
Abstract
Small intestinal bacterial overgrowth (SIBO) is defined as the presence of an abnormally high number of coliform bacteria in the small bowel. It is associated with a broad range of predisposing small intestinal motility disorders and with surgical procedures that result in bowel stasis. The most common symptoms associated with SIBO include diarrhea, flatulence, abdominal pain and bloating. Quantitative culture of small bowel contents and a variety of indirect tests have been used over the years in an attempt to facilitate the diagnosis of SIBO. The indirect tests include breath tests and biochemical tests based on bacterial metabolism of a variety of substrates. Unfortunately, there is no single valid test for SIBO, and the accuracy of all current tests remains limited due to the failure of culture to be a gold standard and the lack of standardization of the normal bowel flora in the small intestine. Currently, the ideal approach to treat SIBO is to treat the underlying disease, eradicate overgrowth, and address nutritional deficiencies that may be associated with the development of SIBO.
Introduction
Small intestinal bacterial overgrowth (SIBO) is a heterogeneous syndrome characterized by an increased number and/or abnormal type of bacteria in the small bowel. While some consider culture of the small bowel the gold standard for the diagnosis of SIBO based on the presence of ≥1 × 105 bacteria [i.e. colony-forming units (cfu)] per ml of proximal jejunal aspiration, this designation was arbitrary and now the value has begun to be questioned by consensus and review of the literature [Gasbarrini et al. 2007; Khoshini et al. 2008]. Khoshini and colleagues suggest normal subjects rarely exceed 1 × 103cfu/ml and that this should be the defining threshold for SIBO [Khoshini et al. 2008].
Historically, the definition of SIBO is based on bacterial overgrowth in the context of abnormal or postsurgical anatomy. The characteristic situation where SIBO was most considered was in the stagnant loop syndrome. It is in this literature that investigators established the culture definition for bacterial overgrowth and the source of >1 × 105 cfu/ml criteria for SIBO. However, over the past three decades, there has been increasing suspicion of a bacterial overgrowth-like entity in many other nonsurgical gastrointestinal diseases. This has led scientists to question whether the definition of >1 × 105 cfu/ml (as defined by stagnant loop) can be used for other conditions. A systematic review conducted Khoshini and colleagues suggests that many gastrointestinal conditions have increased bacterial counts compared with healthy controls in the small bowel but below 1 × 105 cfu/ml. This leads to the suspicion that the definition of SIBO based on culture is more indicative of stagnant loop and not SIBO, and that perhaps a definition of ≥1 × 103 coliform bacteria cfu per ml of proximal jejunal aspiration as suggested by systematic review should be used as the definition of SIBO (Box 1).
Definition of small intestinal bacterial overgrowth (SIBO).
Finding of ≥1 × 103 coliform bacteria [i.e. colony-forming units (cfu)] per ml of proximal jejunal aspiration].
What is unique about SIBO is that there are excessive numbers of aerobic and anaerobic bacteria colonizing the small intestine, a region usually containing few bacterial populations [Toskes, 1993; Bouhnik et al. 1999; Bures et al. 2010]. The bacteria typically recognized as SIBO are mainly of the colonic type and are thus predominantly gram-negative aerobes and anaerobic species that ferment carbohydrates into gas [Posserud et al. 2007; Sachdev and Pimental, 2012]. Common bacteria found in SIBO include Escherichia coli, Enterococcus spp., Klebsiella pneumonia and Proteus mirabilis, among others [Savage, 1977; Bouhnik et al. 1999; Frank et al. 2007; Frissora and Cash, 2007]. The SIBO hypothesis proposes that it is this expansion of bacteria into the small intestine from the large intestine that leads to symptoms including bloating, abdominal discomfort and changes in stool form [Pimentel and Lezcano, 2007].
Causes of gastrointestinal bacterial overgrowth
Bacterial overgrowth occurs when intestinal stasis give the coliform bacteria the opportunity to proliferate locally. Mechanical stasis is an obvious cause of stasis in the gut and can be seen often in patients who have undergone previous gastrointestinal surgery. The classic of these is the surgical blind loop that allows for bacterial proliferation (see Table 1). Other prominent causes include diabetes, scleroderma, intestinal diverticulosis, afferent loop following a Billroth II gastrojenunostomy, and intestinal obstruction caused by strictures, adhesions, cancer and more recently irritable bowel syndrome (IBS). In addition, certain medications are associated with stasis and SIBO. For example, narcotics cause intestinal slowing and proton pump inhibitors (PPIs) reduce acid, which can lead to oral microbe penetration of the proximal gut [Lombardo et al. 2010; Compare et al. 2011; Hamvas, 2012].
Causes of small intestinal bacterial overgrowth.
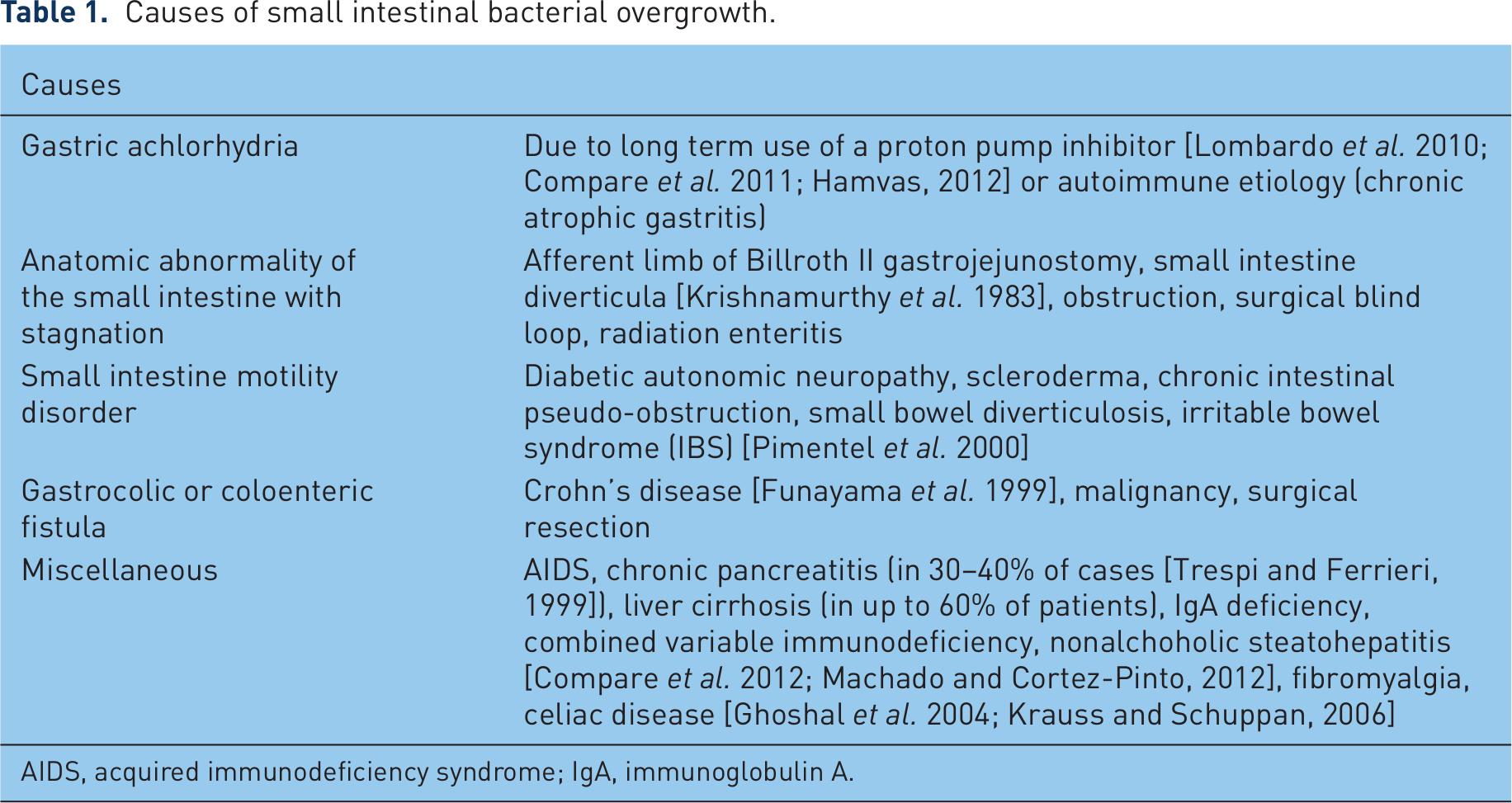
AIDS, acquired immunodeficiency syndrome; IgA, immunoglobulin A.
In evaluating the mechanism of diarrhea in bacterial overgrowth, it is essential to realize that it is multifactorial. Hypothetical mechanisms are the following:
Bacteria digest carbohydrates, producing gas and osmotically active byproducts that promote osmotic diarrhea.
Bacteria and fatty acid byproducts injure the mucosa and contribute to diarrhea.
Mucosal injuries create lactase deficiencies.
Bacterial deconjugation of bile salts interferes with fat absorption and the absorption of fat-soluble vitamins.
Most of these have not been determined by modern scientific method. However, the cause of SIBO also needs to be considered. For example, bowel obstruction or adhesions can cause bloating or distension in addition to SIBO.
Prevalence
The true prevalence of SIBO and its relationship to various disorders is largely unknown [Berlin, 1987] because of the difficulty in its detection and definition [Cole and Ziegler, 2007]. It is particularly difficult to define its true prevalence because there is an association between SIBO and a number of other disorders and symptoms often overlap [Quigley and Abu-Shanab, 2010; Ghoshal et al. 2003]. Some patients may not seek healthcare and SIBO may not be properly diagnosed by medical investigations. Bacterial overgrowth may be asymptomatic or only present with nonspecific symptoms, and all symptoms might be incorrectly ascribed to the underlying disease (leading to SIBO) [Bouhnik et al. 1999]. In addition, the prevalence of SIBO is directly dependent on the characteristic of the study population and the diagnostic method used to detect or define bacterial overgrowth. If a breath test is used as the diagnostic method, prevalence varies further depending on the nature and dose of substrate used. In healthy people, SIBO has been described in 0–12.5% by the glucose breath test, 20–22% by the lactulose breath test and 0–35% by the 14C
Clinical manifestations
Although the symptoms of bacterial overgrowth are well known (Table 2), there are few studies that aim to scientifically characterize the symptoms. Since SIBO can be due to a number of local and systemic disorders, the symptoms of SIBO are distorted by symptoms of the underlying condition (scleroderma is a good example). The clinical manifestations of SIBO depend upon the severity of disease. While one would assume that the greater the quantity of bacteria, the greater the symptom, this has not been well studied. In Billroth II subjects, where coliform counts are ≥1 × 105cfu/ml these patients often develop significant malabsorption as well as the typical symptoms of bloating. It is not clear if the malabsorption is due to the nature of the surgery, the level of bacteria or other consequences. However, it is now believed that most patients with bacterial overgrowth do not have clinical malnutrition caused by malabsorption. In these cases the typical symptoms are nonspecific, and include distention, flatulence and diarrhea. Only rare instances (mostly associated with jejunoileal bypass surgery or short bowel syndrome) result in vitamin and mineral deficiencies, including the fat-soluble vitamins A or D, vitamin B12 and iron [Di Stefano et al. 2001].
Clinical manifestations of small intestinal bacterial overgrowth.

Recently, data are accumulating to suggest that the most common association with SIBO is IBS and bacterial overgrowth may be part of the pathogenesis of this condition [Pimentel et al. 2006; Fumi and Trexler, 2008]. In addition, SIBO has been reported with rosacea, a dermatological skin condition affecting the face [Parodi et al. 2008].
Diagnosis
There are many ways to diagnose SIBO but the diagnosis often starts with clinical suspicion and history of risk factors for SIBO (Table 3). Currently, there is no adequately validated diagnostic test for SIBO despite decades of its recognition as a clinical entity [Khoshini et al. 2008]. Physical examination and laboratory tests can be used, although findings are nonspecific. The gold standard used in diagnosis was quantitative culture of jejunal aspirates demonstrating >1 × 105 cfu/ml of fluid; however, this value is not validated and recently suggested to be more accurately assessed as >1 × 103 cfu/ml by systematic review [Khoshini et al. 2008].
Identification of small intestinal bacterial overgrowth (SIBO) in a patient.

CT, computerized tomography.
Breath testing, and specifically the hydrogen breath test, aid in the diagnosis. Noninvasive breath tests have been shown to have a sensitivity of 60–90% and specificity of 85%, although validation with culture is limited [Khoshini et al. 2008]. Stools studies can also be used to corroborate the presence of steatorrhea. In addition, small bowel barium radiography or computerized tomography (CT) enetrography can be used to identify mechanical factors predisposing to intestinal stasis.
Direct tests for SIBO
Measurement of the bacterial colony count
As described above, the most widely accepted test for SIBO is quantitative culture of luminal contents, and values >1 × 105 cfu/ml are traditionally felt to be abnormal. However, recent data support the argument that this value is too high and represents only the degree of SIBO found in surgically altered patients [Khoshini et al. 2008]. Based on normal human small bowel culture, the definition of SIBO appears more likely counts >103 cfu/ml.
During culture, the proper technique for collection of the specimen for the culture is not well defined. A sterile catheter passed through the instrument channel of an upper endoscope has the means of collecting a specimen free of contamination by saliva and other secretions. Culture techniques on the aspirated sample also vary. The sample is often plated on nonselective media.
There are concerns with culture as a standard as well. One major concern is the inability to gain access to more distal segments of the small bowel, as only the upper small bowel is accessible using standard techniques. The test is also expensive and some risk since it requires endoscopy or fluoroscopy to place the aspiration catheters. Other limitations of jejunal aspirates include the fact that very few of the gut bacteria can be identified or cultured since there are 400–500 species of bacteria in the bowel, and most of them cannot be routinely cultured [Quigley and Abu-Shanub, 2010], and contamination with oropharyngeal flora frequently occurs during collection of the specimen. In addition, the bacterial overgrowth may be patchy and missed by a single aspiration, or located in relatively inaccessible sites [Fan and Sellin, 2009]. Therefore, due to all of these limitations, cultures are not commonly performed.
Indirect tests for SIBO
Breath tests
Breath tests are now widely used as an alternative to direct aspiration because they are noninvasive and less expensive. Breath tests that are commonly used include the 14C
Hydrogen breath tests are based on the principle that carbohydrate fermentation by the gut flora, primarily anaerobic bacteria in the colon, is the only source of hydrogen in the body. When colonic bacteria colonize the small intestine, as in SIBO, fermentation of carbohydrates in the small intestine produces a large and premature amount of hydrogen gas. H2 produced in this manner diffuses into the systemic circulation and is excreted via the lungs in expelled air. Hydrogen breath tests are performed following a 12-hour overnight fast and consumption of a low fiber diet for 1 day. Patients are asked to exhale into a tube connected to a bag and H2 baseline values are obtained before intake of a fermentable substrate. The carbohydrate substrate (glucose, lactulose or xylose) is then administered orally and a sequential end-expiratory breath is taken every 15 minutes for 3 hours.
Owing to their low costs and relative simplicity, hydrogen breath tests are the most common of all the breath tests used to diagnose SIBO and of these, the lactulose hydrogen breath test (LHBT) is the most widely used hydrogen breath test. The increase in hydrogen level after lactulose ingestion was first reported by Bond and Levitt [Bond and Levitt, 1972]. In this case, intestinal flora ferment the lactulose, resulting in the production of hydrogen and/or methane. After the administration of 10 g of the lactulose, breath samples are taken at 15-minute intervals for 3 hours.
The criteria for a positive breath test are also problematic and not well validated. However, the most commonly used technique is to recognize a rise in hydrogen of greater than 20 parts per million (ppm) and a double peak on the breath hydrogen expiration graph. The first peak is caused by production of the gas due to the presence of bacterial overgrowth in the small bowel; the second results from the action of cecal flora on the lactulose. Most investigators accept that the first rise in H2 be within 90 minutes of lactulose ingestion. It is also important to note that since the breath tests are simpler to perform, they are a reasonable choice for screening and monitoring of therapy.
Other tests
A variety of other tests have also been used to diagnose SIBO. Imaging studies are useful for the identification of causative factors such as jejunal diverticulosis. Biopsies are usually not very effective because mucosal injury and villous atrophy are only present in the most severely affected individuals [Quigley and Abu-Shanub, 2010]. Urinary choly p-aminobenzoic acid (choly-PABA) and indican can also be used to detect SIBO [Khoshini et al. 2008]. Various serum makers such as bile acids, folic acid and cobalamin have also been proposed, but none have the diagnostic accuracy necessary for use in the diagnosis of SIBO [Quigley and Abu-Shanub, 2010].
Treatment
Treatment for SIBO is complex and must be individualized. The three main components in treating patients with SIBO are shown in Box 2.
Principles of treating small intestinal bacterial overgrowth (SIBO) [Quigley and Abu-Shanub, 2010].
Treat the underlying disease or condition.
Eradicate overgrowth
Address associated nutritional deficiencies.
It is important to address all causes, symptoms and complications associated with SIBO. Where physical causes are responsible, the best way to treat bacterial overgrowth is to correct the anatomic defect that has potentiated the overgrowth (e.g. adhesions, bowel obstruction, strictures). In other cases, treatment for bacterial overgrowth includes eliminating drugs that reduce intestinal motility or reduce gastric acidity. Dietary manipulation may also assist in the treatment of SIBO [Vanderhoof et al. 1998]. In many patients, it is necessary to exclude lactose from the diet, to reduce other simple sugars, to increase coverage of energy needs by fat and to administer medium-chain triacylglycerol (MCT) oils [Bures et al. 2010]. In cases where there is decreased motility, such as chronic pseudo-obstruction, methods to enhance motility can be attempted. Prokinetic agents that are commonly used and are available in the US include metoclopramide and erythromycin. In Europe, this could include prucalopride although this has not specifically studied in SIBO [Parodi et al. 2008]. In situations where a PPI is a suspected contributor to bacterial overgrowth, lifestyle measures for treatment of gastroesophageal reflux disease (GERD) or a reduction in acid suppression to the lowest possible dose for and shortest duration may be beneficial in alleviating symptoms of overgrowth.
Despite efforts to treat the primary cause of SIBO above, most patients require treatment with antibiotics. Antibiotic treatment should selectively target those bacterial strains that cause SIBO. The goal of treatment with antibiotics is to reduce rather than eradicate the flora, leading to symptomatic improvement. Ideally, the choice of antibiotics could be based on bacterial sensitivity testing to particular antibiotics [Singh and Toskes, 2004]. However, this would require culture in a large number of subjects and the limitation of culture as already discussed [Quigley and Abu-Shanub, 2010].
There is no common agreement concerning the choice, dosing and duration of antibiotic therapy. Broad spectrum antibiotics which affect enteric aerobes and anaerobes and numerous choices are available (Box 3). These include ciprofloxacin, norfloxacin, amoxicillin/clavulanate, metronidazole, cephalexin and more recently rifaximin. Rifaximin has gained popularity since it is nonabsorbed, has few side effects and little evidence for resistance [Frissora and Cash, 2007; Koo and Dupont, 2010]. Rifaximin may therefore be the antibiotic of choice as clinical resistance is seen far less frequent than with other antibiotics [Vanderhoof et al. 1998; Yang et al. 2008; Rabenstein et al. 2011; Di Stefano et al. 2000].
Antibiotic treatment options for small intestinal bacterial overgrowth (SIBO).
Rifaximin
Ciprofloxacin
Norfloxacin [Attar et al. 1999]
Amoxicillin/clavulanate [Attar et al. 1999]
Metronidazole + trimethoprin/sulfamethoxazole [Malik et al. 2011]
Metronidazole + cephalexin [Malik et al. 2011]
Regardless of the antibiotic used, the patient will need to be retreated and in some cases require long-term antibiotic use (e.g. widespread small intestinal diverticulosis). In more conventional cases, it is commonplace to repeat breath testing if symptoms of abdominal pain, diarrhea, bloating, and flatulence relapse [Lauritano et al. 2008]. There are no controlled trials to guide the duration of treatment or management of recurrent SIBO and recommendations are commonly based on clinical experience although successful treatment of recurrence with rifaximin has been reported [Pimentel et al. 2011].
Conclusion
SIBO is defined as an increase in the number of bacteria in the small bowel. While there are a number of different causes of SIBO, SIBO is often misdiagnosed or underdiagnosed due to the variety of clinical manifestations, and treatment must be individualized with a focus on eradicating the underlying disease. While antibiotics remain the mainstay of therapy, attention to understanding the mechanism of SIBO in any given patient is important to help implement a strategy to prevent relapse.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.