
Abstract
Objective:
Determine the incidence of major diabetes risk factors over time in patients prescribed chronic statin therapy.
Methods:
Retrospective observational chart review of adult patients without diabetes in primary care who initiated statin therapy between 2005 and 2010. Presence of diabetes risk factors were determined 1 year prior to statin initiation and continued up to a maximum of 7 years. Diabetes risk factors included impaired fasting glucose, body mass index (BMI) ≥30 kg/m2, hemoglobin A1c >6% and metabolic syndrome. Descriptive statistics were used to describe the incidence of diabetes risk factors over time.
Results:
A total of 98 patients met study criteria; mean age was 57 ± 13 years, 43% were men and 71% self-identified as Caucasian/white. Mean baseline values were A1c of 5.97%, fasting glucose of 104 mg/dl and BMI of 28 kg/m2. There were zero diabetes risk factors over time in 54% ± 7% of patients. The incidence over time of 1 risk factor was 25 ± 9%, 2 risk factors was 17 ± 5% and 3 risk factors was 3 ± 2%. A total of 12 patients were diagnosed with type 2 diabetes during the course of the study period.
Conclusion:
The incidence of diabetes risk factors did not change over time in an ambulatory adult population prescribed chronic statin therapy. Larger population studies assessing the incidence of and change in diabetes risk factors in patients on chronic statin therapy may help assess the association between statin therapy and presence of such risk factors.
Keywords
Introduction
The use of statin (3-hydroxy-3-methylglutaryl coenzyme-A reductase inhibitor) therapy for the secondary prevention of cardiovascular disease (CVD) is well-established [Smith et al. 2011]. In the primary prevention population, data overall demonstrate benefits with a recent Cochrane Review indicating that statin therapy reduces all-cause mortality, major vascular events and revascularization [Taylor et al. 2013]. However, as new evidence has become available, an association between statin use and new-onset type 2 diabetes mellitus (T2D) has been demonstrated.
A meta-analysis of 13 large statin trials including both primary and secondary prevention populations showed a 9% increased relative risk for incident T2D [Sattar et al. 2010]. This risk was highest in trials with older patients, but did not correlate with body mass index (BMI) or low density lipoprotein cholesterol (LDL-C). Data from the Women’s Health Initiative indicated there was a 48% increased risk of T2D among postmenopausal women taking a statin [Culver et al. 2012]. In this analysis, women with a lower BMI were at increased risk compared with women with a BMI of 25 kg/m2 or more. Data also suggest that a higher risk of new-onset T2D is related to the potency of the statin. A meta-analysis of 5 statin trials comparing intensive-dose statin therapy (atorvastatin 80 mg or simvastatin 40–80 mg) to moderate-dose statin therapy (simvastatin 20–40 mg, pravastatin 40 mg, or atorvastatin 10 mg) revealed a 12% increased relative risk of incident T2D in patients who were taking intensive-dose statin therapy [Preiss et al. 2011]. When compared with pravastatin, the authors of a population-based cohort study found a 10–22% increased relative risk of incident T2D in patients taking atorvastatin, rosuvastatin and simvastatin, but not with fluvastatin or lovastatin. These findings were similar among primary and secondary prevention patients [Carter et al. 2013].
The Justification of the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) trial, the largest prospective, randomized, placebo-controlled trial evaluating statin use in the primary prevention population to date, provided the most patient data regarding risk of incident T2D with statin therapy. JUPITER demonstrated an increased risk of physician-reported incident T2D with statin use (3.0% versus 2.4%, p = 0.01) [Ridker et al. 2008]. A preplanned secondary analysis of JUPITER was performed in which patients were stratified based on the presence of zero or one or more major diabetes risk factors [Ridker et al. 2012]. Risk factors included: metabolic syndrome [defined according to the American Heart Association (AHA) and National Heart, Lung, and Blood Institute (NHLBI) 2005 consensus criteria] (Grundy et al. 2005), impaired fasting glucose (IFG) (100–125 mg/dl), BMI ≥30 kg/m2 and hemoglobin A1c >6%. Patients with one or more major T2D risk factors had a 28% increased relative risk of in incident T2D [hazard ratio 1.28, 95% confidence interval (CI) 1.07–1.54, p = 0.01] whereas those with zero risk factors had no increase in the development of T2D. These data suggest the risk of incident T2D may be related to the presence of at least one major T2D risk factors.
Despite evidence suggesting a link between statin use and incidence of T2D, very little is known regarding the development and perpetuity of T2D risk factors over time in patients on chronic statin therapy. Furthermore, even less is known about these risk factors in clinical practice when patients are utilizing all commercially available statins for either primary or secondary prevention. It is unknown if the incidence of these risk factors is constant or changes during the course of statin therapy. This retrospective study was designed to describe the incidence of major risk factors for T2D over time in patients prescribed chronic statin therapy.
Materials and methods
Study design
This was a retrospective observational chart review to assess the incidence of diabetes risk factors with chronic statin use in patients without a diagnosis of diabetes at baseline. The study was approved by the Colorado Multiple Institutional Review Board (COMIRB) and the Hospital Research Review Committee (HRRC) for the University of Colorado Hospital (UCH). The definitions of diabetes risk factors are listed in Table 1 [Grundy et al. 2005]. A modified definition of the metabolic syndrome that included the criterion of BMI ≥30 kg/m2 was utilized because waist circumference is neither regularly measured nor reported in our electronic medical record (EMR). Patients were required to have two IFG values not associated with an acute hospitalization to qualify for the IFG risk factor. Patients were required to have only one IFG value to qualify as a criterion for the metabolic syndrome. Once the date of statin initiation was determined, risk factor data were gathered for a time period of 1 year prior to statin initiation and continued through the end of the study period, or as available data permitted. Descriptive statistics were used to describe the incidence of risk factors over time.
Diabetes risk factors.
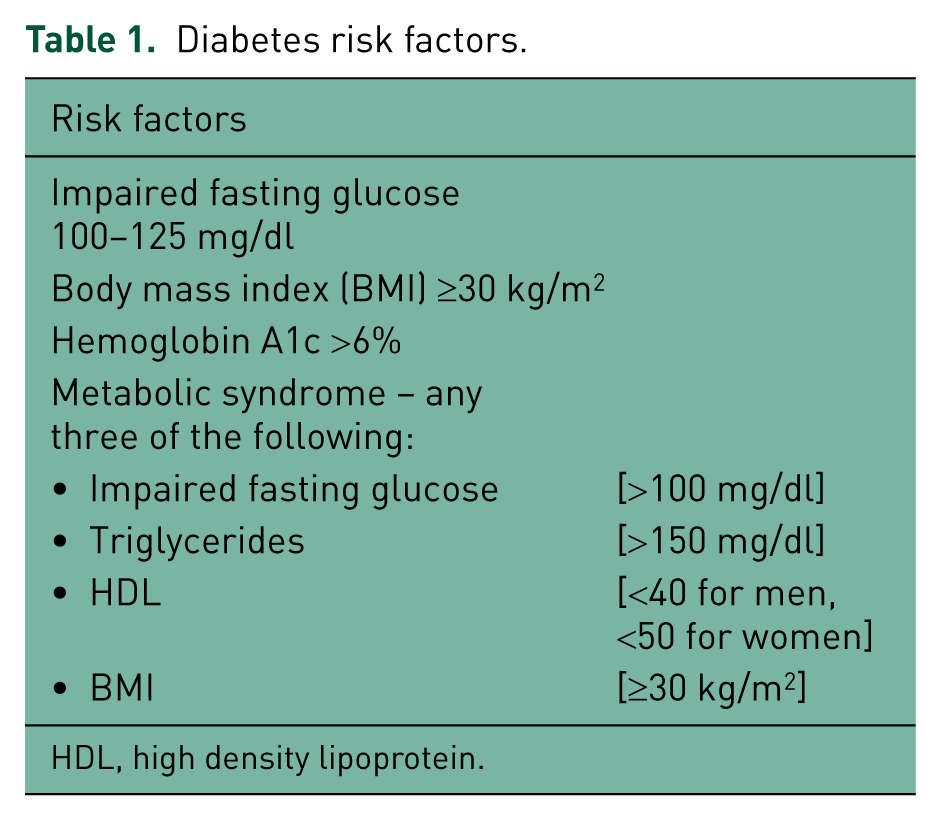
HDL, high density lipoprotein.
Patient population
Inclusion criteria were age between 18 and 89 years, care provided at a UCH primary care clinic, and initiation of statin therapy between 1 January 2005 and 31 December 2010. All commercially available statins at all available doses were evaluated. Patients were excluded if they had an A1c ≥6.5% or a diagnosis of T2D in the year preceding statin therapy initiation, or if they did not continue statin therapy for at least 2 years. Plasma glucose values were not used as a diagnostic criterion for T2D. For patients who developed T2D after initiation of statin therapy, risk factors were not included in the overall analysis from that point forward; however, patient data until that time were included.
Results
A total of 2600 patients were identified with a representative sample of 1687 randomly selected for review of their EMR; 98 patients met study criteria. The primary reason for exclusion was an inability to establish the start date of statin therapy (n = 890), followed by the patient having less than two years of follow-up (n = 562). Other reasons for exclusion were presence of diabetes at baseline (n = 132), invalid medical record number (n = 4) and age > 89 years (n = 1). Three patients did not have prebaseline data, but written documentation in the EMR confirmed statin initiation. None of these three patients were diagnosed with diabetes during the study period.
Baseline demographics of the cohort of 98 patients included are listed in Table 2; the average age was 57 ± 13 years old, 43% were male and 71% self-identified as Caucasian/white. Baseline risk factor values are also listed in Table 2. Primary prevention patients made up 71% of the cohort. Simvastatin was the most commonly prescribed statin at baseline (55%), followed by atorvastatin (34%) pravastatin (7%), lovastatin (3%) and rosuvastatin (1%). No patients were prescribed fluvastatin or pitavastatin at baseline.
Baseline demographics.

BMI, body mass index.
At year 1, 47% of patients (n = 46) had zero risk factors, 30% (n = 29) had one risk factor, 14% (n = 14) had two risk factors, and 6% (n = 6) had 3 risk factors. More than half (54 ± 7%) of patients neither had nor developed T2D risk factors over time. Approximately 25% of patients had 1 risk factor, 17% had 2 risk factors and only 3% had 3 risk factors over time (Table 3 and Figure 1).
Incidence of diabetes risk factors.


Incidence of diabetes risk factors.
Two metabolic syndrome criteria, high-density lipoprotein cholesterol (HDL-C) and triglyceride (TG) levels, improved over time after initiation of statin therapy. However, the incidence of the other diabetes risk factors – A1c, plasma glucose, BMI and categorization of metabolic syndrome – did not change over time. A total of 12 patients were diagnosed with T2D, either by diagnostic laboratory criteria (A1c) or as designated in their EMR; 3 patients were diagnosed with T2D at year 1, 2 patients at year 2, 4 patients at year 3 and 3 patients at year 4. Baseline demographics of this subpopulation were similar to the larger cohort, although the mean age was slightly younger (53 years old). The mean number of risk factors at baseline was 0.92 ± 0.95 which is slightly higher than the number of baseline risk factors for the entire population (0.66 ± 0.87). Notably, 5 of the 12 patients had zero risk factors in the year(s) preceding their T2D diagnosis. Of the remaining patients who were diagnosed with T2D, each met criteria for the metabolic syndrome for at least one time point prior to T2D diagnosis.
Discussion
In this retrospective study of a real world population prescribed chronic statin therapy, the incidence of T2D risk factors did not change over time. Although the number of patients with available data decreased over time, the relative incidence of risk factors remained constant. For example, a patient with only one major risk factor for T2D at the time of starting statin therapy continued to only have one risk factor 6 years later while still being prescribed statin therapy. Two individual components of the metabolic syndrome (HDL-C and TG), which is a major risk factor for T2D, improved over time with statin therapy. While this is expected with statin therapy, the overall incidence of having metabolic syndrome as a T2D risk factor did not change with time. Similarly, the incidence of the other individual major risk factors for T2D did not change over time. This should be reassuring to clinicians who assess baseline risk for T2D prior to starting statin therapy because of the association between statin use and incident T2D.
Despite a large number of unavailable case records in the last 2 years, 8 years of data for our cohort revealed that the overall incidence of T2D risk factors did not change with time, yet 12% of our patients were ultimately diagnosed with T2D. Moving forward, clinicians will be faced with the challenge of weighing risks versus benefits when considering statin therapy. Clinicians may risk stratify patients based on the presence or absence of major T2D risk factors. The current study suggests that, in our population, these risk factors did not change over time. As a result, it may be more prudent to consider the clinical benefit the patient would receive versus untoward side effects, which, as discussed below, are minimal.
Multiple clinical trials and meta-analyses have demonstrated an association between statin use and incident T2D [Sattar et al. 2010; Culver et al. 2012; Preiss et al. 2011; Carter et al. 2013; Ridker et al. 2008]. However, the mechanism explaining why statin therapy is associated with the development of diabetes is unknown. Similarly, the exact magnitude of this association is also unclear, but an association does exist. In response to these data, the US Food and Drug Administration revised the labels of all statins in 2012 to include warnings for increased plasma glucose and increased A1c [US FDA, 2013]. In the largest meta-analysis of 246,955 patients, statins were not associated with higher rates of myalgias, creatinine kinase elevations, cancer or higher rates of discontinuation because of adverse events when compared to placebo [Naci et al. 2013]. Statins were, however, associated with higher rates of incident T2D (odds ratio 1.09, 95% CI 1.02–1.16).
Despite the association between statin use and incident T2D, statin therapy remains an effective therapy to reduce the risk of cardiovascular (CV) events in patients with diabetes and those at risk for T2D. The American Diabetes Association (ADA) continues to recommend that all patients with T2D receive statin therapy [American Diabetes Association, 2013]. In the 2013 ADA Standards of Medical Care, statin therapy is strongly recommended in patients who have overt CVD, do not have CVD but are over the age of 40 years and one or more other risk factor for CVD, or for lower risk patients whose LDL-C remains above 100 mg/dl [American Diabetes Association, 2013]. In the JUPITER subgroup analyses of patients without diabetes (but with either obesity or metabolic syndrome), patients on statin therapy experienced fewer CV events than those on placebo [Ridker et al. 2008]. Statins have proven benefits in both primary and secondary prevention and will continue to be extensively used [Smith et al. 2011; Taylor et al. 2013]. Future statin therapy may be further intensified as an evaluation of the National Health and Nutrition Examination Surveys from 2005 to 2010 revealed that 54.6% of hypertensive patients were not controlled to their Adult Treatment Panel (ATP) III recommended goal, including only 8.1% among those being treated for dyslipidemia [Egan et al. 2013].
The current study is not without limitations. First, the retrospective nature limited the number of patients and the timeframe over which they were studied due to missing data points. Second, multiple assumptions had to be made for data collection purposes. Laboratory values in the EMR do not often document whether they were fasting. The majority of laboratory values reported are designated as ‘random’ and include the time they were collected. All laboratory values collected before 12:00 for plasma glucose were assumed to have been fasting. All lipid panels were assumed to have been fasting regardless of the time they were drawn. Plasma glucose values obtained while patients were hospitalized for an acute illness (e.g. sepsis) or surgery (e.g. solid organ transplantation) were not evaluated for the IFG risk factor due to confounding influences on the plasma glucose values in this setting. Plasma glucose values often increase in a physiologic response to stress, such as that associated with an acute hospitalization. Furthermore, patients were frequently receiving glucocorticoid therapy during this time, which could also acutely increase plasma glucose values. Our EMR neither prompts for waist circumference nor designates a field to enter the value if it is measured, so waist circumference is rarely measured or documented. Because of this, BMI was used as a surrogate marker for waist circumference as a criterion for the metabolic syndrome. Given these assumptions, it is possible that the number of risk factors was overestimated due to an increased incidence of IFG, elevated TG, or patients meeting criteria for metabolic syndrome. It should be noted, however, that none of the 12 cases of diabetes were diagnosed using IFG. Third, the only statin information that was consistently documented in the chart was initial statin therapy. Inconsistent documentation of changes to either statin drug or dose as well as start and stop dates inhibited the ability to track these data. Finally, the entire population of 2600 subjects was not evaluated due to the selection of a representative sample of 1687 patients within that population. Of those 1687, only 6% met study criteria. While approximately 900 patients remain available for analysis, an additional 6% of those patients would only yield another 54 patients for analysis. A larger health system or database would be necessary to yield a more robust sample size, although we feel that our sample is representative of the total population in our health system.
Conclusion
Our study of an ambulatory, ‘real world’ adult population without diabetes taking chronic statin therapy demonstrated that T2D risk factors were consistent over time that patients were prescribed statin therapy. Based on our data, clinicians can use baseline risk of T2D in patients who start statin therapy to aid in the risk stratification of patients and can assume that this risk remains consistent. Larger prospective and population-based studies would be helpful to confirm our observation and to further elucidate any potential relationship between statin therapy, presence of T2D risk factors and incidence of T2D.
Footnotes
Acknowledgements
During the time this project was conducted, W.M.K. IV was a PGY2 Ambulatory Care/Family Medicine Pharmacy Resident at the University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences and University of Colorado Hospital. The authors wish to acknowledge Jim R. Bateman, Epic Technical Team Report Writer at the University of Colorado Hospital for his assistance with assembling data reports.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.