
Abstract
Background:
The aim of this study was to investigate the relationship among management modality, glycemic control, components of metabolic syndrome (MS) and serum levels of γ glutamyl transferase (GGT) and C-reactive protein (CRP) in patients with type 2 diabetes (T2DM).
Methods:
Patients with T2DM, not suffering from diabetes complications, were recruited from outpatients clinics at two hospitals in Jeddah. Anthropometric measurements and blood pressure (BP) were taken. A treatment plan was recorded. Fasting blood samples were obtained to measure glucose, glycated hemoglobin (HbA1c), lipids profile, highly sensitive (hs)-CRP and GGT.
Results:
A total of 71 men and 82 women were recruited. Lower mean HbA1c was found in people receiving oral glucose-lowering drugs compared with those on insulin therapy (p < 0.001). Management modality had no effect on mean GGT or hs-CRP. Higher mean GGT was associated with poor glycemic control, dyslipidemia, hypertension, and abdominal obesity. GGT correlated significantly (p < 0.05) and directly with triglycerides in men (r = 0.401) and diastolic BP (r = 0.279 for men, r = 0.194, for women), but inversely with high-density lipoprotein cholesterol (HDL-C) (r = −0.298 for men, r = −0.171 for women). hs-CRP correlated with waist circumference (p < 0.05, r = 0.312, for men, r = 0.305, for women), with a higher mean being found in men with poor glycemic control (p = 0.015), in hypertensive women (p = 0.030), and in patients who were abdominally obese (p < 0.05).
Conclusions:
High levels of GGT and hs-CRP are associated with components of MS and poor glycemic control, hence increased cardiovascular risk. Due to their value as independent risk predictors of vascular injury, these measures should be included in routine monitoring of patients with T2DM.
Introduction
The prevalence of type 2 diabetes mellitus (T2DM) is one of the highest globally amongst the adult population of Saudi Arabia [IDF, 2014]. New Saudi guidelines for the management of T2DM were issued in 2014 [Ministry of Health, 2014]. These guidelines encourage the use of insulin therapy as monotherapy or combined with oral glucose-lowering drugs to treat inadequately controlled patients, in addition to the usual need for patient education, self-management, and diet therapy. In the face of the commonly noted poor glycemic control among their patients [Alfadda and Abdulrahman, 2006; Al-Elq, 2009; Al-Rowais, 2014], and the absence of well structured and continuous patient education programs, there has been increased dependence on insulin therapy by physicians, in particular to decrease microvascular complications associated with the disease [Ohkubo et al. 1995; UKPDS Group, 1998a&b]. Even though insulin therapy has been reported to be very effective in controlling all levels of hyperglycemia and coexisting dyslipidemia [Nathan et al. 1988], it was also reported to increase body weight and the frequency of hypoglycemic episodes [Diabetes Control and Complications Trial Research Group (Dcactrg), 1993]. Furthermore, the use of insulin therapy was found to be associated with increased risk of cardiovascular disease (CVD), both directly [Stout, 1996] and indirectly due to weight gain [Meigs et al. 2006]. Increased risk of CVD has also been associated with increased levels of C-reactive protein (CRP) [Ridker, 2003; Arad et al. 2005], and the presence of the metabolic syndrome (MS) [Lakka et al. 2002; Galassi et al. 2006]. In addition, it was reported that elevated levels of γ glutamyl transferase (GGT), even within the clinically normal range, are associated with increased risk of T2DM, hypertension, and cardiovascular events, making it an independent risk factor for the development of cardiovascular or cerebrovascular diseases [Lee et al. 2003; Mason et al. 2010; Bradley et al. 2014]. The aim of our study was to investigate the relationship among management modality, glycemic control, components of MS, and serum levels of GGT and CRP in Saudi patients with T2DM.
Patients and methods
Patients with T2DM were randomly selected using a table of random numbers to be included in a cross-sectional study carried out in outpatient clinics at King Abdulaziz University Hospital (KAUH), and King Fahad Armed Forces Hospital (KFAFH) in Jeddah, Saudi Arabia, during June and July 2014. The Committee on the Ethics of Human Research at the Faculty of Medicine, King Abdulaziz University, and the Committee on the Ethics of Medical Research at KFAFH granted the ethical approval for the study. An informed consent form was signed by the patients willing to participate. Pregnant women and patients having any severe chronic illness or severe diabetic complications (i.e. end-stage renal disease, liver disease, recent myocardial infarction, etc.) were excluded. A total of 153 patients were recruited (46.4% men, 53.6% women). Blood pressure (BP) was measured following the recommendations of the American Heart Association Council [Pickering et al. 2005], using a standard mercury sphygmomanometer with the cuff on the right upper arm. Two BP readings were taken, 1 min apart, while patients were seated for 10 min. The mean of the two values was calculated. Height was measured bare footed to the nearest 0.5 cm using a stationary stadiometer. Weight was measured to the nearest 0.5 kg while wearing light street clothing using a calibrated scale. Body mass index (BMI) was calculated using both measurements. Waist measurement was taken at the level of the umbilicus and hip measurement at the maximal protrusion of the gluteal muscles, both to the nearest 0.5 cm. BMI was used to classify patients as being normal weight (18.5 to <25 kg/m2), overweight (25 to <30 kg/m2), or obese (⩾30 kg/m2) [WHO, 2015]. In addition, a face-to-face interview was conducted using a structured questionnaire to obtain demographic information and a management plan was followed by patients to control their diabetes. The treatment regimen was recorded and included lifestyle modification (i.e. diet and exercise), oral hypoglycemic agents (metformin, sulfonylurea, α glucosidase inhibitor, thiazolidinedione, or Dipeptidyl Peptidase (DPP) 4 inhibitor), insulin, noninsulin injectable drugs (Glucagon Like Peptide (GLP)-1 agonist), or any combination of them. Fasting blood sample was obtained for measurement of glucose, glycated hemoglobin (HbA1c) lipids profile, highly sensitive CRP (hs-CRP), and GGT. Serum glucose and lipids [cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-C)] were assayed using automated enzymatic methods (Dimension Vista 1500T Intelligent Lab System from Siemens Company-Germany) at the biochemistry laboratory. Low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald equation [Friedewald et al. 1972]. HbA1c analysis was performed on Dimension Vista 1500T Intelligent Lab System. HbA1c up to 7% reflected adequate glycemic control, while HbA1c greater than 7% reflected poor glycemic control, as recommended by the American Diabetic Associa-tion guidelines [Dc, 2014]. Hypertension was defined as a systolic BP greater than 140 mmHg or diastolic BP greater than 90 mmHg, or current use of antihypertensive drug treatment [Chobanian et al. 2003]. The consensus definition [Alberti et al. 2009] was used to define MS.
Statistical analysis
Data were entered, coded, and analyzed using SPSS version 20. Descriptive statistics, such as mean ± standard deviation (SD) or standard error of the mean (SEM), were calculated for all estimated parameters. Comparison between two means was performed using unpaired Student t test for normally distributed parameters and the Mann Whitney U test for non-normally distributed parameters. Differences between more than two means were tested using one-way analysis of variance analysis. χ2 test was used for categorical variables. Associations between variables were examined using Pearson’s correlation coefficients. All p values that were less than 0.05 were deemed statistically significant.
Results
The studied group included 71 men and 82 women. Women had a significantly higher mean age (mean ± SD: 56.0 ± 11.5 years for men compared with 60.4 ± 10.1 years for women,p = 0.021), BMI (mean ± SD: 30.6 ± 5.4 kg/m2 for men compared with 32.6 ± 6.1 kg/m2 for women, p = 0.033), and diastolic BP (mean ± SD: 74 ± 11 mmHg for men compared with 78 ± 11 mmHg for women, p = 0.016). A low percentage of patients had BMI within the normal range (14.3% for men and 12.3% for women) and a high percentage were classified as obese (51.4% for men and 69.1% for women). No significant differences in means of systolic BP, waist circumference, or duration of diabetes were noted between men and women (p = 0.248, 0.232, and 0.529 respectively). Neither were there significant differences in the percentage of BMI classes, prevalence of hypertension, and MS between the two sexes (p = 0.059, 0.818, and 0.122 respectively). However, a higher percentage of abdominal obesity (
The results of measured biochemical parameters and BP, expressed as mean ± SEM, after classifying subjects according to treatment modality, are presented in Table 1. Almost half of the patients (45.8%) were on insulin therapy, either alone or combined with oral glucose-lowering drugs. The mean age as well as sex distribution among the three treatment groups did not differ significantly. However, patients receiving oral hypoglycemic drugs had significantly shorter mean duration of disease (mean ± SD = 7.96 ± 1.51 years) compared with patients on insulin (9.64 ± 2.32 years), or those receiving combination therapy (9.50 ± 1.84 years) (p = 0.001).
Measured biochemical variables and blood pressure (BP) according to treatment modality (mean ± SEM).

Total number = 83, men = 42.2%, women = 57.8%.
Total number = 20, men=65.0%, women = 35.0%.
Total number = 50, men = 44.0%, women = 56.0%.
GGT, γ glutamyl transferase; hs-CRP, highly sensitive C-reactive protein; SEM, standard error of the mean. Statistically significant values are shown in bold font.
A significantly lower mean HbA1c was noted in patients receiving oral glucose-lowering drugs compared with those on insulin monotherapy or combined with oral drugs (p < 0.001), and a significantly lower mean diastolic BP was found in patients receiving insulin (p = 0.025). No significant difference was found in the means of GGT or hs-CRP between the two treatment groups.
Correlations of hs-CRP and GGT with each other, as well as with HbA1c and different components of MS, in studied subjects are presented in Table 2.
Correlations between hs-CRP and GGT with HbA1c and different components of MS in male and female patients.
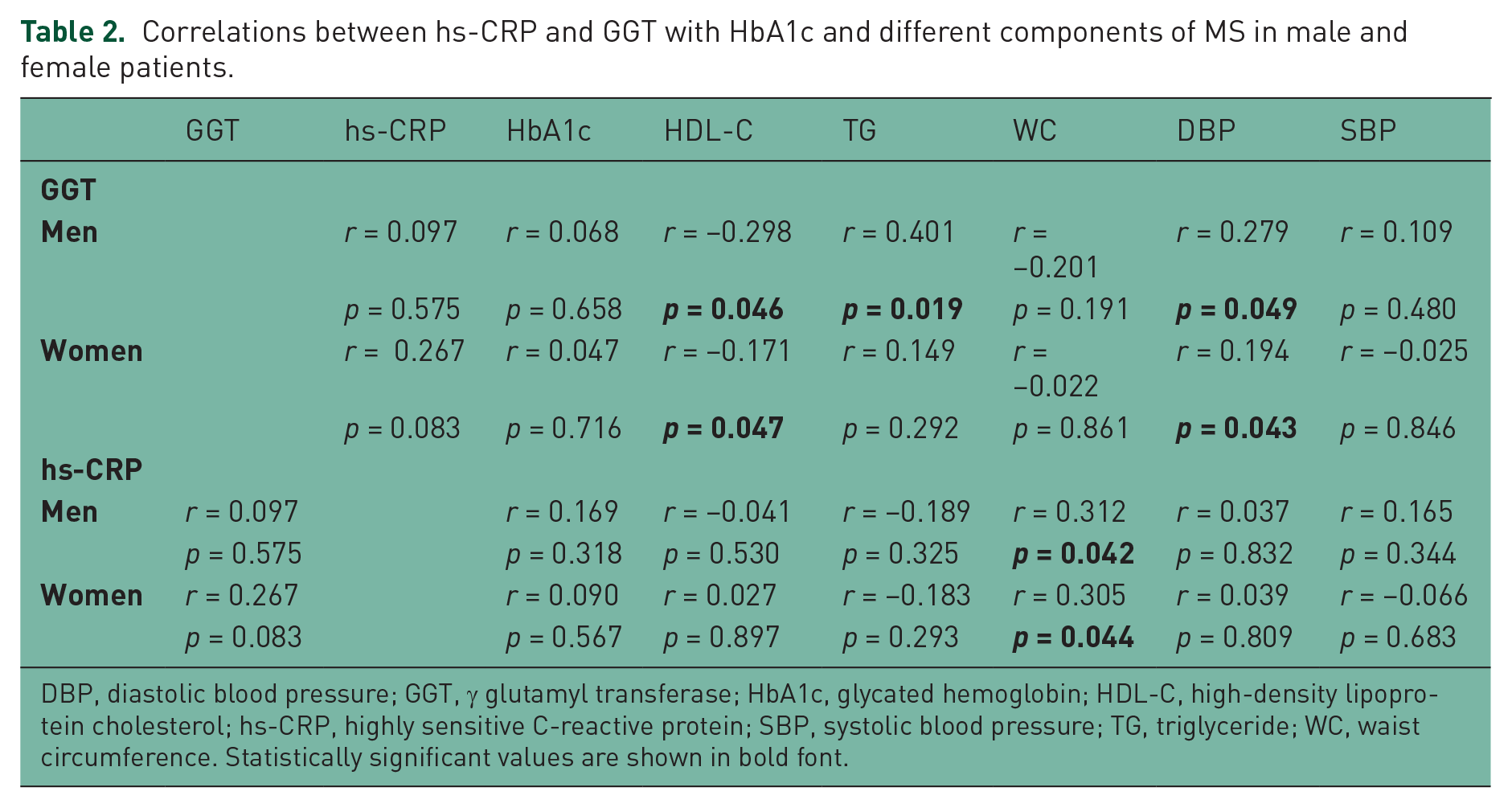
DBP, diastolic blood pressure; GGT, γ glutamyl transferase; HbA1c, glycated hemoglobin; HDL-C, high-density lipoprotein cholesterol; hs-CRP, highly sensitive C-reactive protein; SBP, systolic blood pressure; TG, triglyceride; WC, waist circumference. Statistically significant values are shown in bold font.
GGT correlated directly with DBP and inversely with HDL-C level in both sexes. It also directly correlated with triglyceride level in men only. Serum level of hs-CRP correlated only with WC in both sexes. The correlation between hs-CRP and GGT was not significant.
The means of hs-CRP and GGT in male and female patients according to their status of glycemic control, as well as the presence or absence of hypertension, dyslipidemia, and abdominal obesity, are presented in Table 3.
The means of GGT and hs-CRP in male and female patients in the presence and absence of poor glycemic control, hypertension, dyslipidemia, and abdominal obesity.

Glycemic control defined as poor, if HbA1c > 7%.
Dyslipidemia defined yes if LDL ⩾ 3.37 mmol/liter, HDL < 1.04 mmol/liter for men and <1.3 mmol/liter for women, total cholesterol ⩾ 5.18 mmol/liter, triglycerides ⩾ 1.7 mmol/liter or treatment with lipid-lowering drugs.
Hypertension defined yes if systolic BP > 140 mmHg or diastolic BP > 90 mmHg or current use of antihypertensive drug treatment.
Abdominal obesity defined as yes if WC ⩾ 102 cm in men and ⩾ 88 cm in women.
BP, blood pressure; GGT, γ glutamyl transferase; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; hs-CRP, highly sensitive C-reactive protein; LDL, low-density lipoprotein; SEM, standard error of the mean; WC, waist circumference. Statistically significant values are shown in bold font.
Poor glycemic control was associated with a significantly higher mean hs-CRP in men, and with the presence of hypertension in women. However, a significantly higher mean in people with abdominal obesity was noted for both sexes. Furthermore, the percentage of patients with high serum hs-CRP level (>3 mg/l) among those with poor glycemic control was 32.3% for men and 33.3% for women, compared with 0% in men and 38.5% in women with adequate glycemic control. Moreover, 37.5% of men and 35.7% of women with abdominal obesity had high serum hs-CRP level compared with 7.7% of lean men and 0% of lean women. While more women with dyslipidemia and hypertension had high hs-CRP compared with normolipidemic and normotensive women, in men the situation was different since dyslipidemic and hypertensive men had a lower prevalence of high hs-CRP compared with normotensive and normolipidemic men.
A significantly higher mean GGT was seen in patients with poor glycemic control of both sexes, and in men with dyslipidemia, as well as in women with hypertension and abdominal obesity.
Discussion
Diabetes mellitus is associated with a myriad of micro- and macrovascular complications. Hyperglycemia, increased BP, dyslipidemia (components of MS), inflammation, and oxidative stress are all characteristics of T2DM and are implicated in the development of vascular complications [Hypertension in Diabetes Study, 1993; Klein, 1995; Klein et al. 1996; Turner et al. 1998; Beckman et al. 2002; Fong et al. 2004; Boyle, 2007], so that their control leads to decreased risk of both complications [Diabetes Control and Complications Trial Research Group, 1993; Kunisaki et al. 1995; UKPDS, 1998c; Heart Outcomes Prevention Evaluation Study Investigators, 2000; Rossing et al. 2003; Colhoun et al. 2004]. Adequate glycemic control is the main goal for diabetes management. Most of the patients participating in our study were uncontrolled no matter which glucose-lowering treatment modality was used, as has been reported earlier in other studies in Saudi Arabia [Alfadda and Abdulrahman, 2006; Al-Elq, 2009; Al-Rowais, 2014]. Insulin therapy, either alone or combined with oral glucose-lowering drugs, is implemented in patients with T2DM whose condition is not adequately controlled by oral drugs, and is expected to produce better glycemic control in such patients [Nathan et al. 1988; Ohkubo et al. 1995; UKPDS, 1998a &b]. The Steno-2 study has clearly demonstrated the importance of a multimodal treatment strategy in patients with T2DM [Gaede et al., 2003] (38). However, In our study higher mean HbA1c was found in patients receiving insulin and the lowest mean in those taking oral hypoglycemic drugs. Suspected lack of compliance with insulin therapy could be the cause, but further studies are needed to clarify all causes and to suggest solutions to achieving adequate glycemic control.
In addition to monitoring glycemic control, BP and lipid profile are routinely assessed in patients with diabetes, with their treatment adjusted as needed to achieve better control of global vascular risk. However, monitoring inflammation and oxidative stress are not commonly performed in patients with T2DM in clinical practice.
In comparatively recent studies, CRP was suggested to be a marker of inflammation that may further help in predicting macrovascular complications and their clinical outcomes [Ridker et al. 1997, 2000, 2001; Tracy et al. 1997; Koenig et al. 1999; Danesh et al. 2000; Ridker, 2003]. Moreover, studies also indicated that hs-CRP is a stronger predictor of increased cardiovascular risk in patients with T2DM than more traditional LDL-C [Ridker et al. 2002]. It was also reported that hs-CRP did not correlate with LDL-C, and hence it was suggested to be used as an adjunct measurement to the lipid profile for better risk stratification [Albert et al. 2001; Ridker et al. 2002].
In spite of its proven strength in risk stratification of macrovascular complications, hs-CRP is not routinely measured in patients with T2DM or even periodically in Saudi Arabia. Our results show that mean hs-CRP level is not affected by management modality. Furthermore, the results validate earlier reports of the lack of correlation with serum cholesterol, but indicate a significant correlation with abdominal obesity, a major component of MS. This can be explained by the known relationship between general obesity and abdominal obesity in particular, and systemic inflammation [Fontana et al. 2007]. Moreover, and in spite of no significant correlation being found between HbA1c or BP and hs-CRP level, we found that the mean hs-CRP was higher and the proportion of high hs-CRP values (>3 mg/liter) was also increased in male patients with poor glycemic control compared with those with adequate control. In addition, a higher mean and a higher proportion of high hs-CRP values was found in hypertensive female patients compared with normotensive women. Therefore, in view of the strength of evidence for CRP as a risk predictor, its biochemical stability, and the standardization of the high sensitivity assay, it might be prudent to add it to the tests for monitoring patients with diabetes who are in need of additional improvement of their multimodal management.
Measurement of oxidative stress in clinical settings has its limitations. An important antioxidant defense in human tissues is the tripeptide reduced glutathione (GSH), with oxidative stress occurring when levels are inadequate. Lower levels of GSH in patients with diabetes were found to be associated with increased microvascular complications [Thornalley et al. 1996; De Mattia et al. 2008; Ahmadpoor et al. 2009]. However, the estimation of GSH status is not possible in a routine clinical setting and a more practical marker is needed. Previous studies have indicated that serum GGT can be used as an in vivo biomarker of GSH status due to its role in recycling GSH precursors in almost all tissues [Lee et al. 2004; Franco et al. 2007; Sedda et al. 2008]. However, and in spite of the accumulating evidence of its value as a risk predictor of vascular injury in metabolic disease [Jousilahti et al. 2000; Lee et al. 2003, 2006; Bidel et al. 2008; Mason et al. 2010; Bradley et al. 2014], GGT is still being used as a marker of alcohol consumption or liver disease almost exclusively. Our study shows that the use of different management modalities did not have an effect on mean GGT. However, we found a correlation between GGT level and dyslipidemia, and increased BP associated with MS, which supports earlier reports [Lee et al. 2003; Mason et al. 2010; Bradley et al. 2014]. In addition, our study found increased mean in patients with poor glycemic control, as well as abdominally obese (men and women), hypertensive (women), dyslipidemic (men) patients with diabetes, affirming further its strong connection with factors that increase oxidative stress (hyperglycemia, abdominal obesity, dyslipidemia, and high BP), and hence promote vascular complications. Indeed, we may suggest that the addition of GGT determination to the tests requested routinely for patients with diabetes would help in early detection of risk of vascular complications and help in improving management of such patients.
In conclusion, our study indicates that serum GGT and hs-CRP levels do not appear to be related to management regimen in patients with T2DM in Saudi Arabia. However, poor glycemic control, dyslipidemia, hypertension, and abdominal obesity are associated with higher mean GGT. Serum GGT correlates directly with triglycerides and diastolic BP, but inversely with HDL-C, all known components of MS. However, serum hs-CRP correlates with waist circumference only, with a higher mean being found in male patients with poor glycemic control and in hypertensive female patients. Due to the reported value of serum GGT [Lee et al. 2003; Mason et al. 2010; Bradley et al. 2014], and hs-CRP [Ridker et al. 1997, 2000, 2001; Tracy et al. 1997; Koenig et al. 1999; Danesh et al. 2000; Ridker, 2003] as risk predictors of vascular injury, it might prudent to include them in routine monitoring of patients with diabetes. Further studies are needed to understand how these markers will ultimately lead to CVD risk prediction and how targeting these markers with conventional and contemporary measurements will lead to CVD risk reduction.
Footnotes
Acknowledgements
SMB carried out the study design, literature search, wrote the manuscript and supervised preparing the tables and data analysis. MA, KAS, A Alhozali and SB provided patient and file information. AB and AG performed all biochemical analysis, and AB also reviewed the manuscript. GA supervised statistical analysis and reviewed the manuscript. A Alghamdi performed statistical analysis and collected data from medical records. MA entered data and collected background information and data from medical records. JT contributed to the study design, reviewed the manuscript critically and offered his comments.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Deanship of Scientific Research at King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia under grant number 2-140-1434-HiCi as part of research activity conducted by the ‘Saudi Diabetes Research Group’.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.