
Abstract
Advances in antiretroviral combination therapy lasting the past two decades have transformed HIV-1 infection from a fatal disease into a chronic medical condition that in many cases does not compromise life quality. There are 25 different antiretroviral agents available currently, allowing for patient-centered, individualized management of HIV-1 infection, and ongoing progress in HIV-1 virology and antiretroviral pharmacology is likely to expand treatment options further in the future. Nevertheless, antiretroviral therapy continues to have limitations, including insufficient immunological reconstitution, selection of drug resistance, ongoing abnormal immune activation despite effective suppression of HIV-1 viremia, and the inability to target latently infected cells that are responsible for long-term viral persistence. Owing to these shortcomings, the theoretical ability of antiretroviral therapy to extend life expectancy to normal levels is not realized in many cases. Strategies to address these limitations are a matter of active ongoing research and will be summarized in this article.
Keywords
Introduction
Antiretroviral therapy began more than 20 years ago when zidovudine (AZT) was licensed as the first pharmaceutical agent for treatment of HIV-1 infection. Subsequently, a total of 25 different anti-HIV-1 drugs from six different classes have become available, and the combined use of such agents as ‘highly active antiretroviral therapy’ (HAART) has dramatically reduced the morbidity and mortality associated with HIV-1 infection. In 1994–1995, HIV infection ranked as the leading cause of death among people aged 25–44 in the United States, with approximately 35% of all deaths in this age group being directly attributable to this disease. In contrast, fewer than 4% of deaths were related to HIV-1 infection in this age group in 2006. These advances have been made possible by a detailed understanding of HIV-1 virology and pathogenesis, by the massive investments made in HIV drug design and development and by the rapid evolution of treatment consortia able to conduct large-scale international clinical trials. Moreover, extensive collaborations among physicians, virologists, pharmacologists, HIV-1-infected patients, government institutions, pharmaceutical companies and patient advocacy groups have been critical to the advances in HIV-1 treatment, which today is highly effective, relatively safe and nontoxic, and in many cases easy and convenient to adhere to. Nevertheless, despite such progress, substantial challenges for the optimal care of HIV-1-infected persons remain. In this article, we briefly summarize current standards for HIV-1 treatment, and discuss ongoing research that might improve the clinical management of HIV-1-infected persons.
Current management of HIV-1 infection
Current antiretroviral therapy is based on the simultaneous administration of at least three antiretroviral drugs that target the viral replication cycle and suppress viral replication below the threshold of highly sensitive molecular detection techniques. At present, antiretroviral agents from six different classes are approved for the treatment of HIV-1 infection, and a detailed description of these pharmaceuticals and their clinical use is available in free online resources (e.g. http://www.aidsmap.com).
Nucleoside and nucleotide reverse transcriptase inhibitors
Nucleoside and nucleotide reverse transcriptase inhibitors (NRTIs) represent an integral component of all recommended first-line treatment regimens. These drugs inhibit reverse transcription of viral RNA into DNA by incorporating chemically modified nucleoside or nucleotide analogues into the viral DNA strand that terminate further DNA synthesis. The most widely used NRTIs in the US and other developed countries are emtricitabine and tenofovir, which are generally well tolerated and available as a coformulated pill for once-daily administration. An alternative NRTI preparation for once-daily dosing includes lamavudine and abacavir; however, this combination is less frequently used since abacavir can cause severe hypersensitivity reactions (particularly in HLA-B*5701 expressing individuals [Mallal et al. 2008; Saag et al. 2008]), and has been associated with an increased cardiovascular risk in some [Worm et al. 2010], but not all studies [Ribaudo et al. 2011]. Moreover, two studies have shown that when combined with efavirenz or ritonavir-boosted atazanavir, abacavir–lamavudine may be less effective than tenofovir–emtricitabine in patients with high (>100,000 copies/ml) baseline viral loads [Daar et al. 2010; Post et al. 2010].
Nonnucleoside reverse transcriptase inhibitors
Nonnucleoside reverse transcriptase inhibitors (NNRTIs) act as allosteric, noncompetitive inhibitors of the HIV-1 reverse transcriptase. Four NNRTIs are currently approved for HIV-1 treatment. Efavirenz, the most commonly used agent from this class, has a long half-life allowing for once-daily dosing, a relatively benign safety profile and a long record of superior performance in prospective clinical studies. Nevirapine, an alternative NNRTI, is less frequently used as a first-line agent in the US and Europe. Compared with efavirenz, nevirapine confers a higher risk of severe hypersensitivity reactions and may possibly be less potent [van Leth et al. 2004]. Delavirdine is now used infrequently because of its relatively inconvenient dosing regimen (three times daily) and inferior efficacy compared with other NNRTIs. The major advantage of etravirine, a second-generation NNRTI, is its activity against HIV-1 strains harboring typical escape mutations to efavirenz and nevirapine; it is therefore most commonly administered as part of a second-line or salvage regimen.
Protease inhibitors
Protease inhibitors target viral assembly by inhibiting the viral enzyme protease, which cleaves nascent viral proteins in functional subunits required for effective generation of new viral particles. The introduction of protease inhibitors in 1996 revolutionized antiretroviral therapy, despite problems with difficult dosing regimens, gastrointestinal side effects, and undesirable metabolic complications, including dyslipidemia and insulin resistance. Newer protease inhibitors have featured more convenient dosing regimens with improved safety and tolerability. These drugs, which are substrates of cytochrome P450-3A4, are usually administered with a low dose of the first-generation protease inhibitor, ritonavir (a potent inhibitor of P450-3A4 which is poorly tolerated at its full therapeutic dose) in order to improve their pharmacokinetic properties. ‘Ritonavir-boosted’ protease inhibitors are potent antiretroviral agents with high genetic (multiple mutations required) and pharmacokinetic (trough levels well above IC90) barriers to viral resistance. The most commonly used protease inhibitors for first-line therapy are lopinavir, atazanavir and darunavir. Lopinavir is coformulated with ritonavir and is the most commonly prescribed protease inhibitor worldwide. In high-income countries, lopinavir–ritonavir is gradually being replaced by atazanavir and darunavir (each ‘boosted’ by separately administered ritonavir), which are newer agents with fewer gastrointestinal and metabolic side effects. Darunavir and tipranavir (also given with ritonavir) both often retain activity against viruses which have accumulated mutations conferring resistance to older protease inhibitors, and therefore can be used in salvage regimens after virological failure.
Integrase inhibitors
Integrase inhibitors inhibit the integration of viral DNA into chromosomal host DNA. Raltegravir, a potent agent with apparently low toxicity, is the only currently approved drug from this class. It is administered twice daily, has few interactions with alternative medications and is recommended as a first-line treatment modality. It is also a valuable therapeutic option for treatment-experienced patients with multiclass resistant virus when given with at least one and preferably two other active agents [Yazdanpanah et al. 2009]; however, when given only with NRTIs in treatment-experienced patients, virologic failure is more common with raltegravir than with a boosted protease inhibitor [Eron et al. 2010].
Entry and fusion inhibitors
The group of entry and fusion inhibitors includes maraviroc, a selective inhibitor of the chemokine receptor CCR5 that blocks coreceptor-mediated entry of CCR5-utilizing viruses into host cells. This agent has no activity against CXCR4-tropic viral strains, and therefore generally requires a viral tropism test before being administered for treatment. Enfuvirtide, a biomimetic peptide, can block viral uptake by binding to the gp41 envelope structure and preventing fusion of the viral envelope with the host cell membrane. This is the only approved antiretroviral agent that has no oral bioavailability and must be administered subcutaneously twice a day. It is typically used in patients with multiresistant viruses and limited treatment options.
Initiating therapy and drug selection
Recommended first-line antiretroviral treatment options.
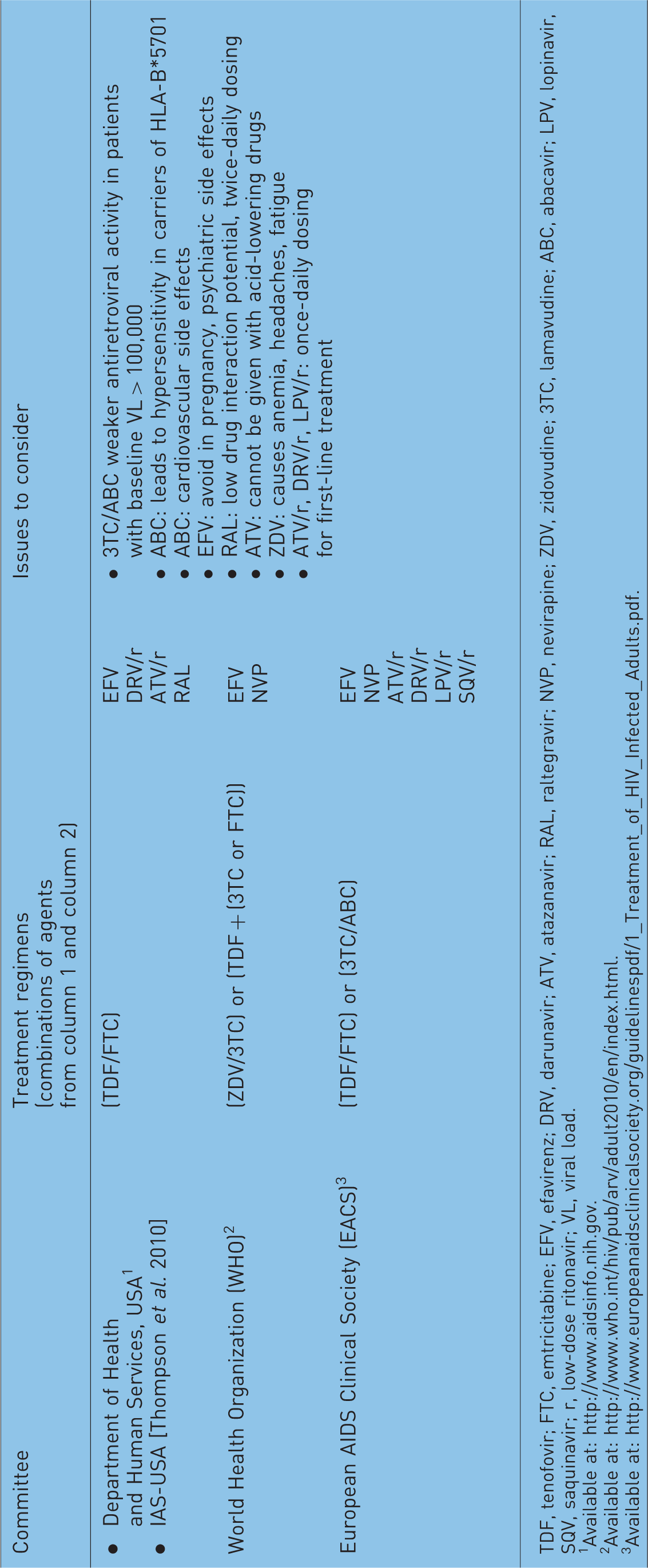
TDF, tenofovir; FTC, emtricitabine; EFV, efavirenz; DRV, darunavir; ATV, atazanavir; RAL, raltegravir; NVP, nevirapine; ZDV, zidovudine; 3TC, lamavudine; ABC, abacavir; LPV, lopinavir, SQV, saquinavir; r, low-dose ritonavir; VL, viral load.
Available at: http://www.aidsinfo.nih.gov.
Available at: http://www.who.int/hiv/pub/arv/adult2010/en/index.html.
Recommendations for initiation of antiretroviral therapy.

Available at: http://www.aidsinfo.nih.gov.
Available at: http://www.europeanaidsclinicalsociety.org/guidelinespdf/1_Treatment_of_HIV_Infected_Adults.pdf.
Available at: http://www.who.int/hiv/pub/arv/adult2010/en/index.html.
With currently recommended first-line antiretroviral regimens, more than 75% of treated patients are able to achieve the primary objective of antiretroviral therapy, a durable suppression of HIV viremia. A failure to reach this goal is in most cases attributable to one of the following reasons: (i) medication nonadherence, (ii) medication toxicity that prevents continuation of a selected regimen, and (iii) viral resistance mutations, the presence of which can be detected by genotypic or phenotypic resistance testing. The availability of antiretroviral drugs from six different classes allows in many cases to design an antiretroviral regimen that is still active in these situations, and can durably suppress viral replication. Typically, such salvage regimens include at least three antiretroviral agents that, based on resistance analysis, are expected to be active against the majority of circulating viral variants.
Limitations of current antiretroviral therapy
Although treatment with modern HAART in high-income societies may extend the life expectancy of HIV-1 infected persons to levels seen in the general population [van Sighem et al. 2010], a number of recent studies have shown that this is not generally the case [Bhaskaran et al. 2008; Hogg et al. 2008]. For instance, a large observation study involving more than 3000 HIV-1 patients and a background population of >300,000 HIV-1-negative persons in Denmark demonstrated that the life expectancy of HAART-treated HIV-1-infected persons is still significantly lower compared with age-matched controls [Lohse et al. 2007], even when patients have unrestricted access to high-quality medical care independent of their financial resources. While these findings may in part reflect a higher incidence of other medical problems in HIV-1-infected patients, such as psychiatric illness, smoking, illicit drug abuse, and chronic viral hepatitis, they also seem to point towards intrinsic limitations of current antiretroviral management. Such shortcomings of current HIV treatment relate in part to antiretroviral agent-specific deficits. Some of the currently available drugs still require more than once-daily dosing, which represents a matter of inconvenience and can be associated with lower adherence, particularly in patients who feel healthy. Moreover, many of the currently available agents, in particular NRTI and NNRTIs, have low genetic barriers to viral resistance formation, and mutations in as few as one amino acid can substantially reduce their antiviral potency. Recent data using ultra-deep HIV-1 sequencing techniques suggest that treatment outcomes seem to be worse even when such resistance mutations are only present in small minorities of all viral species circulating in a given patient [Halvas et al. 2010; Paredes et al. 2010]. Finally, many antiretroviral agents remain associated with specific toxicities which complicate long-term use. These include hyperlipidemia (protease inhibitors, efavirenz, and certain NRTIs), mitochondrial toxicity (NRTIs, especially stavudine, didanosine and zidovudine), neuropsychiatric symptoms (efavirenz), nephrotoxicity (tenofovir) and changes in bone and calcium metabolism (tenofovir).
On a broader level, it is now clear that despite the effective suppression of HIV-1 replication by antiretroviral agents, a certain proportion of HIV-1-infected patients fail to experience substantial increases in CD4 T-cells counts, and therefore remain at a higher risk for acquiring opportunistic infections [Gazzola et al. 2009; Gutierrez et al. 2008]; the reason for these insufficient immunological responses to HAART remain a matter of intense ongoing research. In addition, it is evident from a large panel of empiric data that abnormal levels of immune activation persist in the vast majority of individuals, despite treatment with suppressive HAART [Hunt et al. 2008]. This ongoing pathophysiological immune activation is likely to be causally involved in the increased cardiovascular and metabolic comorbidities frequently encountered in HAART-treated HIV-1-infected persons [Obel et al. 2007; Triant et al. 2007; Brown and Qaqish, 2006], and may in part be related to the fact that low levels of HIV-1 viremia remain detectable during treatment with HAART using ultrasensitive molecular technologies [Palmer et al. 2008]. Finally, it is important to recognize that currently available antiretroviral agents are unable to target latently infected CD4 T cells, in which HIV-1 is integrated into the host DNA but remains transcriptionally silent and can persist for prolonged periods of time [Trono et al. 2010; Richman et al. 2009]. The failure of current antiviral agents to eliminate these cells seems to be the predominant reason why current HIV-1 treatment strategies cannot eradicate and cure HIV-1 infection. In the remainder of this article, we outline how specific advances in HIV-1 drug and treatment development may provide solutions for these limitations of current antiretroviral therapy.
New antiretroviral drugs and drug combinations
Significant advances in antiretroviral drug development have led to a number of new pharmaceutical compounds that are currently in advanced stages of clinical development. In comparison with established drugs, these agents seem to have advantageous pharmacokinetics, better tolerability or increased efficacy against drug-resistant viral variants, and might therefore offer important opportunities for improving antiretroviral treatment in the future.
Rilpivirine
Rilpivirine is a second-generation NNRTI for once-daily administration that was recently evaluated in two randomized, prospective phase III studies. Pooled data from more than 1400 treatment-naive patients demonstrated that rilpivirine-based regimens were statistically noninferior to efavirenz-based treatment combinations, although virological failure (9% versus 4.8%) and viral resistance mutations were significantly more frequently observed in the rilpivirine treatment arms [Cohen et al. 2010a]. In contrast, grade 2–4 adverse events including neuropsychiatric symptoms, rashes and liver transaminase elevations were substantially more common with efavirenz (16% versus 31%). Overall, these data suggest that rilpivirine has an excellent safety and tolerability profile, but may be slightly less potent than efavirenz. Rilpivirine is expected to become available in a combined, triple-drug, fixed-dose preparation with tenofovir and emtricitabine for once-daily administration.
Elvitegravir
Another antiretroviral agent in later stages of clinical development is elvitegravir, an integrase inhibitor that is coformulated with tenofovir, emtricitabine and a new pharmacoenhancer (CYP 450-3A4 inhibitor) called cobicistat in a single, fixed-dose pill for once-daily administration. In a recent phase II study involving 71 treatment-naïve patients, this quadruple combination was shown to be noninferior to combined treatment with emtricitabine, tenofovir, and efavirenz, and was associated with fewer adverse effects than the comparator combination [Cohen et al. 2010b]. This elvitegravir-based combination is currently being compared with efavirenz- or atazanavir-based regimens in two large phase III studies; results are expected in the coming years.
Cobicistat
Cobicistat is also being evaluated as a ‘booster’ for protease inhibitors, and can be envisioned as an alternative to low-dose ritonavir for this purpose in future antiretroviral treatment regimens. As with ritonavir, this reagent delays the elimination of other antiretroviral agents by inhibition of the cytochrome P450 enzyme 3A4 (CYP3A4) but due to a more selective mechanism of action, cobicistat is less likely than ritonavir to cause unwanted interactions with simultaneously administered pharmaceuticals [German et al. 2010]. Moreover, cobicistat is devoid of any intrinsic antiretroviral activity and therefore less likely to select for viral resistance mutations. It also appears to confer a lower risk of hepatotoxicity and hyperlipidemia than does ritonavir. A recent phase II study demonstrated that cobicistat is non-inferior to low-dose ritonavir as a pharmacoenhancer for atazanavir in treatment-naïve patients [Cohen et al. 2010b].
Dolutegravir
Dolutegravir (S/GSK1349572) is an investigation second-generation integrase inhibitor that might have preserved activity against viral species resistant to raltegravir or elvitegravir (Eron et al, 2011). In addition, this agent has advantageous pharmacokinetic properties that may support once-daily dosing without requiring ritonavir boosting, although twice-daily dosing appears to be more efficacious in persons with pre-existing resistance against raltegravir [Eron et al. 2011]. Dolutegravir-based regimens are generally well tolerated and were found to be noninferior to efavirenz-based treatment combinations in prior phase II studies [Arribas et al. 2010a]. Dolutegravir will be compared with raltegravir in an upcoming phase III clinical study, and might ultimately become available as a fixed-dose triple-drug combination with abacavir and lamavudine as a first-line treatment option.
Ibalizumab and BMS-663068
Two new pharmaceutical compounds that target HIV-1 entry are currently in earlier stages of clinical development. Ibalizumab is a monoclonal antibody that binds to CD4 and by this mechanism can block viral entry of both CCR5- and CXCR4-utilizing viral species [Bruno and Jacobson, 2010]. This agent requires parenteral administration, but has an extraordinary long half-life that allows for once-weekly dosing. Owing to its unique mechanism of action, it is expected to be active against multiresistant viral species and might expand treatment options for heavily pretreated patients.
HIV entry processes are also targeted by BMS-663068, the first representative of the new drug class of HIV-1 attachment inhibitors. This molecule binds to the viral gp120 envelope protein and prevents its binding to the CD4 cell receptor. In a small study involving 50 HIV-1-infected persons, 8-day monotherapy with BMS-663068 was generally well tolerated and reduced HIV-1 viremia by >1 log [Nettles et al. 2011]. Its distinct pharmacokinetic profile, which does not seem to require ritonavir boosting, as well as its novel mechanism of action could make it an attractive future treatment modality, particularly for treatment-experienced patients with limited alternative therapeutic options.
Alternative combinations to avoid specific NRTI toxicities
In addition to the development of new antiretroviral agents, recent investigations have also focused on treatment regimens that use alternative combinations of established drugs to avoid specific toxicities associated with the use of NRTIs, particularly of abacavir (hypersensitivity, possible increased risk of cardiovascular morbidity) and tenofovir (nephrotoxicity, decreased bone mineral density). These regimens include combinations of a boosted protease inhibitor with an NNRTI [Riddler et al. 2008], an integrase inhibitor [Reynes et al. 2010], or a CCR5 inhibitor [Mills et al. 2010], without concomitant administration of NRTIs. Moreover, it is now well recognized that monotherapy with the ritonavir-boosted protease inhibitors lopinavir [Delfraissy et al. 2008] or darunavir [Arribas et al. 2010b] can have strong antiretroviral effects that are only slightly inferior to conventional antiretroviral regimens, and do not seem to expose patients to substantially higher risks for selecting viral resistance mutations. While such nontraditional antiretroviral regimens appear to be generally safe and effective, specific advantages of such combinations in comparison to existing and well-established treatment approaches have been less evident, and further investigations will be needed to determine whether true improvements of antiretroviral therapy can be achieved by these regimens.
Targeting HIV-1 associated immune activation
The vast majority of previous HIV-1 treatment studies have focused on virological surrogate markers as primary endpoints, such as a suppression of HIV-1 viremia below the threshold of licensed polymerase chain reaction (PCR) assays; increases of CD4 cell counts have typically been used as additional biomarkers for immunological treatment responses. While such endpoints are clearly predictive of clinical responses to antiretroviral therapy, there is a growing awareness that such parameters fail to consider treatment-related changes in immune activation that may be clinically relevant. Immune activation during HIV-1 infection occurs as a result of direct stimulation of T and B cells by HIV-1 antigens [Papagno et al. 2004], bystander activation of immune cells through cytokine secretion [Bangs et al. 2006], and destruction of the micro-anatomical mucosal barrier in the gut that leads to increased translocation of bacterial polysaccharide antigens into the peripheral circulation [Brenchley et al. 2006]. Such levels of immune activation represent an independent and more accurate predictor of HIV-1 disease progression than HIV-1 viral loads [Deeks et al. 2004; Giorgi et al. 1999], and there is now a large panel of empirical data showing that this ongoing immune activation is associated with a number of deleterious consequences that are responsible for a variety of typical comorbidities encountered in HIV-1-infected persons. For example, increased levels of immune activation seem to be related to endothelial dysfunction, pro-atherosclerotic changes in carbohydrate and fat metabolism, accelerated aging, alterations in bone and calcium homeostasis and possibly neurocognitive deficits [Appay and Sauce, 2008]. Despite the ability of current antiretroviral agents to inhibit HIV-1 replication effectively, a number of recent studies have shown that HIV-1-associated immune activation only partially improves after antiretroviral treatment, and abnormally high levels of immune activation persist even after prolonged therapy [Hunt et al. 2008]. Data from our own laboratory, for instance, have shown by comprehensive microarray-based transcriptional profiling that more than 500 gene transcripts involved in immune activation are highly overexpressed in patients on suppressive HAART, compared with a background population of HIV-1 negative individuals [Vigneault et al. 2010]. Notably, this work also demonstrated that a small group of patients with natural control of HIV-1 infection maintained immune activation levels indistinguishable from those of healthy, HIV-1-negative persons, indicating that it is possible for HIV-1-infected persons to achieve normal levels of immune activation. Based on these considerations, it is likely that the efficacy of future antiretroviral treatment regimens may no longer be evaluated simply by their ability to suppress viral replication, but that monitoring of treatment responses may involve specific humoral or cellular immune activation markers. For instance, it is now possible to measure simultaneously up to 100 different cytokines, chemokines, and other pro-inflammatory soluble factors in patient serum using a multiplexed magnetic-bead-based analysis platform. Moreover, microarray-based whole-genome transcriptional gene expression profiling is now readily available at many centers and provides an unprecedented amount of information about the immune activation of cells. In addition, a variety of existing pharmaceutical agents are currently being evaluated for their ability to reduce immune activation during HIV-1 infection. These agents include statins [Ganesan et al. 2011] and chloroquine [Murray et al. 2010], which may limit immune activation through direct anti-inflammatory mechanisms, as well as rifaximin, a nonabsorbed oral antibiotic that might reduce microbial translocation of bacterial polysaccharide antigens from the gut into the peripheral circulation. Integrating such novel treatment approaches into the design of future clinical studies may eventually identify pharmacological strategies that effectively reduce HIV-1-associated immune activation and its deleterious consequences for HIV-1 infected individuals.
Immunological nonresponders
Despite the impressive ability of HAART to induce a complete (or near complete) suppression of HIV-1 replication in the vast majority of patients who strictly adhere to treatment, most studies agree that a significant minority of individuals (between 5% and 30%) fail to mount robust increases in CD4 T-cell counts after initiation of antiretroviral therapy. Epidemiological cohort studies have now clearly shown that such ‘immunological nonresponders’, most commonly defined by having CD4 T-cell increases <30% after 6 months of treatment, have significantly higher rates of mortality and morbidity from HIV and non-HIV-related causes, and worse long-term treatment outcomes [Moore et al. 2005; Grabar et al. 2000]. Insufficient immunological responses appear to occur most frequently in elderly HIV-1-infected persons, in patients with low CD4 T-cell nadirs and in the setting of co-infection with hepatitis C virus [Kaufmann et al. 2005], but the underlying etiology of such discordant responses to antiretroviral therapy remains unclear. Traditionally, insufficient recovery of CD4 T cells has been attributed to defective regenerative functions of bone marrow progenitor cells, thymic degeneration, and/or destruction and fibrosis of the tissue architecture in secondary lymphoid organs such as the gut and peripheral lymph nodes [Diaz et al. 2011; Badolato, 2008]. However, more recent studies suggest that increased destruction of CD4 T cells due to hyperactivation with ensuing cell death play dominant roles in this process [Marchetti et al. 2006; Pitrak et al. 2001]; moreover, certain immunogenetic characteristics that seem to predispose for blunted immunological responses have also been identified [Haas et al. 2006].
Previous efforts to increase immunological treatment responses have most prominently centered on the administration of recombinant interleukin-2 (IL-2), the most potent growth factor for CD4 T cells, in combination with standard antiretroviral agents. In two prospective, randomized phase III clinical trials comparing more than 5000 HAART-treated patients with or without simultaneous subcutaneous injections of this cytokine, IL-2 was effective at increasing absolute CD4 T cell counts by 50–150 cells/µl [Abrams et al. 2009]. However, this numerical increase in cellular immune function failed to translate into clinical benefits, specifically with regard to the frequency of HIV-associated opportunistic infections, and the use of IL-2 as an adjunctive treatment option is therefore no longer pursued. Alternative approaches for enhancing immunological responses to antiretroviral therapy have focused on identifying specific antiretroviral agents with superior abilities to reconstitute CD4 T-cell counts. In this context, it is remarkable that usage of CCR5 inhibitors as a component of antiretroviral regimens has been associated with higher levels of CD4 T-cell recovery in a meta-analysis involving data from 16 clinical trials [Wilkin et al. 2008]. While such findings have not been confirmed in prospective clinical trials [Wilkin et al. 2010; Stepanyuk et al. 2009], they do suggest that specific combinations of antiretroviral agents may be particularly useful for individuals with insufficient immunological responses to antiretroviral therapy. The future availability of additional antiretroviral agents and drug combinations may further expand treatment options for such persons, and holds promise for developing specific clinical strategies for this specific patient population.
A cure for HIV-1 infection?
Current treatment regimens for HIV-1 are very effective at suppressing HIV-1 replication, but HIV-1 persists despite treatment, and rapid virological rebound occurs upon discontinuation of antiretroviral agents. Although the etiology of this long-term viral persistence is still not entirely clear, most of the currently available data suggest that this viral persistence is most prominently related to the presence of memory CD4 T cells with transcriptionally silent HIV-1 infection. In such latently infected cells, HIV-1 is integrated into the chromosomal DNA of resting CD4 T cells, but HIV-1 genes are not actively expressed. In this form, HIV-1 is not affected by currently available antiretroviral agents and can persist for prolonged periods of time. Indeed, current experimental estimates suggest that the half-life of such latently infected cells is longer than 40 months, and mathematical modeling indicates that more than seven decades would be needed to deplete such cells completely, provided that generation of new cells with latent infected could be entirely blocked using existing HIV-1 drugs [Finzi et al. 1999, 1997]. Since the recognition of these underlying dynamics of latently infected cells, the design of novel therapeutic interventions that specifically target latently infected cells has become one of the highest-priority issues in current antiretroviral treatment research. Currently pursued approaches to decrease the number of latently infected CD4 T cells include the initiation of antiretroviral therapy early during the disease process, when the number of latently infected cells is presumably lower than at more advanced stages of HIV-1 infection. Prior work has indeed shown that HIV-1 treatment initiation during acute HIV-1 infection, followed by prolonged antiretroviral therapy for more than 10 years, can substantially reduce the total number of latently infected cells down to the level of one latently infected cell per 1.7 × 109 total CD4 T cells [Chun et al. 2010]. However, even with such a low reservoir of latently infected cells, virological rebound occurred within 50 days after treatment discontinuation, suggesting that currently available antiretroviral agents alone are unable to lead to complete eradication of latently infected cells, even when started during acute HIV-1 infection.
Pharmaceutical agents that might be able to target latently infected cells by reactivating active HIV-1 replication include histone deacetylase inhibitors, a drug class originally developed for oncologic diseases. These agents inhibit histone remodeling adjacent to the HIV-1 gene promoter that otherwise contributes to repression of HIV-1 gene transcription in latently infected cells [Colin and Van Lint, 2009]. Such a forced induction of HIV-1 replication can render HIV-1 viruses in latently infected cells susceptible to currently available antiretroviral drugs that are simultaneously administered. Although previous studies with valproic acid, a licensed anticonvulsive drug with weak biochemical properties of a histone deacetylase inhibitor, has not detectably decreased the number of latently infected cells in most studies [Archin et al. 2010; Sagot-Lerolle et al. 2008], the development of more potent pharmaceutical reagents from this class holds promise for future therapeutic manipulation of the latently infected cell pool. More recent efforts have focused on reducing latently infected CD4 T cells by using immunologic modulators to HIV-1 latency. For example, interleukin 7 (IL-7) has been shown to be highly effective in enhancing reactivation of active HIV-1 replication from latently infected cells [Wang et al. 2005], and clinical studies investigating its use for purging the latently infected cell pool are currently being initiated. Although concerns about the efficacy of such approaches have recently been voiced, particularly since IL-7 may also serve as a growth factor for latently infected cells [Chomont et al. 2009], cytokine-mediated induction of latent HIV-1 provirus may ultimately contribute to treatment strategies aiming for a cure of HIV-1 infection. Finally, reports of a seemingly durable cure of HIV-1 infection after allogeneic transplantation of hematopoietic stem cells with the homozygous CCR5Δ32 gene defect [Allers et al. 2011] have stimulated investigations of using zinc finger nucleases for selectively disrupting HIV-1 coreceptor expression. This approach may allow engineering HIV-1 resistant T cells, which could then be administered to patients as adoptive immunotherapy. While such strategies are obviously associated with numerous challenges, initial experiences in proof-of-principle studies [Lalezari et al. 2011; Wilen et al. 2011] seem encouraging, and warrant further investigation.
Footnotes
Funding
Dr Lichterfeld is supported by a Clinical Scientist Development Award from the Doris Duke Charitable Foundation and by the NIH (grant number AI093203).
Conflict of interest statement
The authors declare no conflict of interest in preparing this manuscript.