
Abstract
Multiple myeloma (MM) is a hematological cancer characterized by abnormal proliferation of plasma cells in bone marrow. In recent years, autologous stem cell transplantation (ASCT) has become the cornerstone of MM treatment. At the same time, immunotherapy, such as monoclonal antibody therapy and chimeric antigen receptor T cell (CAR-T) has also emerged, in which CAR-T is the most attractive focus. ASCT and its myeloablative preconditioning will turn its immune microenvironment into an inhibited state, which may provide an opportunity for the expansion of CAR-T cells so as to further clear the residual lesions after ASCT and reduce the recurrence rate after ASCT. Meanwhile, the infusion of CAR-T cells can accelerate the cellular immune reconstruction after ASCT of myeloma, thereby improving the antitumor effect. In order to explore the clinic value, this article reviews the progress and prospect of ASCT combined with CAR-T therapy in the treatment of MM.

Introduction
Multiple myeloma (MM) is still incurable under the existing autologous stem cell transplantation (ASCT), chimeric antigen receptor T cell (CAR-T), and other therapies. We screened the literature on this topic in databases such as PubMed Central and China National Knowledge Internet; meanwhile, we searched for relevant clinical studies on clinicalrials.gov. After organizing and describing the analysis, we found that the combination of ASCT and CAR-T may be more effective in treating MM than using either therapy alone, but there are still many issues which needed to be addressed. This article provides a comprehensive explanation of the background, synergistic mechanism, safety, effectiveness, and future prospects of this combination therapy, aiming to provide some insights for clinical doctors and researchers.
Overview of progress and problems in MM treatment
MM is a plasma cell malignant tumor, mainly manifested as destructive bone injury, acute renal injury, anemia, and hypercalcemia. Its incidence ranks second among hematological malignancies. 1 In 2019, more than 155,688 people worldwide were diagnosed with MM. 2 With the deepening understanding of its pathogenesis, people found that immune disorder was the key factor for myeloma cells to escape immune surveillance and cause disease progression.3,4 In recent years, the clinical application of proteasome inhibitors (PIs), immunomodulators (IMiDs), monoclonal antibodies, and CAR-T has brought MM therapy into the era of targeted immunotherapy.1,5–7 However, MM is still incurable, and recurrence and intractability are still the main problems of treament. 7
Autologous transplantation is still irreplaceable in the era of vigorous development of new drugs
In the era of new drugs, the role of ASCT has been questioned. 8 The University of Arkansas conducted the latest analysis of 4329 newly diagnosed multiple myeloma (NDMM) patients treated with ASCT from 1989 to 2018. The results showed that ASCT may cure a small number of patients, ranging from 6.3% to 31.3%, many of whom have normal life expectancy. 9 Among NDMM patients eligible for transplantation, ASCT is still the standard treatment recommended by international guidelines such as the American Society of Clinical Oncology and European Society for Medical Oncology, because ASCT has significant benefits whether compared with patients receiving ‘old’ chemotherapy or those treated with new triads such as PIs and IMiDs. 10 However, the survival benefits of ASCT are limited. 11 The addition of IMiDs, PIs, and other new drugs and the improvement of maintenance therapy further improved the progression-free survival (PFS) and overall survival (OS) of MM patients. However, the problems of relapse and drug resistance still exist, and drugs with new mechanisms of action need to be developed for relapsed/refractory multiple myeloma (RRMM). 12 Compared with the standard-risk patients, the prognosis of high-risk MM patients is still the worst. 8 Therefore, in the future, it can be expected that the consolidation of CAR-T cells or bispecific monoclonal antibodies after transplantation can be used to improve this adverse outcome. 8
CAR-T which is the top representative of immune-targeted therapy, has significant but not lasting effects
CAR-T cell therapy has shown great prospects in the treatment of RRMM. In March 2021, Food and Drug Administration approved the first B-cell maturation antigen (BCMA) CAR-T cell therapy to treat RRMM. There are other targets in the clinical trial exploration stage, such as CD138, CD38, CD19, GPRC5D, SLAMF7, integrin β7, and so on. 13 Roex et al. conducted a systematic review and meta-analysis of the clinical studies published between 1 January 2015 and 1 January 2020. In total, 640 patients used 23 different CAR-T cell products. The combined objective response rate (ORR) and complete response (CR) rates were favorable compared with the expected PFS without CAR-T treatment. 14 Although the ORR and CR rates are impressive, more than half of the patients treated with BCMA CAR-T recur within 1 year. 15 The exact mechanism of drug resistance leading to disease recurrence is still unclear, and the potential mechanisms include clearance of CAR-T cells, antigen escape, and immunosuppressive tumor microenvironment (TME). 16 At present, the methods used to improve the efficacy of MM CAR-T are ongoing.
Put forward a question: how to combine the advantages of ASCT and CAR-T
To sum up, ASCT still has an irreplaceable position in the era of new drugs. CAR-T has become the focus of emerging immunotherapy. Both have their advantages and disadvantages, no matter which one is used, recurrence is inevitable. Therefore, in order to provide the best treatment, we should focus on combination rather than comparison. For relapsed/refractory (R/R) patients, complete remission can be achieved through early CAR-T treatment, and the optimal state can be smoothly bridged to transplantation, achieving the best therapeutic effect. Transplantation combined with CAR-T therapy can improve antitumor targeting and effectively reduce adverse reactions; choosing CAR-T treatment for recurrent patients after transplantation has good efficacy and safety. Among them, hematopoietic stem cell transplantation combined with CAR-T therapy can combine the advantages of both, reducing the recurrence rate and toxic side effects after transplantation, and the combination of the two can expand the scope of applicability. 17 Therefore, this article only explores the progress and prospects of ASCT combined with CAR-T treatment, and we have elaborated in detail on how the two can exert positive complementary effects on each other.
T cells play an important role in the development of MM disease
The immune function of the body can not completely eliminate tumor cells but can make the remaining tumor cells in a functional dormancy state. More and more studies have shown that monoclonal gammopathy of uncertain significance (MGUS)/smoldering multiple myeloma may represent an immune balance by itself, which is destroyed in the process of developing into active myeloma. 6
At present, it has been fully recognized that the changes in bone marrow (BM) microenvironment could promote tumor growth, especially through local immunosuppression and inhibition of antitumor effector lymphocytes to promote immune escape, leading to the evolution of MGUS to MM. 18 Cellular immunity mediated by T lymphocytes is the main antitumor mechanism in MM patients. 6 Effective T cells (CD8+T cells) play a major role in cellular immune response by specifically recognizing endogenous antigen peptides to kill target cells; T helper cells (CD4+T cells) also play an important role in this process. In the clinical process of patients with MM, some abnormalities in the number, phenotype, and function of T cell repertoire have been confirmed. In the process of disease progression, the total number of CD4+T cells decreased, CD8+T cells increased relatively, and the ratio of CD4+/CD8+ decreased. 3 Expanded CD8+T cells have been proven to be associated with a good prognosis.19,20 In the preclinical model, the addition of autologous or syngeneic T cells to BM transplantation significantly improves the survival rate and reduces the progression of myeloma. 21 The function reconstruction of B lymphocytes still needs the assistance of T cells. 22 Therefore, the number and functional recovery of T cells determine the effectiveness of immune reconstitution; people began to vigorously use T cells to fight myeloma, including immunocheck point inhibitors, bispecific antibodies, and CAR-T cells. 12
What synergistic effects does CAR-T therapy have on ASCT
CAR-T therapy can correct the imbalance of T cell immune reconstitution after ASCT to maintain a sufficient number of T cells to play an antitumor role
The cellular immune reconstitution after hematopoietic stem cell transplant (HSCT) depends on two ways: one is that hematopoietic stem cells and lymphoid progenitor cells gradually differentiate into mature lymphocytes depending on the thymus; the other is the expansion of peripheral blood lymphocytes independent of thymus under the stimulation of antigen. 23
Before transplantation, all patients received pretreatment treatment, which caused varying degrees of damage to thymus function, resulting in different recovery times of CD8+ cells and CD4+ cells and long-term inversion of CD4+/CD8+ after transplantation. 4 CD8+T cells proliferate rapidly, while CD4+T cells rely more on the function of thymus than CD8+T cells, so the proliferation is slow.3,23 In addition, in the state of lymphocyte depletion, memory T cells have stronger proliferative capacity than naïve T cells, 24 so most of the expanded cells are effectors or memory T cells, and the number and diversity of naïve T cells cannot be reconstructed. 25 With the steady proliferation of lymphocytes in the thymus, the output function of the thymus gradually recovers, a T cell bank with diverse T cell receptors will be generated, and the balance between various lymphoid subsets will be reestablished. 23 However, the thymus with impaired function will reduce the output of mature T cells, and the early expansion of peripheral T cells is transient and unstable. This is not sufficient to resist tumor cells. If at this time, CAR-T cells are transfused to patients after ASCT. The immunosuppressive environment created by ASCT and pretreatment promotes the expansion of CAR-T cells in vivo. Sufficient CAR-T cells can not only correct the dysfunctional reconstruction of T cell tumor immune microenvironment in MM patients but also more profoundly eliminate tumors. 26
Improved CAR-T cells may be able to antagonize T cell dysfunction after ASCT
ASCT seems to have restored immune balance for a period of time, but it usually follows further escape and disease progression. 18 Immune escape is attributed to a variety of factors, including T cell failure, tolerance of tumor-associated antigen-presenting cells, changes in cytokine production, accumulation of BM derived suppressor cells, and inhibitory tumor-associated macrophages. 18 Among them, cell dysfunction after SCT, including failure and/or aging, contributes to the persistence and progression of tumors. 19
The current CAR-T cells lack persistence and durability. In all MM trials, the degree of CAR-T cell amplification is the most robust marker associated with remission, and this amplification is most significant in patients with lymphopenia. Therefore, the combination of CAR-T cells and ASCT may also be the most effective. 6 In recent years, a new class of engineered CAR-T cells has emerged to resist exhaustion. This kind of CAR-T cells secreting autoantibodies against programmed cell death protein 1 (PD-1). Related studies evaluated their efficacy in lung cancer xenotransplantation model in mice and found that CARαPD1-T cells have stronger expansibility and antitumor effect than CAR-T cells. 27 Other methods to improve the quality of CAR-T cells include selecting specific initial or stem cell/memory T cells, combinations of CD4+/CD8+T cells, and selecting co-stimulatory domains of CD28 and/or 4-1BB depending on the situation. 6 Another approach to preventing tumor escape is enhancing the ability of CAR-T cells to induce the self T cell response in the tumor-bearing host. Some T cell clones from the tumor host are activated through epitope diffusion and subsequently kill tumor cells with altered tumor antigens. 28
Improving the quality of CAR-T cells can not only resist their own depletion and exert long-lasting effects but also activate patients’ autologous tumor-specific T cells. For the T cell dysfunction faced after ASCT, CAR-T therapy is undoubtedly a good complementary method, with the potential to collaborate with ASCT to resist immune escape and exert stronger and more long-lasting antitumor effects.
What synergistic effects did ASCT have on CAR-T therapy
The early stage after ASCT is one of the best opportunities for immunotherapy such as CAR-T
In the early stage after ASCT, lymphocytes decrease, T lymphocytes fail, and tumor load is low. Lymphocytes proliferate steadily during immune reconstitution, and at the same time, it can induce the release of related cytokines, providing a good platform for immunotherapy. 29 Currently approved immunotherapeutic drugs, in addition to the previously mentioned IMiD, have other options to induce MM-specific immunity when the antigen expression is enhanced, such as monoclonal antibodies, CAR-T cell immunotherapy, immunocheck point therapy, adoptive cell therapy, and tumor vaccine. 30 At the same time, immunotherapy further promotes the recovery of lymphocyte function through enhancing the efficacy of ASCT. 30 In acute lymphoblastic leukemia, the response to blinatumomab (anti-CD19/CD3 bispecific antibody) is related to the low Treg level after ASCT. 30 Early administration of drugs in reconstruction is a method to improve tumor-specific immunity, and trials of other methods are also in progress.
CAR-T, as a new immunotherapy option, some clinical trials are investigating the efficacy and tolerability of CAR-T as an early treatment (such as consolidation treatment). 31 The clinical results of CAR-T cells are related to the quality of harvested autologous T cells. 32 In a clinical trial of RRMM, the expansion and response of anti-BCMA CAR-T cells were related to CD4+/8+ cells and high levels of naïve and memory stem cell-like T cells preserved during mobilization and CAR-T manufacturing. 33 Compared with MM patients with severe treatment, T cells suitable for manufacturing CAR-T are easier to be identified in early MM patients. Therefore, the early stage after ASCT is one of the best opportunities for immunotherapy, including CAR-T. 31
ASCT and its pretreatment make up for the limitations of CAR-T therapy and create favorable conditions for CAR-T to better play its antitumor role
CAR-T therapy has shown unprecedented results in B-cell malignant tumors. 34 CAR-T, as a ‘living drug’, propagates in patients, recognizes cancer cells with specific antigens, and kills tumor cells through apoptosis mediated by granzyme/perforin, which enables it to continue to play its role. 35 While, its limitations cannot be ignored. Even patients who respond to CAR-T therapy in the hematologic setting are still at risk of recurrence, which is due to several factors, including poor expansion of T cells, lack of long-term durability after adoptive transplantation, and excessive inhibitory determinants in the TME leading to T cell failure.34,36 Secondly, CAR-T cells may also lead to potential lethal toxicity, including cytokine release syndrome (CRS) and neurotoxicity. 37
Preconditioning is an important part of ASCT. Previous studies have shown that the lymphocyte consumption conditions created by ASCT and conditioning chemotherapy can improve the antitumor effect, expansion, and persistence of CAR-T cells, thus improving the disease-free survival rate.29,34 Moreover, the leukopenia caused by high-dose chemotherapy and ASCT can alleviate CRS. Cytokines derived from BM cells are the main source of CRS, while most patients only have mild or moderate CRS, which may be due to the reduction of myeloid cells and cytokines in high-dose chemotherapy and ASCT. 38 In addition, extensive cell reduction minimizes the use of cytokines by endogenous cells, which leads to higher availability of cytokines for newly transferred T cells, thus enhancing their proliferation and effect function (i.e. steady-state proliferation). 39
Efficacy and safety of ASCT combined with CAR-T therapy in the treatment of MM
At the early stage after HSCT, the number of immunosuppressive cells decreased, and BM clearance therapy liberates the niche of BM stromal cells. If we add CAR-T cells at this time, its effectiveness may be enhanced. 40 CAR-T cells as consolidation or maintenance therapy can reduce the risk of recurrence in high-risk patients after transplantation.
A phase I clinical trial report on central memory-derived CAR-T cells expressing CD19 after ASCT treatment for B-cell non-Hodgkin’s lymphoma presents the results of two studies (NCT01318317 and NCT01815749) (Table 1). Study 1 used CD19 CAR-T cells containing the endogenous domain of CD3, and Study 2 used CD19 CAR-T cells containing CD3 and CD28. Most of the two groups of patients had no disease progression at 1 year, and no CRS or delayed hematopoietic differentiation were observed. 41 Following closely, another study confirmed that CD19 CAR-T cell therapy administered after high-dose chemotherapy combined with autologous stem cell transplantation (HDC-ASCT) was safe and effective for R/R B-cell non-Hodgkin lymphoma (B-NHL) (NCT01840566) (Table 1). 42 Wang et al. 38 studied 14 R/R-diffuse large B-cell lymphoma patients treated with ASCT combined with anti-CD19 CAR-T cells (ChiCTR-OIN-15007668) (Table 1), and 11 patients (78.57%) had complete or partial remission. Median PFS was 14.82 months. Median OS was not achieved, with 1-year OS rate of 65.48%. Seven (50.00%) patients had grade 2–3 CRS, all cases were reversible. 38 With the development of dual targeting CAR-T cells, Cao et al. 43 conducted an open single-arm prospective clinical study (ChiCTR-OPN-16009847) (Table 1). In total, 42 patients received HDT-ASCT and then received anti-CD19/22 CAR-T cell infusion. The total effective rate was 90.5%, and the 2-year incidence of PFS was 83.3%. Only two patients had grade 3 CRS, 5% of patients had severe grade 3 neurotoxicity, and all CRS and neurotoxicity were reversible. 43 Moreover, its clinical results significantly exceeded the previous clinical trials in which the dual targeting strategy was used alone in R/R B-NHL patients (PFS < 50.0% in 1 year). 44 TP53 gene alteration conferences inferior diagnosis in R/R B-NHL. Wei et al. (ChiCTR-OPN-16009847) have proven that CAR19/22 T cell therapy is effective for R/R aggressive B-NHL with TP53 changes (Table 1). Combining ASCT with CAR-T cells can further improve the long-term prognosis of patients. 45 Experiments are also underway on the combination of ASCT and other targeted CAR-T cells for the treatment of hematological tumors, such as CD20 (ChiCTR1900020980) (Table 1) 46 and CD30 (ChiCTR210053662) (Table 1), 47 which have achieved good remission rates. Median PFS and OS were not reached, among which Xue et al. (ChiCTR1900020980) compared patients receiving ASCT + CAR-T treatment with those receiving CAR-T treatment alone. The complete remission rate (CRR) of the ASCT group was 100%, while median PFS and OS were not reached. The CRR of the non-ASCT group was 44.4%, while the median PFS and OS were 4.8 and 13.5 months. 46
ASCT + CAR-T for malignant tumors of B-cell lymphatic system.

ASCT, autologous hematopoietic stem-cell transplantation; BCL, B-cell lymphomas; B-NHL, B-cell non-Hodgkin lymphoma; CAR-T, chimeric antigen receptor T-cell; CNS, central nervous system; CRR, complete remission rate; CR, complete response; CRS, cytokine release syndrome; DLBCL, diffuse large B-cell lymphoma; FDG-PET, positron emission tomography using 18F-deoxyglucose; ICANS, immune effector cell-associated neurotoxicity syndrome; lgH-MYC:lgH-MYC chromosomal translocation; N/A, not applicable; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; R/R, relapsed/refractory; SD, stable disease; VGPR, very good partial remission.
In recent years, relevant studies have explored the effectiveness and safety of ASCT combined with CAR-T therapy for MM (Table 2). Garfall et al. 48 made subjects receive CTL019 after high-dose melphalan and ASCT (NCT02135406) (Table 2). In order to distinguish the clinical effects of ASCT and CTL019, they recruited subjects who had received ASCT before and had adverse reactions (PFS less than 1 year). Study intervention consisted of melphalan at 140–200 mg/m2 followed 2 days later by infusion of ⩾2 × 106/kg CD34+ cells and 14–16 days later by infusion of 1 × 107 to 5 × 107 CAR-T cells. 48 If the subject receives maintenance treatment with lenalidomide after the previous ASCT, it is allowed to start maintenance treatment with lenalidomide approximately 100 days after ASCT. In total, 100 days after ASCT, 8 out of 10 patients showed partial or better response, which is the expected outcome of ASCT alone treatment. To evaluate whether CTL019 extended the PFS after ASCT, they compared the PFS (PFS2) after ASCT + CTL019 with the PFS (PFS1) of each patient after previous ASCT. Compared to previous ASCT, 2 out of 10 subjects showed significantly longer PFS after ASCT + CTL019. 48 The team also conducted another single arm, open label study (NCT02794246). Patients will be included in the trial during induction therapy for MM, and CAR-19 T cells will be injected 60 days after ASCT. Unfortunately, the results were not presented clearly and completely.
ASCT + CAR-T for MM.
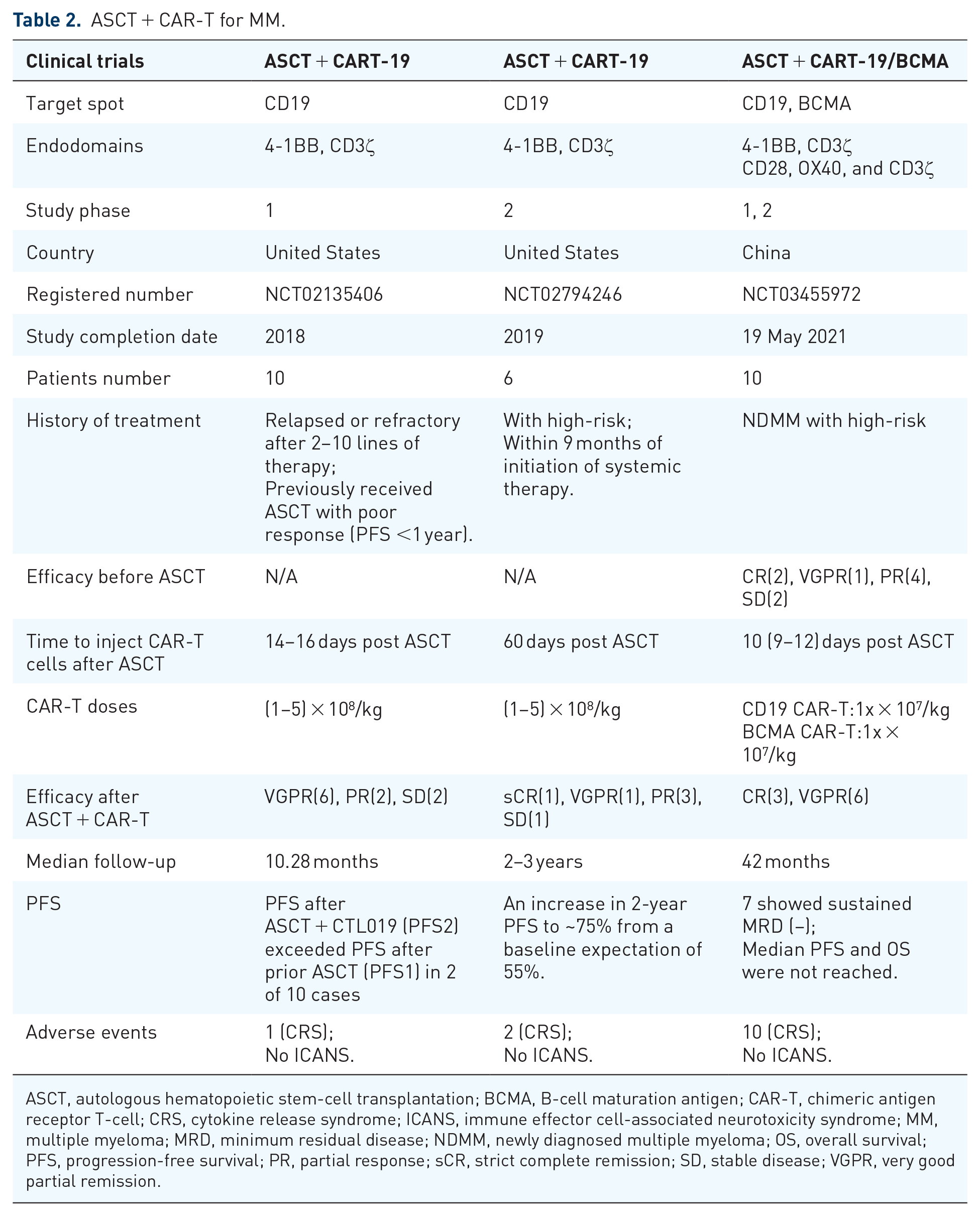
ASCT, autologous hematopoietic stem-cell transplantation; BCMA, B-cell maturation antigen; CAR-T, chimeric antigen receptor T-cell; CRS, cytokine release syndrome; ICANS, immune effector cell-associated neurotoxicity syndrome; MM, multiple myeloma; MRD, minimum residual disease; NDMM, newly diagnosed multiple myeloma; OS, overall survival; PFS, progression-free survival; PR, partial response; sCR, strict complete remission; SD, stable disease; VGPR, very good partial remission.
Anti-BCMA CAR-T cells and anti-CD19 CAR-T cells are the focus of MM cell immunotherapy, which may have the ability to carry out persistent tumor monitoring and disease control for MM patients.49,50 The efficacy and safety of combined infusion of anti-CD19 and anti-BCMA CAR-T cells in patients with recurrent or refractory MM have recently been proven to be beneficial.51,52 It can induce lasting response in R/R MM patients, and has manageable long-term safety. 53 A single-arm exploratory clinical trial evaluated for the first time the safety and effectiveness of maintenance therapy with lenalidomide after sequential infusion of anti-CD19 and anti-BCMA CAR-T cells after ASCT in 10 high-risk NDMM patients (NCT03455972) (Table 2).26,54 After receiving four 28-day PAD (Bortezomib, adriamycin, and dexamethasone) induction cycles, all patients underwent peripheral stem cell mobilization and stem collection, followed by high-dose pretreatment and ASCT.26,54 After hematopoietic reconstruction, continuous infusion of CAR-T cells began. Considering that low tumor load in patients after ASCT may lead to unsatisfactory expansion, the dose of CAR-T cell input was designed to be higher than that of patients with advanced diseases. Starting from the 100th to 110th day after ASCT, oral lenalidomide was administered to prevent disease progression. 26 In this trial, all patients had CRS, but they were self-limited and did not need to take prophylactic tropicamab or corticosteroids. No neurotoxicity was observed. 26 The incidence of strict complete remission (sCR) on the 100th day after ASCT was 80%; with longer follow-up, all 10 (100%) patients responded, of which the sCR rate was 90%, indicating that anti-CD19 and anti-BCMA CAR-T cell infusion after transplantation may further improve the effect of ASCT. 26 On the 100th day after ASCT, 50% of patients showed negative minimum residual disease (MRD). At a median follow-up of 42 months, 7 out of 10 patients showed negative MRD for more than 2 years, and neither median PFS nor OS were achieved, indicating the efficacy of CAR-T cells in residual disease patients. 26
In order to determine the optimal time for ASCT and CAR-T cell therapy for patients, Xiaolan Shi’s team performed a retrospective analysis of the outcomes of 32 patients according to the time of autologous transplantation (NCT03455972) (Table 2). 55 All patients were divided into three groups. Group 1 (18 patients) underwent ASCT and CAR-T cell treatment as first-line therapy; Group 2 (5 patients) underwent ASCT and CART cell treatment at second line because of induction failure or re-induction after PD or relapse; Group 3 (9 patients) underwent salvage ASCT and CART treatment at third line or more after disease progress or relapse. 55 During a median follow-up of 13 months, the latest reactions of CR and above were 78% in group 1, 100% in group 2, and 44% in group 3. The 1-year PFS of the first, second, and third groups were 100%, 100%, and 68%, respectively (p < 0.05); the 2-year survival rates of each group were 100%, 100%, and 64%, respectively (p < 0.05). 55
More clinical trials are underway on ASCT combined with CAR-T cells for MM treatment, such as BCMA CAR-T cell therapy in high-risk NDMM patients with positive MRD after first-line ASCT (NCT058467370), a study of X-VRD combined with CART-ASCT-CART2 treatment in NDMM patients with P53 abnormalities (NCT05850286), ASCT in combination with C-CAR088 for treating patients with ultra-high-risk MM (NCT05632380).
Conclusion and future perspectives
With the continuous deepening of understanding of the pathogenesis of MM and the application of new therapeutic drugs, the survival outcomes of MM patients have been greatly improved. However, there are still some challenges, especially in patients with high-risk cytogenetic abnormalities and recurrent/refractory (R/R) who have poor prognosis. MM cells often undergo clonal evolution under treatment selection pressure, which may lead to disease progression and resistance to conventional treatment. Therefore, the treatment of R/R MM urgently requires new treatment methods. 13
From our current summary of trials, it can be seen that the majority of patients receiving combination therapy are malignant tumors of the B-cell lymphatic system, and they are patients who have not achieved remission or relapse after multi-line therapy. They may or may not have received ASCT, including patients with high-risk cytogenetic abnormalities and double/triple strikes. Most of the experiments were infused with CAR-T cells 2–6 days after ASCT, while some experiments were infused within 100 days after ASCT. These patients achieved good efficacy and good long-term PFS after receiving ASCT + CAR-T combination therapy, and the median PFS of some trials was not yet achieved at the end of the trial follow-up. The inspiration for the use of CAR-T cells in myeloma comes from their significant success in other B-cell lymphoid malignancies. Although CAR-T cell therapy is still in its early stages in MM, it has shown good safety and efficacy in R/R MM patients. 56 There are few reports on the combination of ASCT and CAR-T in the treatment of MM patients, mainly based on the results reported by Alfred L. Garfall 48 and Xiaolan Shi 26 teams. In their published articles, CAR-T cells were infused during the hematopoietic reconstruction phase after ASCT.
Garfall et al. 48 used ASCT + CD19 CAR-T (CTL019) for the treatment of refractory MM, PFS after ASCT + CTL019 (PFS2) exceeded PFS after prior ASCT (PFS1) in 2 of 10 cases. Although both patients received low-dose lenalidomide maintenance therapy after ASCT + CTL019, this cannot explain the prolongation of PFS2 compared to PFS1. One patient’s maintenance treatment regimen had a lower intensity than the previous maintenance treatment regimen given after ASCT, while the other patient did not start maintenance treatment until PFS2 had exceeded PFS1 after ASCT + CTL019. 48 At the same time, the team conducted a retrospective analysis of 18 patients who underwent two ASCTs at their institution from 2008 to 2015 (the first being a component of first-line treatment and the second being salvage treatment for recurrent myeloma) and survived for more than 30 days after transplantation. None of the 18 salvage ASCT cases showed a PFS2 greater than PFS1, and the PFS2/PFS1 ratio in the historical cohort was significantly lower than that in the ASCT + CTL019 cohort of this study. 48 So, in this study, the PFS2 of the two cases was significantly longer than PFS1, which is unlikely to be caused by the second ASCT alone. It proves that CTL019 may improve duration of response to standard MM therapies. Shi et al. 26 studied high-risk patients with NDMM and sequentially infused anti-CD19 and anti-BCMA CAR-T cells after ASCT. As far as we know, this single-center, single-arm, exploratory clinical trial is the first of its kind. The above results demonstrate that ASCT + CAR-T cell therapy not only has good efficacy and safety in treating MM patients but also has good long-term PFS. Moreover, compared with the level after transplantation, the plasma soluble B-cell maturation antigen (sBCMA) level was significantly reduced after CAR-T cell infusion, indicating that the tumor elimination was deeper after ASCT combined with CAR-T cell therapy. 26 High-risk patients already had the worst prognosis, but based on the existing results of this trial, the median PFS of this combination therapy for high-risk NDMM patients was not less than 4 years, and at the end of follow-up, 70% of patients still maintained MRD (−). In recent years, an increasing number of meta-analyses and clinical studies have shown that for high-risk NDMM patients, the MRD (−) state is strongly correlated with prolonged PFS, and the MRD (−) state exceeds the prognostic value of reaching CR. Maintaining the MRD (−) state for as long as possible is more valuable for high-risk diseases. 10 Xiaolan Shi’s team also retrospectively studied the optimal time for ASCT + CAR-T cell therapy in MM patients. 55 It shows that the combined infusion of anti-CD19 and anti-BCMA-CAR-T cells after ASCT in high-risk MM patients is safe and effective, especially as conjunction therapy to early or later transplant at front line even with primary resistant disease or early disease progress. 55
For patients with multiple myeloma (MM), without any treatment in historical reports, the median PFS is 8.5 months. 57 Before the introduction of the new drug, standard treatment included a combination of PIs and oral IMiD and dexamethasone, resulting in a median PFS of 41 months for patients. 57 In the current era of MM treatment, there are excellent treatment plans that can enable approximately 55% of patients to achieve at least 5 years of survival. 58 CAR-T cell therapy can cure some patients with high-grade lymphoma and invasive leukemia. But currently, in the field of MM, there is too little research data on this combination therapy, which is more based on hypotheses and small-scale single-center studies, and lacks a control group. The follow-up time is usually less than 4 years before the end of the trial, and there is no PFS or other data available for about 5 years, so it is not possible to evaluate the long-term benefits it brings. Nevertheless, we found that the vast majority of the study subjects for this combination therapy were recurrent or refractory patients, and even those who received ASCT treatment had a worse prognosis than the general population. The median follow-up time of most of the trials we cited was around 2 years, and the median PFS and OS were not reached. If we follow up for a longer period of time, perhaps we can come to surprising conclusions.
To sum up, the combination of ASCT and CAR-T cells for the treatment of MM has good efficacy and safety. The immune effector cells provided by ASCT can eradicate most tumors and create an ideal environment for immune regulation. However, the increase of immunosuppressive subsets is not conducive to tumor immune monitoring.59,60 And patients with high levels of naïve and terminally differentiated T cells in the early stage after ASCT had a poor prognosis. 48 Therefore, CAR-T cell therapy after ASCT is a promising choice to correct the dysfunctional reconstruction of T cell tumor immune microenvironment in MM. 26 At the same time, the acceptable rates of CRS and immune effector cell-associated neurotoxicity syndrome may be attributed to the minimization of tumor burden and myeloid cells by using enhanced preconditioning protocols and ASCT before CAR-T cell infusion.39,61 Antigen loss is a cellular escape mechanism after CAR-T therapy. Double-targeted CAR-T cells may be initiated and activated by different MM lineages and/or clones of different patients so as to eliminate heterogeneous myeloma cell chambers, further deepen the reaction, and achieve negative MRD after ASCT. 26 The combination of CD19 and BCMA CAR-T cell infusion seems to provide better survival benefits in patients with recurrent or refractory MM.51,52 At the same time, research on double targeting CAR-T cells is also in progress, such as BCMA/SLAMF7 and BCMA/CD38 bispecific CAR-T cells.62,63
We need to continue developing the benefits of ASCT. At the same time, innovative strategies to improve the efficacy and persistence of CAR-T cells, as well as to reduce tumor cell resistance to CAR-T cells, are crucial for further improving patient outcomes. 56 We need more colleagues in the future to further enrich this data and provide strong evidence support. We believe that the continuous improvement of constantly changing treatment models may 1 day make myeloma a curable disease.
Limitations
There are currently few studies on the combination of ASCT and CAR-T therapy, and most of them are small sample studies, lacking strict experimental design and a strong control group. Especially, there are few studies using this combination therapy to treat MM, and they are all self-controlled before and after treatment. Currently, there is no data such as PFS for about 4 or 5 years, so it is impossible to evaluate the long-term benefits it brings, and it is also impossible to calculate the required parameters to determine the sample size required to achieve a certain survival outcome in the next 5 years in a relatively professional and accurate manner. In addition, there is a lack of more clear prospective experimental data to illustrate the comparison between the efficacy of ASCT combined with CAR-T therapy and that of ASCT alone. Because the number of relevant studies is less and the time limit, there is no clear standard for the dose of CAR-T cells, the optimal interval between ASCT and CAR-T in this combination therapy, and the long-term efficacy of the combination of the two in MM remains to be observed. Therefore, more large-scale prospective clinical studies are needed in the future to solve these problems.