
Abstract
Background:
Generics imatinib became an alternative treatment option for chronic myeloid leukemia (CML) patients in China. However, clinicians and patients alike harbor concerns regarding the long-term safety of generic imatinib.
Objectives:
Patients with chronic phase CML receiving frontline imatinib treatment.
Design:
A retrospective study was used to evaluate the blood concentration, effectiveness, and safety of generic in 170 CML patients.
Methods:
Imatinib plasma concentrations were detected by high-performance liquid chromatography-tandem mass spectrometry.
Results:
Among the 170 patients, 73 (42.9%) patients treated with branded imatinib as first-line therapy, while 22 (12.9%) switched to generic imatinib during treatment due to economic considerations. No significant differences in trough concentrations between branded and generic imatinib (1549.9 ± 648.8 ng/mL vs 1479.0 ± 507.0 ng/mL; p = 0.95). During the 2-year follow-up, there were no significant differences in molecular response rates (major molecular response (MMR): 33.3% vs 37.0%; deep molecular response: 56.9% vs 42.9%, p = 0.17) between the branded and generic imatinib. Both groups showed similar rates of switching to second-generation tyrosine kinase inhibitor (11.8% vs 15.1%, p = 0.56). Furthermore, there were no significant differences in event-free survival or failure-free survival between branded and generic imatinib. Twenty-two (12.9%) switched to generic imatinib during treatment, 68.2% maintained their level of response, 27.3% improved, and only one patient (4.5%) lost MMR. There were no significant differences in the incidence of various adverse events.
Conclusion:
Generic imatinib are equally effective and safe compared to branded molecules, both for newly diagnosed patients and those who switch from branded.
Introduction
The advent of imatinib has significantly revolutionized the management of chronic phase (CP) chronic myeloid leukemia (CML).1,2 Although tyrosine kinase inhibitors (TKIs) have become the backbone of CML therapy, their exorbitant costs can pose a challenge to patients and healthcare systems. 3 In response to the appearance of generics, the reimbursement policies in several nations have shifted, providing CML patients with an alternative therapeutic choice. 4
Imatinib remains the primary choice of initial therapy for a large proportion of global CML patients. Since the launch of generic imatinib in 2016, several resource-limited countries, such as China, have incorporated them into their treatment plans. Although researchers anticipated a substantial outcome similar to the groundbreaking International Randomized Study of Interferon and STI571 (IRIS) trial, actual results can differ due to real-world conditions. Several studies investigating the effectiveness and safety of generically manufactured CML drugs have been published with discrepant outcomes.5–9 Clinicians and patients alike harbor concerns regarding the long-term safety of generic imatinib. Among the 1518 surveyed CML patients and 259 hematologists, 10 patients expressed their top concerns as TKIs reimbursement policies, TKIs pricing, and new drug development. Conversely, physicians prioritized other issues such as patient monitoring, dose adjustments, and new drug development. While both patients and physicians shared significant apprehension regarding the quality and use of generic drugs, hematologists showed greater concern than patients.
The number of studies evaluating the effectiveness and safety of generic imatinib in CML patients is increasing, although the quantity, particularly in China, remains restricted. This study aimed to evaluate the blood concentration, effectiveness and safety of generic compared with branded imatinib, including newly diagnosed CML-CP patients, and after switching from frontline original imatinib.
Patients and methods
Patients
Between January 2019 and December 2022, we retrospectively recruited CML patients received first-line imatinib therapy at Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. Eligibility requirements for participation included a diagnosis of CML-CP treated with first-line imatinib, age over 18 years, and good adherence (good adherence is characterized by timely and correct imatinib intake daily, along with regular attendance of follow-up appointments). Pharmacists conducted compliance assessments every 3–6 months and provided medication education for patients exhibiting suboptimal compliance levels. Patients were excluded if they had accelerated or blastic phase disease at diagnosis, received first-line treatment with second- (2G) or third-generation TKIs, displayed poor conformity, received medication that could affect imatinib levels, or had incomplete data. We retrospectively collected data on the patients’ clinical information, including demographics, underlying conditions, medication, laboratory results, and adverse events (AEs), through regular outpatient follow-up visits.
Drug administration
All patients were treated with first-line imatinib, taken once daily at a fixed time, with a standard dose of 400 mg. Dose reduction was implemented in patients with sustained optimal response, in cases of severe AEs, desired a decreased financial burden, or as preparation for discontinuation. Patients with sustained deep molecular response (DMR) for over 2 years could discontinue imatinib with physician guidance based on their medical status. Patients who experienced unacceptable AEs or had treatment failure were switched to second- or third-generation TKIs, such as dasatinib, nilotinib, flumatinib, or olverembatinib.
Therapeutic drug monitoring
The imatinib trough concentration was achieved after 28 days of uninterrupted treatment and remained stable thereafter. Once this state was reached, blood samples were drawn into EDTA tubes 24 ± 2 h postadministration and centrifuged at 10,625g for 10 min. The plasma was then stored at −80°C until analysis by high-performance liquid chromatography-tandem mass spectrometry to determine imatinib plasma concentrations.
Clinical response and outcomes
CML-CP was defined as less than 10% blasts in the peripheral blood or bone marrow, and the absence of extramedullary involvement.11,12 Therapeutic efficacy assessment based on the 2020 ELN guidelines. 13 Major molecular response (MMR) was specified as a BCR::ABL1IS level less than 0.1%. The primary objectives were to determine the achievement rate of MMR within 2 years of imatinib treatment and assess the frequency of transitioning to second-generation TKIs. Event-free survival (EFS) refers to the duration from when TKI therapy began until the occurrence of several events, including loss of complete hematological remission (CHR), complete cytogeneric response (CCyR) or major cytogeneric response, loss of MMR, emergence of mutations or clonal chromosome abnormalities in Ph+ cells, progression to advanced phase or blast crisis, or death due to any cause. Additionally, failure-free survival (FFS) was calculated from the start date of therapy until treatment discontinuation for any reason except treatment-free remission (TFR), including changing to alternate TKIs.
Adverse events
At each follow-up visit, patients carried out hematology and biochemistry analyses. Adverse reactions were recorded in accordance with the Common Terminology Criteria for Adverse Events, version 4.0, and including hematologic AEs such as leukopenia, neutropenia, anemia, and thrombocytopenia; gastrointestinal AEs including nausea, vomiting, and diarrhea, along with other symptoms such as fatigue, periorbital and limb edema, rash, musculoskeletal pain, and conjunctival hemorrhage.
Statistical analysis
Descriptive statistics were reported as either percentages or medians with interquartile ranges (IQRs). Categorical variables were compared with the Pearson’s chi-squared or Fisher’s exact test, whereas continuous variables were evaluated via the Mann–Whitney U or Kruskal–Wallis test. Survival probabilities were estimated by means of Kaplan–Meier survival analysis, and these estimates were compared using the log-rank test. Statistical analyses were conducted utilizing IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA), and statistical significance was observed at the p value <0.05 level.
Results
Patient characteristics
The flow chart of our study was shown in Figure 1. Among the 240 patients receiving frontline imatinib treatment, 18 lacking complete data, 32 subjects had irregular response monitoring, and 20 were lost to follow-up were excluded. A total of 170 patients were ultimately included in this study, of whom 86 (50.6%) were male. Among these 170 patients, 73 of them are receiving first-line treatment with branded imatinib (Glivec®), while 97 patients are generic imatinib (Xinwei®, n = 57; Genike®, n = 35, and Nuolining®, n = 5). Demographic and clinical data of branded and generic groups are presented in Table 1. Significant differences were observed in the duration of imatinib therapy between the two cohorts. Patients in the branded imatinib group (11.04 years, IQR [7.83–13.52]) had a lengthier median duration of treatment compared to the generic imatinib group (4.76 years, IQR [3.04–6.72], p < 0.001). Nevertheless, no substantial differences were noted in gender, age, comorbidities, Sokal risk, EUTOS long-term survival score (ELTS score), or TKIs therapy lines between the two cohorts.

The flow chart of this study.
Demographic and clinical characteristics between branded and generic groups.

BMI, body mass index; CML, chronic myeloid leukemia; ELTS score, EUTOS long-term survival score; IQR, inter-quartile range; TKI, tyrosine kinase inhibitor.
In the branded cohort, 22 patients (12.9%) with a median treatment duration of 6.41 years transitioned to generic imatinib due to economic considerations. Additionally, eight patients exhibited an unfavorable response, while two patients demonstrated intolerance, prompting a switch to 2G-TKIs. In the generic imatinib cohort, 14 (8.2%) patients encountered treatment failure (n = 11) or intolerance (n = 3) and subsequently transitioned to a 2G-TKI. Among the 146 patients who did not switch to 2G-TKIs, 78 patients (45.9%) underwent dose reduction (44 prepared for discontinuation, 29 for alleviation of severe AEs, and 5 to mitigate financial burdens), while 10 (5.9%) patients attempted TFR.
Imatinib trough concentration for branded or generic imatinib
Imatinib trough concentration monitoring requires blood collection within 24 ± 2 h postadministration, coordinated with their medication schedule. Because some patients’ medication times do not meet the testing requirements (e.g., if a patient takes medication at 10:00 pm, we are unable to collect their blood for testing), we analyzed the trough concentration of imatinib in 139 patients (branded imatinib, n = 44, generic imatinib, n = 95) who received a daily dose of 400 mg in this study. The individual trough concentrations of imatinib for branded and generic formulations are presented in Table 2. Our findings revealed no significant differences in trough concentrations between branded and generic forms of imatinib (1549.9 ± 648.8 ng/mL vs 1479.0 ± 507.0 ng/mL; p = 0.95) groups. Additionally, we classified the patients receiving 400 mg daily into two categories based on their trough concentration: >1000 and ⩽1000 ng/mL. The results showed no significant difference in the proportion of patients with trough concentrations >1000 ng/mL between branded and generic imatinib (84.1% vs 84.2%; p = 0.99).
Imatinib trough concentrations in branded and generic imatinib.
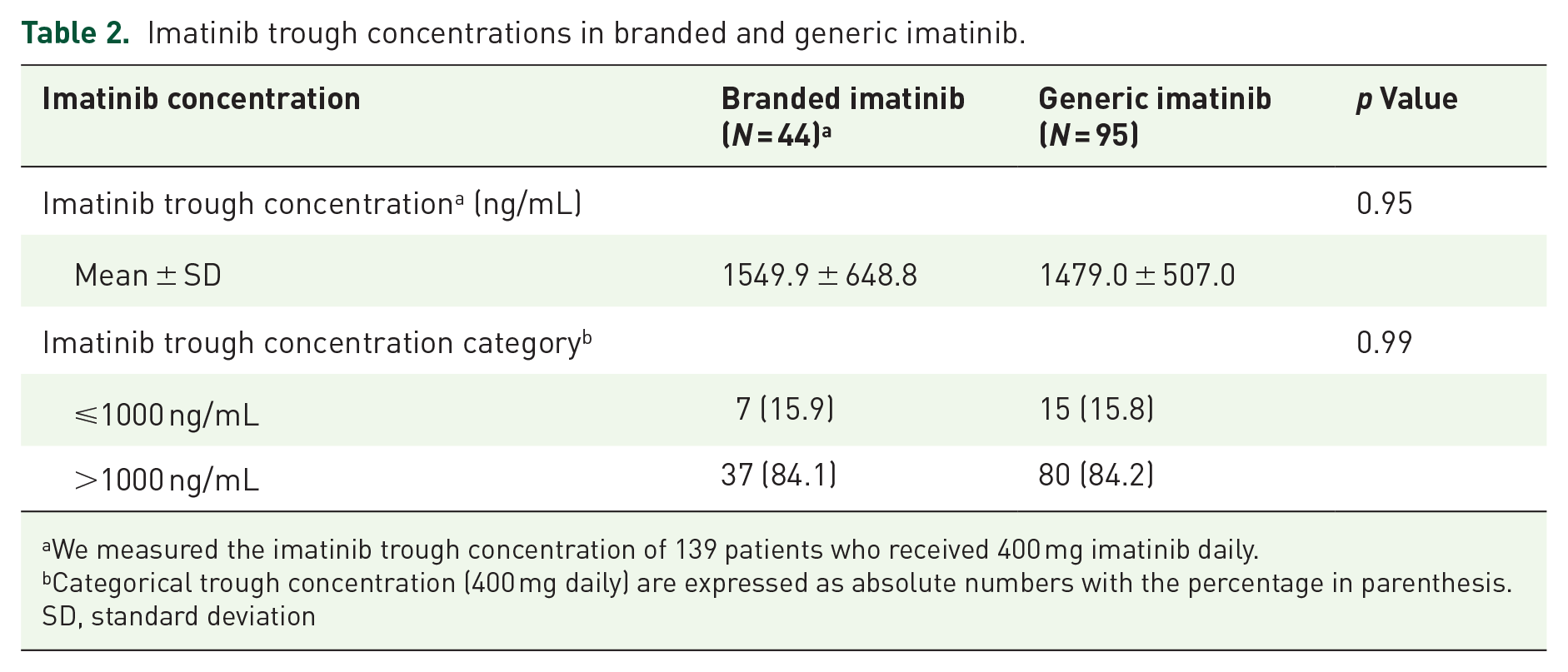
We measured the imatinib trough concentration of 139 patients who received 400 mg imatinib daily.
Categorical trough concentration (400 mg daily) are expressed as absolute numbers with the percentage in parenthesis.
SD, standard deviation
Relationship between clinical outcomes and branded or generic imatinib
A total of 24 (14.1%) patients switched to 2G-TKIs, with a median duration of imatinib treatment was 4.70 years (IQR 2.83–9.27 years). The branded or generic imatinib groups showed similar rates of switching to second-generation TKIs (11.8% vs 15.1%, p = 0.56, Figure 2). We also investigate the clinical outcomes of branded or generic imatinib in a sample of 146 patients who did not switch to 2G-TKIs (Table 3). During the 2-year follow-up period, 33.3% and 56.9% of patients in the branded imatinib group achieved MMR and DMR, respectively. In comparison, 37.0% and 42.9% of patients in the generic imatinib group achieved MMR and DMR, respectively. Statistical analysis showed no significant difference in molecular response between the two groups (p = 0.17). Additionally, 24 (53.3%) and 54 (53.5%) patients underwent reduced imatinib dose in branded and generic imatinib group, respectively (p = 0.97). Furthermore, there were no significant differences in EFS (84.3% vs 89.1%; hazard ratio (HR), 1.16; 95% CI, 0.49–2.77; p = 0.73, Figure 3(a)) or FFS (74.5% vs 79.0%; HR, 1.15; 95% CI, 0.60–2.22; p = 0.68, Figure 3(b)) between branded and generic imatinib.

Comparison of switching to second-generation tyrosine kinase inhibitor rates between branded and generic imatinib.
Comparison of clinical outcomes between branded and generic imatinib.
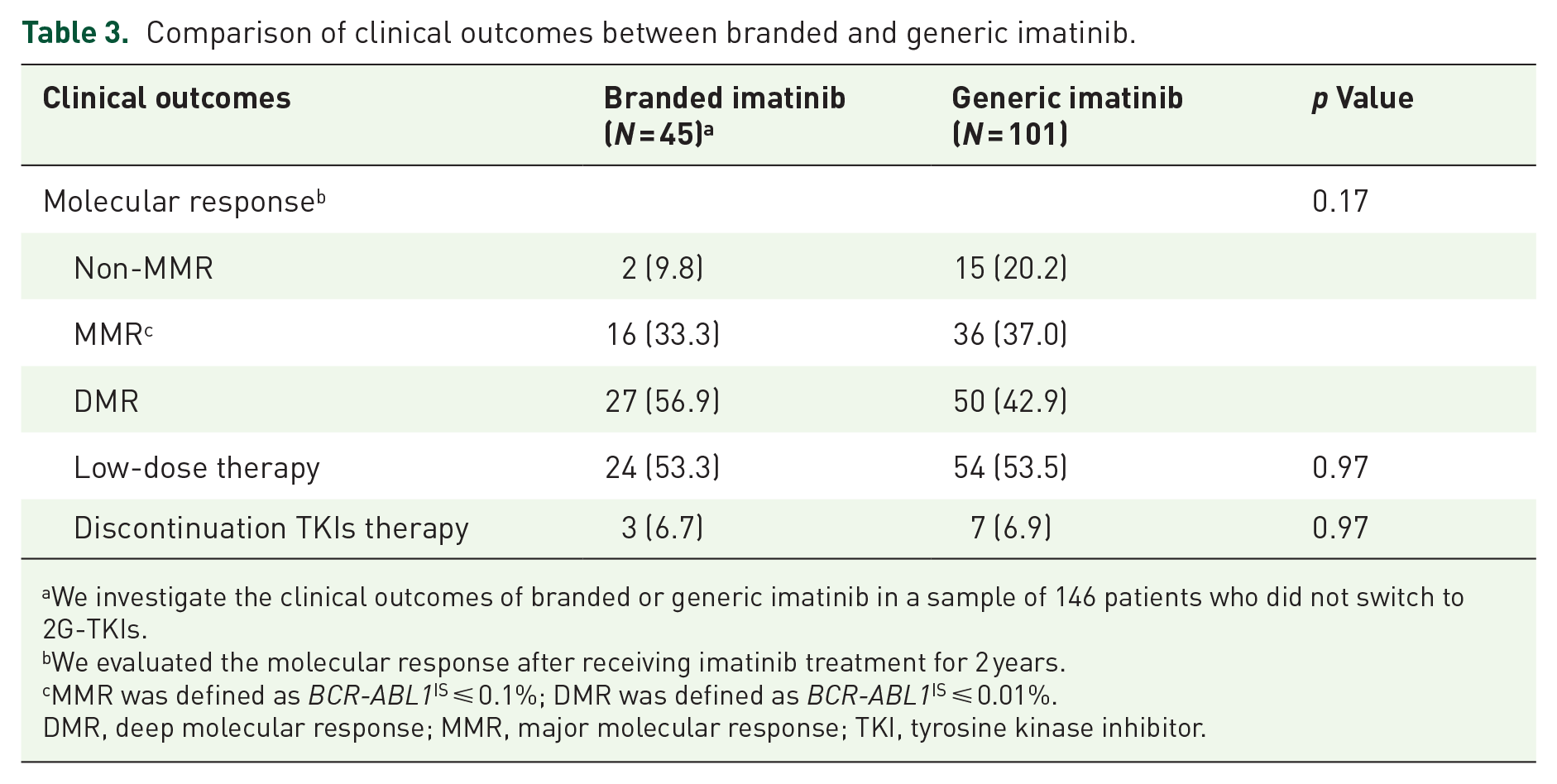
We investigate the clinical outcomes of branded or generic imatinib in a sample of 146 patients who did not switch to 2G-TKIs.
We evaluated the molecular response after receiving imatinib treatment for 2 years.
MMR was defined as BCR-ABL1IS ⩽ 0.1%; DMR was defined as BCR-ABL1IS ⩽ 0.01%.
DMR, deep molecular response; MMR, major molecular response; TKI, tyrosine kinase inhibitor.
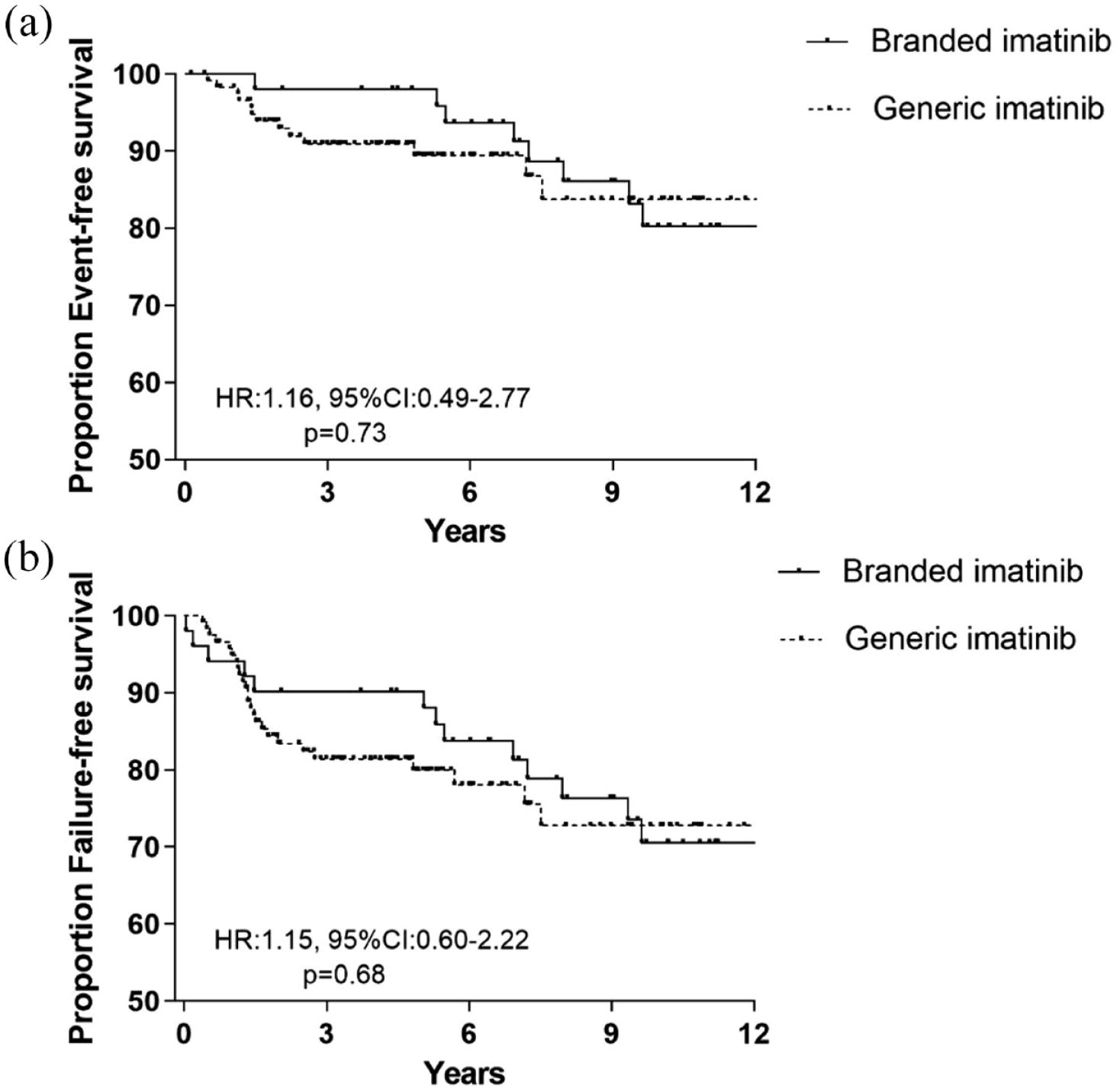
The relationship between branded/generic imatinib and clinical outcomes. (a) Event-free survival (EFS); (b) failure-free survival (FFS).
Twenty-two patients (12.9%) switched from branded to generic imatinib, and their degree of response after conversion was evaluated (Supplemental Table S1). Of these, 68.2% maintained their level of response, 27.3% improved, and only one patient (4.5%) lost MMR. However, four patients underwent a median of 5.41 years of treatment with branded imatinib, then receiving a median of 3.36 years of generic imatinib treatment duo to financial burden. Of these patients, three patients did not achieve MMR, while one patient lost MMR, prompting them to switch to 2G-TKIs.
Correlation of branded or generic imatinib with adverse reactions
Most patients (58.9%) experienced at least one AE while taking branded imatinib, with the most common being musculoskeletal pain, periorbital and limb edema, anemia, and thrombocytopenia (Table 4). After switching to generic imatinib, six patients reported new or exacerbated AEs, with musculoskeletal pain, fatigue, and hyperuricemia being the most prevalent. Additionally, nine patients maintained low-grade persistent AEs, with severity remaining consistent when transitioning from branded imatinib to generic imatinib.
Frequency of AEs associated with treatment using branded and generic imatinib.

This value is not the sum of the column since a patient may have experienced more than one AE.
Discussion
With the emergence of generic imatinib, reimbursement policies of many countries have been changed, and generics became an alternative treatment option for CML patients. In this study, we compared the differences between branded and generic imatinib in terms of plasma drug concentration, efficacy, and safety.
Previous research studies have shown a close correlation between imatinib trough concentrations and clinical response in patients with CML.14–16 Such findings underscore the importance of bioequivalence and bioavailability consistency of generic drugs with the original molecule. In line with this, Natarajan et al. 17 evaluated imatinib plasma trough levels in 206 CML-CP patients, where 130 received original imatinib while the remaining 76 were administered two separate generics. The study showed no substantial difference between the plasma trough levels of branded and generic drugs. Similarly, Malhotra et al. 18 compared imatinib plasma trough levels among 84 patients taking branded imatinib and 47 receiving generic imatinib. Imatinib plasma trough levels did not differ significantly between both groups. Our results also support previous studies, indicating that generic imatinib has comparable bioavailability to the original molecule.
In newly diagnosed CML-CP patients, Danthala et al. 19 conducted a retrospective analysis of 1067 CML-CP patients treated with first-line branded imatinib and 144 patients receiving generics, evaluating both efficacy and safety. Comparable cumulative CCyR rates, EFS, FFS, transformation-free survival (TFS), and overall survival (OS) rates were observed in both groups. No grades 3–4 AEs were reported in either cohorts, although grades 1–2 edema was more prevalent in patients receiving branded imatinib than those given generics (12% vs 5%, respectively). In another study, 442 newly diagnosed CML-CP patients were evaluated (206 patients receiving branded and 236 taking generic imatinib). The cumulative CCyR, MMR, and DMR rates were similar between both groups, and the probability of FFS, progression-free survival, and OS at 4 years did not significantly differ between original molecule and generics. Hematologic and nonhematologic grade >3 AEs were also comparable in both arms. 20
It is also necessary to investigate the efficacy of patients who first receiving branded imatinib and subsequently switch to generic imatinib treatment. An Italian retrospective study 21 analyzed the sustainability of achieved responses after switching to generic from branded imatinib in 140 CML patients. After a median follow-up period of 19 months postswitch, 84% of patients maintained their responses, while 6% showed improved responses. Molecular fluctuations were detected in 10% of cases, but only one patient lost their response during follow-up. The incidence of AEs worsened in 20% of cases, but only 15% of these AEs were recorded as grade >3. A study was conducted on 200 patients who had been diagnosed with CML-CP. 22 The participants were switched to generic medication after achieving stable CCyR for at least 18 months, following no less than 36 months of imatinib treatment. The results showed that sustained, improved, and worsened molecular response rates under generics were 69%, 25.5%, and 5.5%, respectively. Bonifacio et al. 23 found that switch to generic imatinib for patients who have been receiving branded imatinib for at least six consecutive months appears to be effective and safe.
Several studies have reported comparable efficacy and safety outcomes between CML patients treated with generic and original imatinib. However, some studies have shown contradictory findings regarding their effectiveness and toxicity. Saavedra and Vizcarra 24 analyzed a group of 12 patients who switched from branded imatinib to nonbranded drug, revealing that 5/8 patients (63%) experienced treatment failure, while 6/8 (75%) suffered severe and recurrent AEs. Furthermore, a prospective study conducted in Iraq found that one-third of 126 CML-CP patients lost CHR after switching to generic imatinib. 7 In contrast, our study showed that generics exhibited similar 2-year MMR rates, EFS, and FFS compared to the original molecule, both in newly diagnosed patients and those who switched medications. Moreover, in terms of safety, no significant differences in toxicities were observed between the original and generics.
Our study has certain limitations. First, it is a single-center retrospective study with a limited number of participants, so further multicenter and large-scale studies are needed to confirm our findings. Second, we did not grade the adverse reactions. In addition, our study did not evaluate the differences between branded/generic imatinib in terms of TFS, OS, adherence, and healthcare costs. Furthermore, there are three generic versions of imatinib available in the Chinese market. However, due to sample size limitations in each group, we did not compare the differences among the three generic imatinib formulations. In conclusion, our results support the notion that generic imatinib are equally effective and safe compared to branded molecules, both for newly diagnosed patients and those who switch from branded imatinib.
Supplemental Material
sj-docx-1-tah-10.1177_20406207241270806 – Supplemental material for Comparable efficacy and safety of generic and branded imatinib for patients with chronic myeloid leukemia in China
Supplemental material, sj-docx-1-tah-10.1177_20406207241270806 for Comparable efficacy and safety of generic and branded imatinib for patients with chronic myeloid leukemia in China by Fang Cheng, Di Wu, Zheng Cui, Qiang Li, Weiming Li and Yu Zhang in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.