
Abstract
Pneumothoraces may be due a variety of aetiologies. Here we present two different cases: one with a unilateral pneumothorax due an iatrogenic medical procedure and another of idiopathic spontaneous bilateral nature. Although both cases were initially managed conservatively, the latter case required surgical intervention. We also conduct a literature review of the aetiology and management of pneumothoraces.
Keywords
Introduction
Pneumothorax is defined as air in the pleural cavity and can be primary, secondary or traumatic in nature [Macduff et al. 2010]. Primary spontaneous pneumothorax is not associated with any underlying lung diseases and most commonly occurs in young patients. The incidence of primary spontaneous pneumothorax has been reported at 9 per 100,000, of which 1.3% of these cases can be bilateral [Melton et al. 1979]. Secondary pneumothorax is associated with underlying lung disorders such as chronic obstructive pulmonary disease, cystic fibrosis or interstitial lung diseases [Macduff et al. 2010]. Many specialists need to be aware of a rare possibility of pneumothorax complicating common procedures that may not necessarily be considered as a potential cause of an iatrogenic pneumothorax. In addition, awareness is required that rarely patients may present with bilateral pneumothoraces and that if this is not recognised the consequences may be catastrophic. Here we describe a rare case of pneumothorax following multiple trigger point injection (TPI), a common anaesthetic procedure, and another of bilateral pneumothoraces, as well as a review of the literature with regards to their pathology and management. Written informed consent was obtained from both patients.
Case 1
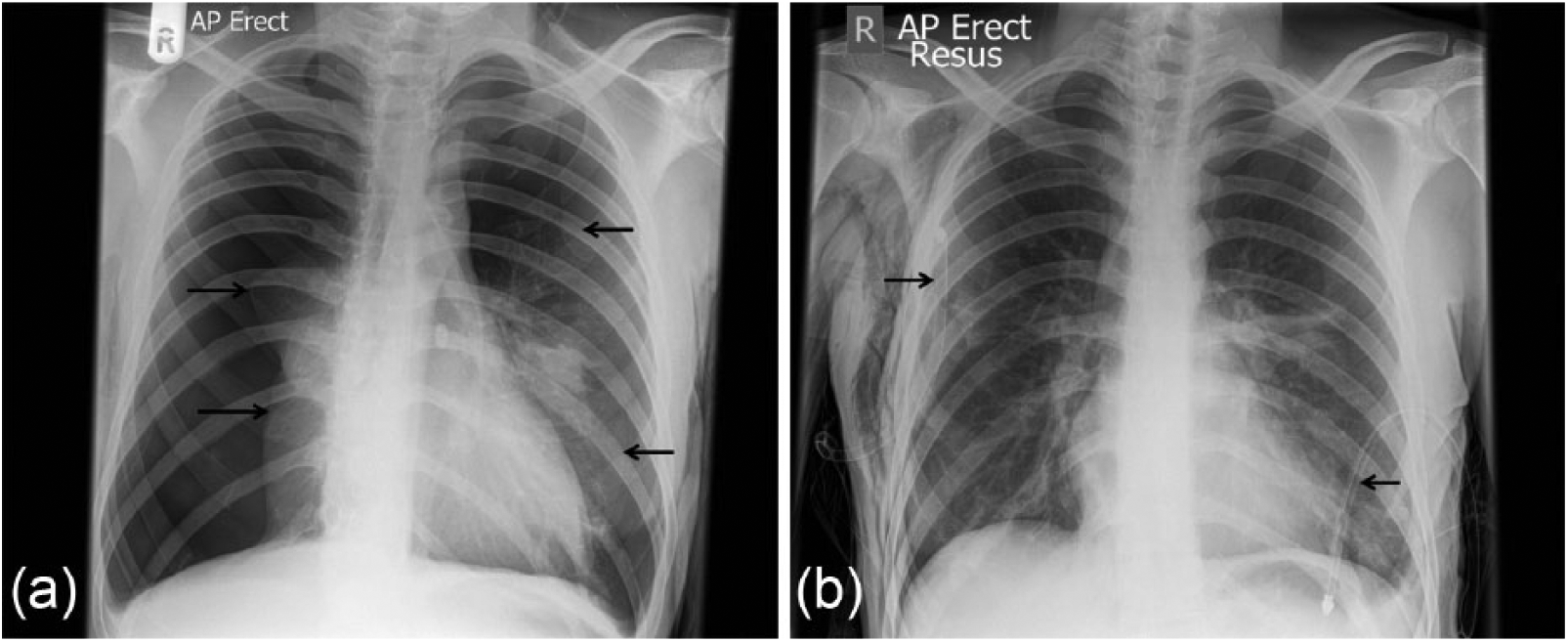
A 77-year-old woman with past medical history of asthma, hypertension, Paget’s disease and previous right breast cancer for which she had a mastectomy and radiotherapy was admitted with epigastric pain, progressive breathlessness and right-sided chest and neck pain. She had no prior history of pneumothorax, was a nonsmoker and had family history of note. Importantly, she had developed myofascial pain following her radiotherapy for which she underwent multiple TPIs to her back, neck and just below her right axilla (Figure 1). The needle size used was 21-guage [Yoon et al. 2009]. This admission was triggered 15 hours following the procedure. On examination, her oxygen saturation was 93% on room air and routine assessments being within normal limits, with a hyper-resonant percussion note and reduced air entry over the right hemithorax. A chest radiograph confirmed a large right-sided pneumothorax (Figure 2(a)). Consequently, an intercostal chest drain was inserted (Figure 2(b)) with good resolution within 36 hours, and the patient was discharged. At 6-week follow up she remained asymptomatic with normal chest radiograph.
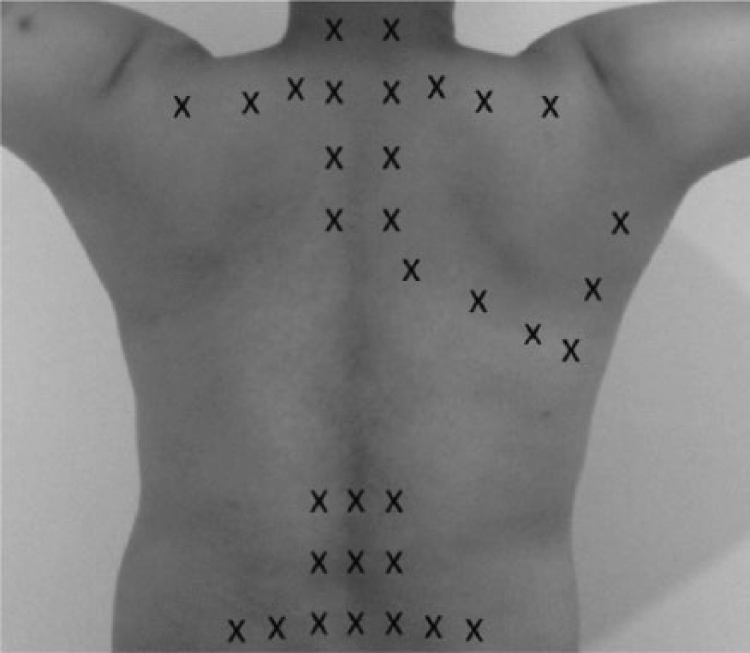
The torso showing the area covered and locations of the trigger point injections.

(a) Chest radiograph showing the unilateral pneumothorax. The arrow indicates the lung edge. (b) Chest radiograph with intercostal chest drain in the right hemithorax. The arrow indicate the position of the intercostal chest drain.
Case 2
A 22-year-old male never smoker with no previous medical conditions or relevant medical family history presented with sudden onset bilateral pleuritic chest pain. The chest radiograph revealed bilateral pneumothoraces (Figure 3(a)). He was apyrexial, with a heart rate of 84 beats/min, blood pressure of 130/80 mmHg, respiratory rate of 24/min and oxygen saturation of 94% on room air. The initial treatment involved insertion of bilateral intercostal chest drains (Figure 3(b)). Although both lungs re-inflated, there remained persistent air leaks; hence the patient underwent bilateral video-assisted thoracotomy surgery (VATS) and pleurectomy. There were no post-operative complications and at 4-week follow up the patient remained well with a normal chest radiograph and was back to his usual premorbid state.
(a) Chest radiograph with bilateral pneumothoraces at presentation. Arrows point towards the lungs edge. (b) Chest radiograph following bilateral intercostal chest drains insertion. The arrows indicate the position of the intercostal chest drains.
Discussion
Pneumothorax is a common medical emergency therefore many specialists need to be aware of its less common presentations. Iatrogenic pneumothorax can occur following a number of invasive medical or surgical procedures, however, it is not well recognised that some anaesthetic procedures such as TPIs may also be complicated by pneumothoraces. Trigger points are small, discrete, highly sensitive areas in taut muscles. Compression of these points produces pain locally and in a referred pattern [Fitzgibbon et al. 2004]. Despite controversy over efficacy, direct needling of trigger points with or without local anaesthetic and added steroid has been reported to be an effective treatment option in pain management [Simons et al. 1999]. However, this may be associated with complications including pneumothorax, epidural abscess, and muscle atrophy at the injection site [Scott et al. 2009]. In our case the most likely cause of pneumothorax was the TPI administered below the right axilla. Initially the pain (atypical for pneumothorax) was attributed to a possible gastroesophageal reflux disease. TPI in the cervicothoracic musculature as evidenced by our case can occasionally be associated with pneumothorax. For this reason in order to reduce the risk of pneumothorax electromyography and ultrasound-guided TPI in the cervicothoracic musculature have been advocated [Botwin and Patel, 2007; Botwin et al. 2008]. Delayed pneumothoraces have been described in the literature following procedures in or in close proximity to the thorax [Levy et al. 1986; Spiliotis et al. 1992; Traill and Gleeson, 1997]. Therefore, patients undergoing this procedure should routinely receive advice regarding recognition of symptoms suggestive of pneumothorax and need for an urgent chest radiograph.
Bilateral pneumothoraces are rare and represent approximately 1% of all pneumothorax cases; global literature describes just over 60 cases [Sayar et al. 2004]. It has been described in patients undergoing medical or surgical procedures or in patients with underlying lung disorders including silicosis, interstitial lung diseases, lung metastases, histiocytosis X, lymphangiomyomatosis, chronic obstructive pulmonary disease, occupational asthma or genetic disorders such as Birt–Hogg–Dube syndrome or in patients with HIV/AIDS infection [Graf-Deuel et al. 1994; Toro et al. 2007; Williams-Johnson et al. 2008; Khan et al. 2013; Corega et al. 2014]. A recent report described 12 cases of bilateral spontaneous pneumothorax all of which were treated with chest drain insertion and over half of which require surgical thoracotomy and pleurectomy [Sayar et al. 2004]. The British Thoracic Society recommends that patients presenting with simultaneous bilateral spontaneous pneumothoraces (SBSPs) should proceed to immediate chest drain insertion [Macduff et al. 2010]. Using only conservative management with chest drains has been reported to be effective and adequate in a number of patients, however a proportion would require surgical intervention, especially patients with underlying lung disease [Graf-Deuel et al. 1994; Garrido and Aguilera, 2002; Sayar et al. 2004]. Surgery is also advised if conventional management fails, i.e. if there remains persistent air leak and/or haemodynamic instability [Saadi et al. 1963; Graf-Deuel et al. 1994; Garrido and Aguilera, 2002; Sayar et al. 2004]. Bilateral VATS has shown to be safe in the treatment of SBSP [Ayed, 2002], however thoracotomy and pleurectomy have been preferred in haemodynamically unstable patients [Sayar et al. 2004]. Surgical intervention is viewed as a definitive option hence avoiding it in the future although there have been rare reports of recurrence of unilateral pneumothoraces post-surgically for bilateral pneumothoraces [Khan et al. 2013].
The underlying aetiology of pneumothoraces is not fully understood. There is evidence that a pneumothorax may occur as a result of the rupture of peripheral blebs or bullae [Haynes and Baumann, 2011; Grundy et al. 2012]. Other commonly described abnormalities that occur in patients with pneumothoraces include emphysema-like changes. More recent reports describe the presence of pleural inflammation and porosity in areas of inflammation on the visceral pleura most likely due to mesothelial cells being replaced by inflammatory cells [Haynes and Baumann, 2011; Grundy et al. 2012]. However, what is not known is how primary pneumothorax are precipitated. There is evidence that some activities such as playing air instruments could precipitate a pneumothorax. Other causes such as trauma or iatrogenic are clearly explained. Thus, in our first case an iatrogenic pain controlling procedure resulted in a pneumothorax. In the case of bilateral pneumothorax the mechanism remains a matter of speculation but may be related to an underlying aetiological processes such as inflammation and/or subpleural emphysema-like changes. The first, second and third recurrence episodes of primary spontaneous pneumothoraces has been suggested to be 54.2%, 62% and 83%, respectively [Gobbel et al. 1963; Sadikot et al. 1997].
The management of pneumothoraces depends on the patients’ symptoms and its size, and may vary from simple observation, aspiration, intercostal chest drain insertion or surgery [Baumann et al. 2001; Macduff et al. 2010]. Both our patients were treated initially with insertion of an intercostal chest drain. International guidelines differ slightly in their recommendations. The British Thoracic Society (BTS) guidelines recommend that an intercostal chest drain is inserted for a large over 2 cm in size primary spontaneous pneumothorax and for a secondary pneumothorax [Macduff et al. 2010]. The American College of Chest Physicians (ACCP) guidelines define a large pneumothorax as ≥3 cm apex-to-cupola distance and favour insertion of intercostal chest drain over a simple aspiration in majority of the cases. In the case of the iatrogenic pneumothorax in our first patient this resulted in full lung expansion. In contrast our patient with bilateral pneumothoraces required surgery due to the presence of persistent air leakage. Surgical management including VATS is the most common surgery with resulting risks of recurrence of less than 3% [Chambers and Scarci, 2009]. Surgery should be considered in the recurrent ipsilateral, contralateral or bilateral simultaneous pneumothoraces [Baumann et al. 2001; Macduff et al. 2010]. Surgery would involve the resection of a bullous lesion, emphysematous pleural blebs and emphysema-like changes together with pleurodesis.
Pneumothoraces may occur following a number of procedures and in some cases are medical emergencies requiring urgent attention and management, especially when they occur bilaterally. Often in the acute situation drainage of the pneumothorax with an intercostal drain is pivotal, however in certain cases surgery may be essential. The cases we discuss here not only report iatrogenic and idiopathic causes of pneumothoraces, but also the conservative and invasive management strategies.
Footnotes
Conflict of interest statement
The authors have none to declare with respect to this case series.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.