
Abstract
Background:
Cytomegalovirus (CMV) infection can lead to significant morbidity and mortality in pediatric hematopoietic stem cell transplant recipients. Early detection of CMV infection is crucial for managing its impact.
Aim:
This study aims to evaluate the effectiveness of QuantiFERON-CMV® (QF-CMV) and QuantiFERON-Monitor® (QFM) tests in predicting CMV infection and graft-versus-host disease (GvHD) in pediatric hematopoietic stem cell transplant recipients to enhance patient outcomes and support personalized prevention strategies.
Methods:
The QF-CMV and QFM tests were used to predict CMV pp65 antigen and GvHD in 24 pediatric hematopoietic stem cell transplant recipients.
Results:
Data showed that positive CMV antigenemia (CMV-Ag) increased the risk of GvHD by 21.2%. QF-CMV and QFM were associated with CMV-Ag, with QF-CMV inversely predicting GvHD. Lymphocyte and neutrophil counts were positively linked to both tests.
Conclusion:
The findings suggest that QF-CMV and QFM tests could predict GvHD and CMV infection risk and help identify high-risk patients, contributing to personalized prevention strategies and improving CMV treatment. Despite the small sample size, this study is an essential proof of concept due to the unique patient population of pediatric bone marrow stem cell transplant recipients. Further multicenter studies are needed to validate these results.
Plain language summary
Cytomegalovirus (CMV) infection is a serious concern for children undergoing hematopoietic stem cell transplants, as it can cause significant illness and complications. Early detection is vital to improving outcomes for these patients. This study explored whether two blood tests, QuantiFERON-CMV and QuantiFERON-Monitor, could help predict the risk of CMV infection and a common transplant complication called graft-versus-host disease (GvHD). Researchers evaluated 24 children with stem cell transplants, analyzing their test results alongside other factors like immune cell counts. The study found that children with positive CMV antigenemia (a sign of CMV infection) were 21.2% more likely to develop GvHD. The QuantiFERON tests were linked to CMV antigenemia and could help predict infection risk. Interestingly, the QuantiFERON-CMV test also appeared to indicate a lower risk of GvHD. Higher counts of certain immune cells, like lymphocytes and neutrophils, were associated with better test performance. Overall, the findings suggest these tests might help doctors identify children at high risk for CMV infection or GvHD, enabling more personalized and preventive treatment strategies. While the study had a small sample size, it highlights the potential value of these tests in managing care for this unique group of pediatric transplant patients. Larger studies are needed to confirm these results.
Keywords
Introduction
Cytomegalovirus (CMV) infection is a significant concern following hematopoietic stem cell transplantation (HSCT) in pediatric and congenitally infected newborns. 1 The presence of CMV DNA in plasma or whole blood is the defining characteristic of an active CMV infection. Infections may manifest as primary infections, arise from the reactivation of latent viruses, or stem from the acquisition of a novel strain of CMV. 2 Both primary and latent CMV infections are possible in HSCT recipients. Recent studies have estimated that CMV reactivation occurs in around 20% of HSCT recipients.3,4 Asymptomatic CMV infection typically develops 8 weeks after transplantation on average. 5 The risk of CMV reactivation in patients is associated with the serostatus of the recipients and the transplant donor.6,7 Cell-mediated immunity (CMI) is crucial in providing the primary defense against CMV disease.
Unlike in solid organ transplantation, seropositive HSCT recipients are at the highest risk of reactivation due to the prolonged absence of T-cell-mediated immunity to control CMV replication.6,8 End-organ disease may develop in 25%–30% of untreated CMV cases, including pneumonia, colitis, graft-versus-host disease (GvHD), and retinitis.9,10 CMV can also cause significant morbidity and mortality in immunocompromised pediatric patients. Consequently, these children are at an increased risk for CMV-related severe diseases. 11 Moreover, CMV alters CMI and may predispose hosts to other bacterial, fungal, or viral infections and graft rejection.12,13 Therefore, accurate prediction of CMV infection and understanding its impact on survival are essential to improving the outcomes for this specific group of patients. Studies have shown that a proactive or preventive approach can prevent CMV disease. Despite the complexity of drug–drug interactions and toxicity, significant reductions in CMV-related morbidity and mortality have been achieved in high-risk children following HCT using prophylactic measures in conjunction with routine CMV monitoring. 14
In addition to the CMV antigenemia (CMV-Ag) test, polymerase chain reaction (PCR) is the standard technique for detecting CMV. 15 Monitoring CMV viral loads can help predict the emergence of antiviral resistance. In the absence of CMI following HCT, virus loads may take several weeks to decrease despite receiving proper therapy. 16
The QuantiFERON-CMV® (QF-CMV) and QuantiFERON-Monitor® (QFM) assays can predict and track CMV infection after allogeneic HCT. 17 A QF-CMV test identifies the CMV-specific T-cell response, suggesting the immune system’s virus control. 18 This test is crucial for controlling CMV infection in pediatric allogeneic HCT recipients.19–21 Furthermore, the QFM assay measures the quantitative evaluation of in vitro IFN-γ production using Enzyme-Linked ImmunoSorbent Assay (ELISA) technique in response to mitogen stimulation of T cells. This quantitative evaluation has advantages over its qualitative predecessors, such as providing data on immunological competency. 22
Our study aimed to compare the effectiveness of CMV pp65 antigen detection in pediatric HSCT in Peripheral blood lymphocytes (PBL) with the predictive value of QF-CMV and QFM assays in predicting GvHD.
Materials and methods
Study design
This prospective observational study was conducted at King Hussein Cancer Center (KHCC) from January 13, 2021 to March 2, 2022, involving 24 successfully engrafted pediatric HSCT recipients. Twenty-one recipients received an allogeneic pediatric HSCT transplant, while three had an autologous transplant. Out of the sample size, 16 individuals underwent fully matched pediatric HSCT, 5 received haploidentical transplants, and 3 underwent autologous transplants. The inclusion criteria didn’t take a particular underlying diagnosis into account. Patients 18 years and older signed a consent form to participate in the trial. Following the Declaration of Helsinki, the parent, guardian, or legal representative of each child participant in the study signed the assent form. The KHCC Ethics Committee-Institutional Review Board (IRB) approved the study protocol with reference number 20 KHCC 83. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, Supplemental Material 1. 23
Collection of blood samples
After Allogeneic Peripheral Blood Stem Cell engraftment, whole blood samples were taken weekly, 7–10 days apart. These samples were tested for QF-CMV and QFM. Parallel to this, CMV-Ag levels were measured. Patient cohorts were observed for at least 100 days. QF-CMV and QFM were done during antiviral treatment in individuals with positive CMV-Ag, indicating CMV infection. Patients’ demographics, pediatric HSCT type, donor type, stem cell source, conditioning regimen, CMV serostatus for donors and recipients, and acute GvHD incidence were collected after enrollment. Prospective clinical data were collected at each testing interval for GvHD, infection identification, CMV reactivation, neutrophil and lymphocyte counts, antiviral prophylaxis or treatment, and underlying disease status monitoring. Acyclovir prophylaxis was given to all PHSCT recipients from day 3 to 12 months following the transplant. Valganciclovir, Ganciclovir, and Foscarnet were also used for preemptive treatment.
CMV-Ag-pp65 test
Three to five milliliters of whole blood was collected from participants. The CMV Brite™ turbo kit detected CMV-Ag. Assessing CMV reactivation involved assessing CMV-Ag (pp65 positive/counted PMNs, PMNs + pp65) using indirect immunofluorescence microscopy (CMV Brite Turbo Kit; IQProducts, Groningen, the Netherlands) as directed by the manufacturer.
QuantiFERON-CMV assay
Whole blood was collected and processed per the manufacturer’s instructions for QF-CMV testing. The CMV peptide pool included 23 peptides that are designed to target CD8+ T cells, including A1, A2, A3, A11, A23, A24, A26, B7, B8, B27, B35, B40, B41, B44, B51, B52, B57, B58, B60, and Cw6 (A30, B130) HLA Class I haplotypes covering >98% of human population. One milliliter of whole heparinized blood was placed into each of three specialized blood collection tubes: CMV Antigen tube, nil control tube (negative control), and mitogen tube containing (positive control). The tubes were centrifuged to separate plasma after 15–24 h at 37°C. Plasma IFN-γ concentrations were measured using manufacturer-provided software and a standard ELISA method.
QFM assay
The QFM assay (QIAGEN Ltd., Manchester, United Kingdom) measured adaptive and innate immune activity. One milliliter of whole blood was incubated with QFM stimulants coated-lyophilized spheres containing R848 and CD3 antibodies. The samples were incubated at 37°C for 16–24 h. After centrifugation plasma was recovered, and IFN-γ concentrations were measured using an ELISA method and manufacturer-provided software.
Statistical analysis
Categorical data were presented as percentages and frequencies. The median was used for scale data, and the Mann–Whitney U test compared positive and negative CMV-Ag days after engraftment. The generalized estimating equation (GEE) predicted CMV-Ag and GvHD from QF-CMV and QF-M. Spearman’s correlation was employed to determine the relationship between QF-CMV and QF-M in relation to the patient’s lymphocyte and neutrophil levels. Point biserial correlation assessed the relationship between CMV-Ag and lymphocyte and neutrophil counts. A p-value of less than 0.05 indicates statistical significance. Data were processed via SPSS IBM version 28 (IBM Corp., Armonk, N.Y., USA).
Results
Transplant recipients’ demographics
The study recruited 24 transplant recipients. The majority were males (62.5%, n = 15). The mean age and standard deviation at the time of pediatric HSCT were 10.12 ± 5.7 years. The age distribution of the participants ranged from 1 to 22 years, with a mean age of 10.12 years (SD = 5.7). Most participants (41.7%) were 6–10 years old, including ages 6, 7, 8, 9, 9.9, and 10. A smaller proportion (20.8%) were in the 1–5 age group, with ages 1, 3, 4, and 5 represented. Participants aged 11–15 accounted for 20.8%, including ages 12, 13, and 15. Those aged 16–20 made up 12.5%, with ages 16, 17, and 18, while only one participant (4.2%) was in the 21–25 age group at 22 years. This distribution reflects a higher concentration of participants in younger age groups, particularly between 6 and 10 years. Malignant conditions accounted for the main indications for PHSCT in the study patients with acute leukemia (37.5%, n = 9), lymphoma (12.5%, n = 3), followed by nonmalignant conditions such as aplastic anemia (16.7%, n = 4), thalassemia (8.3%, n = 2). Eleven pediatric patients had acute GvHD. Table 1 describes the pediatric HSCT recipients enrolled.
Characteristics and clinical data of pediatric transplant recipients enrolled in the study.

CMV, cytomegalovirus; CMV-Ag, cytomegalovirus antigenemia; CsA, cyclosporine A; Cy, cyclophosphamide (Cytoxan); GvHD, graft-versus-host disease; MMF, mycophenolate mofetil; MTX, Methotrexate.
Association between CMV-Ag and GvHD in pediatric patients
We employed the GEE, which modeled the GvHD incident from CMV-Ag status across time. Table 2 shows that the odds ratio of GvHD disease increases by 21.2% in positive CMV-Ag. However, this association is not statistically significant (p = 0.780).
Association between patients’ CMV-antigenemia status and GvHD.
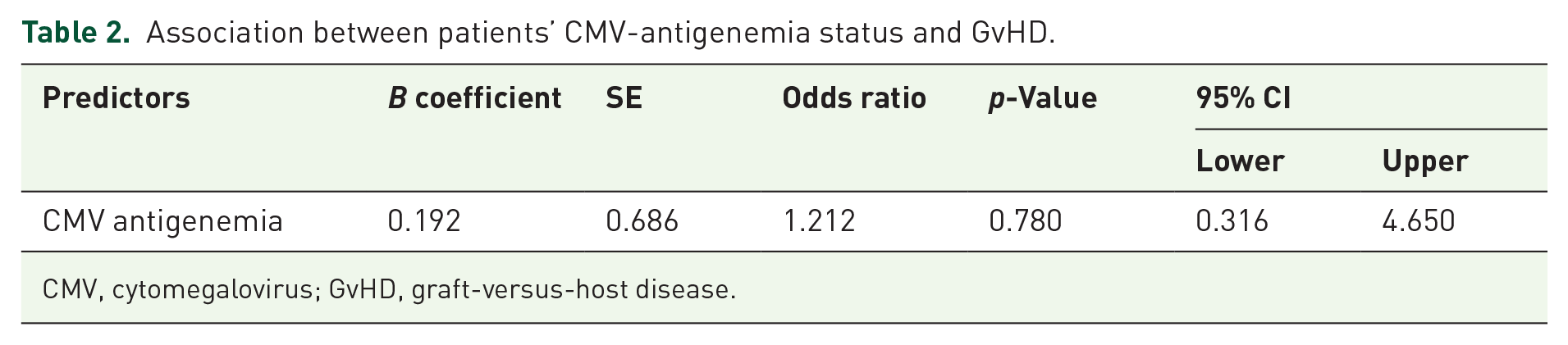
CMV, cytomegalovirus; GvHD, graft-versus-host disease.
Evaluation of QF-CMV and QF-M as CMV infection predictors
The predictive value of QF-CMV and QF-M for patients’ CMV infection status as determined by the CMV-Ag test was analyzed using the GEE statistical test. GEE modeled patients’ CMV-Ag status across time using QF-CMV and QF-M as quantitative variables. The QF-CMV and QFM both showed a negative association with CMV-Ag, as shown in Table 3; however, this correlation was not statistically significant (p = 0.725, p = 0.334).
QF-CMV and QF-M as a predictor test for patients’ CMV infection status.

QF-CMV, QuantiFERON-cytomegalovirus.
Determine the predictive value of QF-CMV and QF-M for GvHD in patients
We used the GEE to model patients’ GvHD over time based on QF-CMV and QF-M test results. The results in Table 4 demonstrate that the QF-M exhibited a positive but not significant association with GvHD; however, QF-CMV showed an insignificant inverse association with GvHD among pediatric patients (p = 0.064, p = 0.274, respectively).
QF-CMV and QF-M as predictors for patients’ GvHD.

GvHD, graft-versus-host disease; QF-CMV, QuantiFERON-cytomegalovirus.
Evaluate the correlation between the patient’s lymphocyte and neutrophil counts and the QF-CMV, QF-M, and CMV-Ag tests
To measure the strength of the association between lymphocyte and neutrophil counts and the QF-CMV, QF-M, and CMV-Ag variables, we used the Spearman’s correlation coefficient (Spearman’s rho). Our data showed that QF-CMV showed a positive association with lymphocytes and neutrophils, although insignificant (p = 0.134 and 0.680, respectively) (Table 5). However, QFM results showed a positive significant correlation with lymphocyte count (rho = 0.248, p < 0.001), and there was a positive but insignificant correlation with neutrophil cell count (rho = 0.079, p = 0.263) (Table 5).
Correlation between the patient’s lymphocyte and neutrophil counts and the QF-CMV, QF-M, and CMV-Ag levels.

Spearman’s correlation.
Point biserial correlation.
CMV, cytomegalovirus; CMV-Ag, cytomegalovirus antigenemia; QF-CMV, QuantiFERON-cytomegalovirus; QFM, QuantiFERON-Monitor.
Regarding the correlation of CMV-Ag with lymphocyte and neutrophil counts, the point biserial correlation demonstrated that lymphocyte count was negatively correlated with CMV-Ag test results (rpb = −0.073, p = 0.300). In contrast, neutrophil cell count was positively insignificantly associated with CMV-Ag test results (rbp = 0.117, p = 0.098) (Table 5). A summary of the results is presented in Table 6.
An overview of the correlation between QF-CMV and QF-M test results and GvHD and CMV infection (CMV-antigenemia).

CMV, cytomegalovirus; GvHD, graft-versus-host disease; QF-CMV, QuantiFERON-cytomegalovirus.
Table 6 shows that each column is a test or indicator (QF-CMV, QF-M, GvHD, CMV infection (CMV-Ag)), and each row represents a specific factor or indicator (CMV-Ag), GvHD, Lymphocyte Count, Neutrophil Count). A negative or positive correlation that is either not significant or significant is shown between the rows and the columns.
Discussion
This study examined the relationship between active CMV infection, QF-CMV assay, and QFM test results in pediatric PHSCT recipients. The test results were employed for GvHD prediction. Our findings suggested that QF-CMV and QFM assays may be valuable tools for predicting CMV infection in pediatric HSCT recipients. Using the CMV Brite turbo test to detect CMV infection is advantageous in our study since it measures actively reproducing virus synthesizing viral proteins. While the CMV-Ag test is not considered the gold standard for diagnosing CMV infection in immunocompromised patients, it remains a widely used and valuable tool due to its ability to detect CMV-Ag in a timely manner. The gold standard for CMV diagnosis is quantitative PCR testing, which directly measures CMV DNA in the blood and offers greater sensitivity and specificity. However, given the limitations of cost and accessibility, the antigenemia test provides a practical alternative for monitoring CMV infection in clinical settings.
Our data showed that the CMV-Ag test results were inversely correlated with QF-CMV and QFM test results. Increased IFN-γ production by T-cells, assessed by QF-CMV and QFM, indicated CMV infection prevention similar to our previous findings in adult transplant patients. 24 However, the small sample size prevented us from confirming the use of QF-CMV and QFM assays as predictors of CMV infection in pediatric patients. Nevertheless, our findings supported previous studies on PHSCT recipients that found that a low risk of recurrent CMV infection was associated with a positive QF-CMV, suggesting that QF-CMV may help assess the risk of recurrent CMV viremia and improve posttransplantation monitoring of pediatric recipients. 25
Additionally, our findings complemented previous studies on adult allogeneic PHSCT recipients, where QFM was demonstrated to be negatively correlated with CMV infection and other studies showed that patients with low IFN-γ levels were more susceptible to CMV infection.26,27 Our results also showed a positive correlation between CMV infection and GvHD, suggesting that CMV infection may cause GvHD. However, the study’s small sample size made this finding insignificant, but previous research found a statistically significant positive correlation between acute GVHD within 6 weeks of transplantation and CMV reactivation. 28
We also found a negative correlation between QF-CMV test results and GvHD, where increased IFN-γ release from CMV-specific T-cells was linked to decreased GvHD incidence. This suggested that CMV-specific T cells, which control CMV infection, can prevent GvHD. These findings align with the study conducted by Tey et al. that reported an association between GvHD and delayed re-constitution of CMV-specific CD8+ T-cells. 28 However, our study found a statistically significant positive correlation between QFM test results and GvHD, where elevated IFN-γ levels detected with the QFM test were correlated with a higher risk of GvHD. To our knowledge, this dataset is the first to show a correlation between QFM test results and GvHD risk in children undergoing HSCT. QF-CMV, QFM, and CMV-Ag tests were compared to the patient’s total lymphocyte and neutrophil counts. QF-CMV correlated positively with lymphocyte numbers (although not statistically significant). Our data showed that an increase in IFN-γ levels, measured by QF-CMV, correlated with a rise in CMV-specific T-cells, as seen in the rise in lymphocyte count, supporting previous results. 27 Additionally, QFM test results showed a significant positive correlation between lymphocyte counts and IFN-γ levels, indicating that an increase in IFN-γ corresponds to an increase in the overall cellular immune response, similar to adult organ transplants. 27
Our data demonstrated a negative correlation between CMV-Ag test results and lymphocyte count. As lymphocyte counts increase, CMV infection risk decreases, corroborating a previous study that indicated lymphocytopenia to be a significant risk factor. 29
However, our results revealed a nonsignificant positive correlation between neutrophil count and CMV-Ag. One possible explanation is that CMV exploits neutrophils to disseminate 30 or slows neutrophil apoptosis. 31 Moreover, the total neutrophil count may correlate with QF-CMV and QFM results but not statistically. To our knowledge, this is the first study to suggest an association between the outcomes of these two tests and the absolute neutrophilic number.
Due to the small sample size, this study has limitations. The small sample size was attributable to the patient’s demographics: 62.5% were under 10. More notably, this study was undertaken during the COVID-19 epidemic, when surgery was almost entirely halted except in emergencies. These findings need to be confirmed in a larger prospective trial with diverse PHSCT recipients that can yield more robust results. Note that the QF-CMV test primarily detects CMV-specific CD8+ T cell activity. Even though these cells directly destroy infected cells, help eliminate them, and regulate viral replication, the test does not detect CMV-specific CD4+ T cells, which are essential for initiating effective immune responses, coordinating immune reactions, and eliminating the virus.
In conclusion, our research underscores a notable association between CMV infection and GvHD in pediatric HSCT recipients. QF-CMV and QFM tests could serve as tools for predicting CMV infection. These preliminary research results help refine Preemptive Therapy (PET), which may improve outcomes and reduce healthcare expenditures. Furthermore, our research suggests the potential utility of QF-CMV and QFM assays in predicting GvHD and its possible implications for patient outcomes. Further research involving a larger sample size and multiple institutional involvement is required to validate these findings and explore their therapeutic implications.
Supplemental Material
sj-docx-1-tah-10.1177_20406207251316680 – Supplemental material for Predicting cytomegalovirus infection and graft-versus-host disease using QuantiFERON-CMV and Monitor in pediatric transplants: a proof-of-concept study
Supplemental material, sj-docx-1-tah-10.1177_20406207251316680 for Predicting cytomegalovirus infection and graft-versus-host disease using QuantiFERON-CMV and Monitor in pediatric transplants: a proof-of-concept study by Lina Souan, Rawad Rihani and Maher A. Sughayer in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.