dementia, including the LADIS study, 38 the Rotterdam Study, 39 and the Caerphilly Prospective study. 40 In a landmark trial evaluating the usefulness of combining physical exercise and cognitive training in adults with cognitive impairment [Mental Activity and eXercise (MAX) trial], all participant groups showed cognitive improvement. The study lacked a pure control group and all participants received some form of physical and mental stimulatory exercise (mental activity and exercise for 60 min/day for 3 days/week for 12 weeks). The study found that the amount of activity is more important than the type of activity.41,42 In another study, exercise was found to be more effective in slowing down cognitive decline than was cognitive training. 43 In accordance, older adults with normal cognitive functioning who engaged in 3–4 instances of moderate-to-vigorous-intensity exercise of at least 30 min duration every week showed lower risk for cognitive decline over the course of 8 years. 44 In individuals with MCI, physical exercise can improve several cognitive domains, including verbal and spatial memory, 45 and even delay progression to dementia. 46 In patients with dementia, evidence from 18 RCTs, recently synthesized in a meta-analysis, showed that aerobic exercise alone or in combination with nonaerobic exercise may improve cognitive function. 47
Mechanisms by which physical activity/exercise may aid cognition
Postulated mechanisms for the beneficial effects of exercise on cognition include the enhancement of neurotrophin production and signaling,48–50 the induction of angiogenesis and blood flow in the brain,51,52 the amelioration of inflammatory processes, 53 and the induction of epigenetic modifications in brain regions relevant for cognition. 54
Recent studies and ongoing trials
Recent studies have also coupled physical exercise with other interventions. The Life Randomized Trial (Lifestyle Interventions and Independence for Elders) recruited 1635 community-living participants at risk for cognitive impairment at eight US centers from February 2010 until December 2011. The interventions comprised either a structured, moderate-intensity physical activity program, which included walking, resistance training, and flexibility exercises, or a health education program of educational workshops and upper-extremity stretching. No differences in executive function were observed between the two interventions over a period of 24 months when comparing adults over 80 years of age or those with lower baseline physical activity performance who did benefit with the physical activity intervention. 55
Several ongoing trials seek to better characterize the effect of physical exercise on cognitive decline. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) is an ongoing trial recruiting individuals whose cognitive performance is lower than average to participate in a multidomain intervention trial over a 2-year period. Interventions comprise nutritional guidance, exercise, education on vascular risk factors and cognitive retraining. Nutritional interventions comprise a diet low in carbohydrates and salt, and with adequate amounts of unsaturated fatty acids (from fish). Exercise consists of weekly physical activity encompassing both aerobic exercise and muscle-strength training ranging from 30 to 60 min. Preliminary results suggest some beneficial effect on cognitive domains assessed with a neuropsychological battery for the intervention group as compared with the control group. 56 Another ongoing trial will examine the combination of lean red meat consumption and exercise (220 g of lean red meat cooked and divided into two 80 g servings on each of the 3 days that they complete their exercise session) in the form of progressive resistance training (PRT) in community-dwelling individuals aged > 65 years for a duration of 48 weeks. In this trial, PRT comprises a detailed exercise regimen that occurs in 3 consecutive days of a week ranging a duration of 30–75 min. Outcomes include muscle mass, cognitive performance and inflammatory serum markers. 57 The Australian Imaging Biomarkers and Lifestyle Flagship Study of Aging (AIBL) will examine if a combination of moderate home-based physical activity (150 min every week) and behavioral interventions over a period of 24 weeks in patients with MCI and vascular risk factors would cause changes in white matter hyperintensities on magnetic resonance imaging (MRI), changes in cognition, and positron emission tomography (PET)-measured amyloid–beta (Aβ) burden. 58 The Multidomain Alzheimer Preventive Trial (MAPT study) aims at assessing the effect of a combined approach with omega-3 fatty acids, physical activity, nutritional counseling, and cognitive training in a group of adults with cognitive impairment over a period of 3 years. 59
Future directions
Challenges faced by studies examining the impact of physical exercise on dementia prevention include the interindividual variability in response to these interventions, differences between physical activity and exercise, the difficulty in quantifying benefits, and the heterogeneity of interventions across studies, which overall impede replication efforts. Although physical activity has moderate effect size in the World Alzheimer’s Disease Report, 17 more RCTs are required to validate its recommendation as a lifestyle intervention.
Vascular risk factors and dementia prevention
Vascular disease can predispose to the development of dementia syndromes, including vascular dementia and AD.60–62 Therefore, the amelioration of predisposing conditions for vascular pathology, such as hypertension, dyslipidemia, and diabetes, may be an important target for dementia prevention.
The relationship of antihypertensive treatment and risk for dementia has been examined by both observational studies and RCTs. A recent systematic review found that antihypertensive medications may result in 19–55% reduced risk of cognitive decline, vascular dementia, and AD. 63 Nonetheless, the effect of antihypertensive treatment on dementia risk is weaker when considering only RCTs, 64 suggesting the presence of confounding factors. A previous meta-analysis concluded that antihypertensive treatment could only decrease the risk of vascular dementia but not Alzheimer dementia or cognitive decline. 65 In addition, negative results have been reported when examining subjects without vascular disease,66,67 indicating that antihypertensive medications may be more effective as a prevention strategy if targeted at individuals with high risk for vascular disease. Among the classes of antihypertensive medications, the strongest effect has been observed for modulators of the renin–angiotensin system (RAS), which may decrease the risk for cognitive decline and dementia and slow conversion of MCI to dementia.63,68,69 The effect of RAS modulators may be to an extent explained by their actions in brain regions relevant for cognition that are independent of effects in the vasculature. 70 Supporting this hypothesis, polymorphisms of RAS genes were associated with hippocampal volume loss and longitudinal decline in the episodic memory performance of older adults.71,72 These findings also raise the possibility that targeting carriers of these polymorphisms with RAS modulators may be a promising strategy for the prevention of dementia.
Studies have also examined the potential role of interventions for dyslipidemia, but there is currently limited evidence to support their role in dementia prevention. Prospective studies have found an association of lipid-lowering drugs, and in particular statins, with decreased risk for MCI and dementia,73–75 and this association may be independent of other vascular risk factors. 74 Despite these encouraging reports, RCTs to date have shown contradictory results and a recent systematic review reported no significant effect of statins on risk for cognitive decline or dementia.76,77 Further studies that control for concomitant vascular risk factors and other potential confounders will need to delineate the potential role of lipid-lowering interventions for dementia prevention.
Lastly, studies have examined the potential to prevent dementia by treating diabetes mellitus. Association studies suggest that patients with diabetes have up to three times higher risk for the development of dementia,78–80 and this risk remains significant after adjusting for other vascular risk factors. 81 Notably, diabetes may confer greater risk for vascular dementia in women than in men, 82 suggesting that vascular risk factors for dementia may have sex-specific effects. Longitudinal studies have also observed increased incidence of dementia in patients with diabetes. 83 However, negative findings are also reported, 84 and a systematic review of RCTs found no effect of treatment of diabetes mellitus on cognitive decline. 85 Potential explanations for these discrepancies include the heterogeneity in the populations studied and the inadequate adjustment for potential confounders. Beyond the acceleration of microvascular pathology in the brains of diabetic patients, diabetes may confer risk for cognitive impairment through other end-organ damage, such as diabetic retinopathy, and through fluctuations in blood glucose and insulin levels that could influence clearance of Aβ.86–88
Major depressive disorder and risk for cognitive decline
Neurobiological mechanisms
MDD is strongly associated with increased risk for cognitive decline,80,89,90 but the causal direction of this association remains unclear. Most studies have examined MDD occurring in late life, proposing that depressive syndromes could be a sequela, prodrome, or risk factor for dementia. 91 Depressive episodes have been associated with persistent deficits in select cognitive domains, including psychomotor retardation and executive function, 92 which may in turn predict worse antidepressant treatment outcomes. 93 Notably, the increasing burden of depressive illness, manifested by earlier onset, repetitive MDD episodes, and greater illness severity and duration, may cumulatively increase the risk for dementia94–96 and predict structural brain changes that are associated with higher risk for cognitive decline, such as hippocampal and cortical atrophy.97–99 MDD may further accelerate the progression of MCI to dementia.100,101 Beyond the MDD-related hippocampal and brain atrophy, other plausible neurobiological substrates linking MDD and cognitive decline include the downregulation of neurotrophins, the accumulation of Aβ, and the accentuation of age-related vascular changes and inflammatory processes in brain circuits with critical roles in mood and cognition.102–104 Furthermore, MDD throughout life contributes to higher risk for cerebrovascular disease in a dose–effect manner,105–108 thus increasing the likelihood for the clinical expression of dementia as amyloid and other brain pathologies progress. 109
Evidence linking major depressive disorder and cognitive decline
While the sequence and exact role of these pathogenic events remain to be determined, the findings to date suggest that timely identification and treatment of MDD, which is a highly prevalent disorder impacting every age and population, may substantially influence cognitive functioning in late life. RCTs examining this question show that effective treatment of MDD may result in improvements across several cognitive domains, including attention, psychomotor speed, and executive function.110–112 Most RCTs reporting beneficial effects have utilized selective serotonin reuptake inhibitors,110,111,113 whereas negative findings have been reported in observational studies114,115 and studies utilizing tricyclic antidepressants. 116 The identification and treatment of MDD may be more effective when targeted at high-risk subjects; for example, untreated depression has been shown to increase risk for negative cognitive outcomes following stressful life experiences. 117
Despite these observations, there is a paucity of studies examining the long-term impact of MDD treatment on incident dementia. Furthermore, several challenges are involved in the selection of antidepressant strategies, particularly in patients with cerebrovascular disease. Antidepressants are the most commonly used treatment for MDD but their efficacy is modest, at best helping 50% of patients. The efficacy of antidepressants is even lower in older patients, and their use has been linked to cerebrovascular stigmata. Complicating the picture further, recent studies have reported an association of antidepressants with increased risk for ischemic and hemorrhagic stroke. The Women’s Health Initiative reported a 45% increase in the risk of stroke. 118 A large case-control study also found antidepressants to be linked with a 20–40% increase in the risk of stroke, 119 but disagreement on this association exists.120,121
Nonpharmacological, behavioral interventions are a reasonable intervention for MDD without the risk of increasing vascular pathology. An additional advantage of nonpharmacological therapies is that they can target both depression and poor health behaviors that increase the risk of stroke. However, most nonpharmacological therapies are complex, are rarely implemented in the community correctly, and have limited scalability and reach. We have proposed that neurobiological concepts can be used to identify distinct behavioral targets and use them, as simplification rules to streamline behavioral interventions to enable their use by community clinicians. We used concepts of the Research Domain Criteria project and our findings to develop a neurobiological model of depression and utilized it in a simplified behavioral intervention (Engage), 122 which appears to have similar efficacy to problem-solving therapy. 123
Treatment of major depressive disorder to prevent cognitive decline
Antidepressant and mood-stabilizing strategies have also been examined in patients who already have some degree of cognitive impairment. In a group of healthy subjects, 60 mg of citalopram given in divided doses of 30 mg reduced (Aβ) production by 38% compared with placebo. 124 In a group of 45 patients with MCI treated with lithium versus placebo, treatment with lithium titrated to a blood level of 0.25–0.5 mEq/l for a year slowed down cognitive deterioration compared with placebo, as measured with the Alzheimer’s Disease Assessment Scale-Cognitive subscale. Lithium also decreased the level of phosphorylated tau in patients with MCI. 125 In a study examining the association between amyloid pathology and remission of depressive symptoms with electroconvulsive therapy (ECT), remitters showed significantly lower Aβ40/Aβ42 than nonremitters. 126 In a group of patients with MDD receiving ECT, there were changes in levels of CSF Aβ1-42, the (Aβ) isoform with highest amyloidogenic potential. 127 RCTs examining dementia prevention as a result of ECT are lacking; however, evidence points to an increase in hippocampal volume with ECT,128,129 thus providing a pathophysiological basis for the potential role of severe MDD treatment in dementia prevention.130,131
The role of pharmacological and nonpharmacological antidepressant strategies in preventing dementia onset and progression warrants further examination by future studies.
Stress reduction as a dementia prevention strategy: role of meditation
Psychosocial stressors, most notably chronic and perceived stress, have been associated with lower levels of cognitive performance across several domains and with faster cognitive decline in both healthy adults and subjects with MCI.132–137 Furthermore, chronic stress may indirectly influence cognitive function by moderating the impact of other risk factors on cognitive function; for example, metabolic risk factors strongly accelerate the 8-year cognitive decline in chronically stressed caregivers of a relative with dementia. 138 These observations in human studies are congruent with a large body of evidence in rodent and other vertebrate models indicating that chronic stress can impair cognitive performance.139–141 Notably, this negative influence is observed when stressors are unpredictable, whereas mild predictable stress may actually enhance cognitive performance. 142 Furthermore, the impact of chronic stress can manifest long after stressor cessation; for instance, stress exposure during adolescence may impair spatial memory when mice age. 143 The effects of stress on cognitive function may be mediated by several mechanisms, including the accumulation of Aβ in the brain,144,145 the induction of brain inflammation, 146 epigenetic modifications mediated by stress-induced glucocorticoid deregulation,147–149 and changes in brain structures with central roles in cognition, such as the hippocampus.150–152 Some of these effects, however, may vary depending on the timing and duration of stress exposure.148,153
The negative impact of chronic and perceived stress on cognition suggests that interventions aiming at controlling stress levels may be beneficial for dementia prevention. Supporting this notion, regular meditation may improve cognitive function of healthy individuals.154,155 Furthermore, preliminary evidence suggests that long-term meditation may delay age-related decline of several cognitive functions156,157 and improve some neuropsychological outcomes in subjects with MCI. 158 A randomized trial which employed mindfulness-based stress reduction (MBSR) found that MBSR-treated patients with MCI showed improved cognitive performance compared with the those who received usual care. 159 Furthermore, MBSR increased functional connectivity between the posterior cingulate cortex and bilateral medial prefrontal cortex and left hippocampus in adults with MCI. 160 Although these findings are encouraging, the small sample sizes and potential confounders of studies to date limit conclusions and call for confirmation by larger RCTs.
Prevention by addressing other lifestyle parameters
Several other lifestyle parameters, including the level of education, smoking, and alcohol consumption may influence the incidence of dementia.87,161,162 Given that such factors frequently coexist within individuals and synergize to influence the risk for cognitive decline, interventions that address multiple risk factors in a coordinated manner are more likely to prove beneficial for the early prevention of dementia.
Cognitive retraining and dementia
Cognitive interventions for dementia syndromes encompass a wide range of modalities, including cognitive training that targets one domain and increasing task difficulty as expertise develops, cognitive stimulation targeting multiple domains with emphasis on social interaction, and cognitive rehabilitation tailored at improving activities of daily living. These interventions aim at enhancing cognitive reserve, that is, the structural and dynamic capacities of brain circuits that compensate when one or more brain regions do not function adequately, thus increasing resilience against the neuropathological changes of dementia.15,163 Several long-term follow-up studies have looked at trajectories of cognitive impairment and the effect of cognitive stimulation, including the German Interdisciplinary Longitudinal Study on Adult Development and Aging Study, the Minority Aging Research Study, the Memory and Ageing Project, the Chicago Health and Ageing Project, and the Betula prospective cohort study. The PACE study was an RCT designed to study the effect of cognitive interventions on the progression of MCI. The intervention group received supervised education on cognitive retraining strategies. Over a period of 2 years, there was no significant effect on progression to dementia; 164 however, a limitation of the trial was the lack of active supervised task engagement for the participants of the intervention group beyond the 5-week intervention period.
Non-invasive brain stimulation to modify the course of dementia
A recent meta-analysis showed that non-invasive modalities of brain stimulation (including repetitive transcranial magnetic stimulation and transcranial direct current stimulation) may significantly improve cognitive function in both healthy older adults and patients with AD. 165 Notably, multiple sessions of brain stimulation were twice as effective in improving cognition than were single sessions, suggesting that a sustained treatment effect is needed to modify brain function. However, studies to date are limited by the short duration of the follow-up after the intervention,166–169 not allowing conclusions about the long-term impact of brain stimulation on the development and course of dementia. Notably, preliminary evidence suggests that the lack of neuropsychological and electrophysiological response to brain stimulation may represent a biomarker of increased risk for progression of MCI to dementia. 131 These findings and the role of brain stimulation in dementia prevention warrant further examination by longitudinal RCTs with long duration of follow up.
Immunomodulators to prevent dementia
The effect of immunomodulators, including active immunization using vaccines and passive immunization with chimeric antibodies, have also been evaluated as a therapeutic strategy in AD. 170 Active immunization to date includes either the use of tau peptide conjugates or the use of prefibrillized synthetic (Aβ1–42). Tau is a phosphoprotein with 85 phosphorylation sites. Selective targeting of individual sites with engineered tau peptide conjugate is one way of active immunization. In rodent models, active vaccination has achieved a striking decrease in tau oligomer aggregation, tau hyperphosphorylation, and neurofibrillary burden. 171 In humans, however, the initial vaccine used, AN1972 (combination of prefibrillized synthetic Aβ and adjuvant), had modest efficacy on cognitive functioning, and clinical trials were halted due to the adverse effect of subacute meningoencephalitis. 172 Newer vaccines, such as ACC-001 (also known as Vanutide cridificar), containing multiple short Aβ fragments linked to a carrier made of inactivated diphtheria toxin demonstrated a safer profile in phase II trials, 173 but did not prove to be efficacious and trials were discontinued. 174 AADvac-1 is a vaccine which is currently in a phase II trial and consists of modified tau protein (synthetic peptide derived from amino acids 294–305 of the tau sequence, coupled with hemocyanin). Passive immunization, using agents such as bapineuzumab and solanezumab, has been tested in phase III trials. Patients with mild or moderate dementia treated with bapineuzumab showed no substantial improvement in any primary cognitive outcome, and the main adverse effect related to the drug was vasogenic cerebral edema. 175 Trials with solanezumab (EXPEDITION 1, 2 and 3 and EXPEDITION-PRO) did not show robust changes in cognition, and a phase III trial was recently terminated (NCT01850238, NCT02031198). Other immunomodulators being tested include intravenous immunoglobulin infusions and passive immunization with gantenerumab, BAN2401, aducanumab, and crenezumab. The potential role of these approaches in preventing dementia remains to be determined.
Conclusion and future directions
As summarized in Figure 1 and Table 1, several preventive strategies have been examined to date, but there is currently limited evidence to support a cause–effect relationship between any strategy and the development or progression of dementia. Most animal studies have targeted the amyloid cascade in the pathogenesis of dementia, showing encouraging or even enthusiastic results in model organisms; however, therapeutic interventions derived from these studies have not been able to meaningfully impact disease course. This lack of therapeutic translation calls for animal models that target novel mechanisms and encapsulate the multifactorial processes implicated in the pathogenesis and progression of dementia. Studies in humans face major challenges, including the multiple confounding factors, the clinical heterogeneity of dementia syndromes, and the need to properly randomize and follow subjects over the long term. Keeping these limitations in mind, studies to date indicate that a multifactorial intervention approach characterized by regular exercise and healthy diet, along with the amelioration of vascular risk factors, psychosocial stress, and major depressive episodes, may be most promising for the prevention of cognitive decline. Future studies may help to determine the exact role of these interventions and to identify novel modalities with therapeutic benefit for the different stages of cognitive decline.
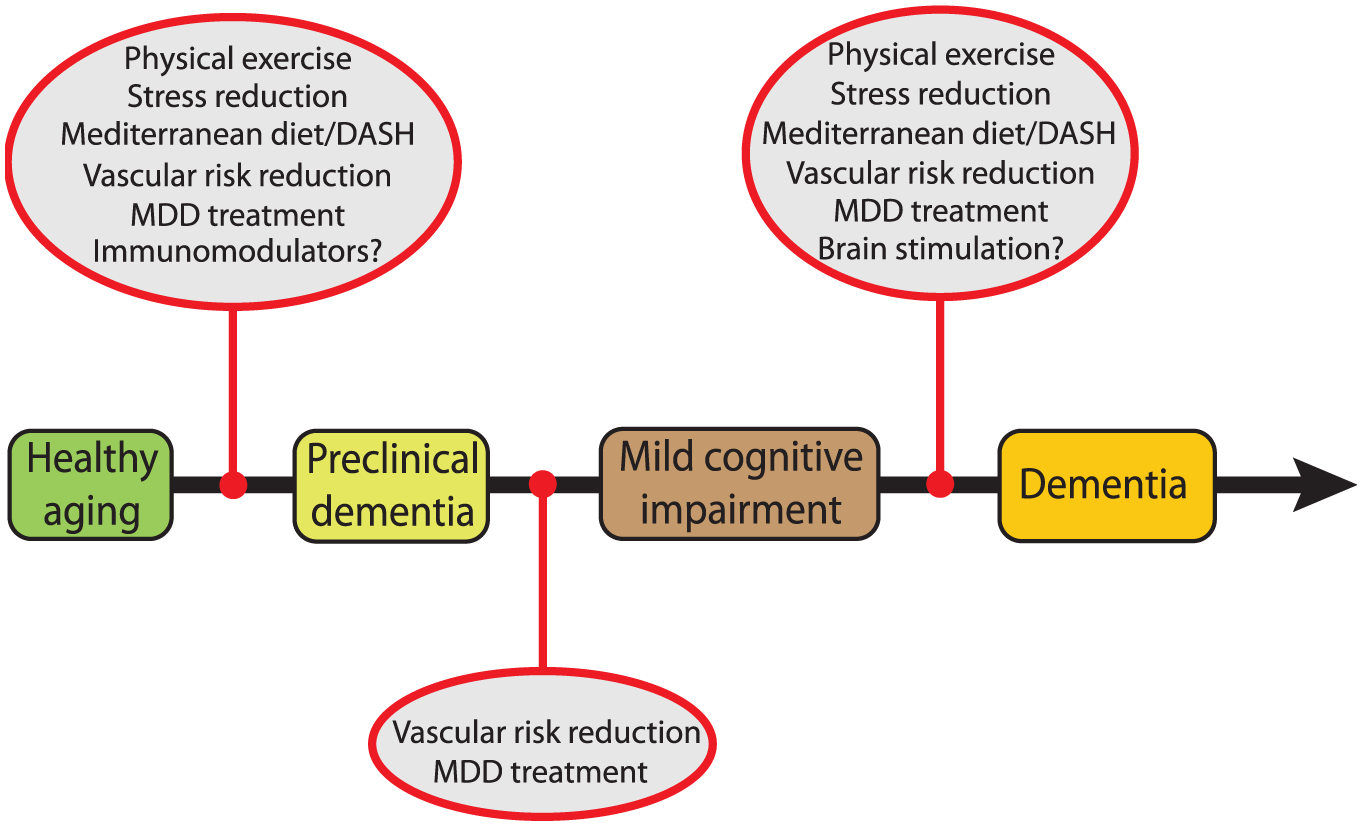
Schematic summary of the strategies that may show promise for the prevention of dementia at different stages of the disease. Details for each intervention are provided in the text. Overall, the evidence for preventing dementia is, to date, limited, and the exact role of these interventions warrants further examination by future studies.
Overall appraisal of existing strategies for the prevention of cognitive decline (rating is based on the GRADE system). 176

++, moderate; ++, low; +, very low; MDD, major depressive disorder.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.