
Abstract
Background:
Hematological patients are a highly vulnerable population with an increased risk of developing severe COVID-19 symptoms due to their immunocompromised status. COVID-19 has proven to cause serious mental health issues, such as stress, anxiety, and depression in the general population. However, data on the psycho-social impact of COVID-19 on hematological patients are lacking.
Objectives:
This study aims to examine the psychological well-being of hematological patients in Italy during the initial period of the COVID-19 pandemic. Furthermore, it seeks to explore the association between modifications in the management of hematological diseases and employment status of these patients during the COVID-19 pandemic and the resulting mental health outcomes.
Design and Methods:
A survey using the DASS-21 questionnaire was administered to 1105 hematological patients. Data analysis was conducted using the R software, and logistic regression analysis was performed to predict the association between hematological patient/general population and employment status with DASS scores.
Results:
The hematological patient population reported significantly higher levels of depression (OR 0.947, 95% CI 0.966–0.982, p < 0.001), anxiety (OR 0.948, 95% CI 0.939–0.958, p < 0.001), and stress (OR 0.984, 95% CI 0.977–0.992, p < 0.001) compared with the general population. A significant relationship has been found in stress between employed and unemployed patients (OR 1.015, 95% CI 1.000–1.030, p = 0.044), as well as in the control group (OR 1.024, 95% CI 1.010–1.039, p = 0.001). In addition, employment status is significantly related to depression, anxiety, and stress in both the hematological patient group and the general population.
Conclusion:
During the initial phase of the COVID-19 pandemic, hematological patients had elevated levels of depression, anxiety, and stress compared with the general population. The delay in their treatment and employment status played a role in their mental health outcomes. These findings emphasize the importance of further research to gain deeper insight into the long-term psychological effects and explore effective strategies for managing mental health in similar crises.
Introduction
In December 2019, the first human cases of a new type of severe acute respiratory syndrome coronavirus 2 (SARS-CoV‑2) were identified in Wuhan, Hubei province, China. The highly contagious virus, causing the coronavirus disease 2019 (COVID-19), began to spread quickly around the entire world. 1 Clinical manifestations of COVID-19 range from asymptomatic (no symptoms) to paucisymptomatic (presenting few flu-like symptoms) to severely comprised patients with atypical pneumonia and respiratory failure. 2 Two years after the first COVID-19 cases, the COVID-19 pandemic is still causing unprecedented challenges in the world.
Although the COVID-19 restrictions limited the spread of the disease, several studies highlighted that the potential negative psychological effects of pandemics and lockdowns cannot be ignored. 3 Previously published studies showed that patients recovering from acute viral infections have a higher risk of developing mental problems. As an illustration, several studies have investigated the mental health impact of the SARS outbreak in 2003 and showed that symptoms of stress, anxiety, and depression were more prevalent in SARS patients.4–8 Not only those infected seemed to be at risk to experience negative psychological effects. As Sim and colleagues 9 have shown, the SARS outbreak also negatively affected the mental health of the non-infected population visiting the healthcare centers where the outbreak took place, by causing fear of contracting SARS, losing control of the spread of the virus, and health concerns about family members. Following earlier research addressing the psychological impact of the SARS outbreak, there was an urgent need to explore the impact on mental health caused by the COVID-19 pandemic. Extensive recent research has shown that the COVID-19 pandemic has significantly affected the psychological well-being of the general population (GP).10,11 For example, a study among the GP in China reported that more than half of their respondents rated the mental impact of the COVID-19 outbreak as moderate to severe within the first 2 weeks of the COVID-19 outbreak. 12 Also, Özdin and Bayrak Özdin 13 showed that depression, anxiety, and health anxiety levels were higher among their Turkish study participants.
As previous research has shown, some individuals are particularly vulnerable to mental health issues during this pandemic.14,15 Prior studies have noted that chronic physical health issues, such as diabetes, heart diseases, and cerebrovascular diseases, increased the risk of developing mental health problems during the COVID-19 pandemic.13,16,17 For instance, Li and colleagues 16 found that female respondents with chronic non-communicable diseases were more likely to suffer from depression, anxiety, and stress. Özdin and Bayrak Özdin 13 identified chronic diseases as a risk factor for anxiety disorders, while Chew and colleagues 17 found a significant relationship between comorbid physical health problems and depression, anxiety, and stress among their study population of Chinese healthcare workers. Furthermore, several studies have established that people with cancer, in general, have an increased risk of high psychological distress as a result of the symptoms, treatment, and potentially life-threatening complications of the disease.18–20 A recent study by Edge and colleagues 21 suggests that the COVID-19 pandemic has led to increased psychological distress among cancer patients and more suffering from long-term effects. There are various factors linked to this increased risk, for example, fears of contracting COVID-19, as cancer patients are more vulnerable to infections due to the malignancy and the anticancer treatment causing an immunosuppressive state. 22 Also, researchers suggest that delayed treatment, social distancing from loved ones, financial difficulties, and difficulties in contacting healthcare providers contributed to their increased risk of facing the negative psychological consequences of the COVID-19 pandemic.19,23
Hematological malignancies are a unique subset of cancers that generally require long and aggressive therapies. 24 Several studies have explored the impact of having a hematological disease on patients’ lives, which includes symptoms such as feeling worried, stressed, or anxious about one’s disease and the consequences on one’s life and the lives of others, tiredness, expectations from others, finding fellow patients to talk with about common experiences, and finally, concerns about the reachability of the hospital.25–27 Earlier research underscored the importance of patient-centered healthcare based on the needs of each individual patient in particular in cancer care. 26 Lee and colleagues 28 showed that hematological patients are at increased risk of acquiring COVID-19 infections, compared with both non-cancer patients and cancer patients with solid organ tumors. Furthermore, patients with hematological malignancies appear to be at increased risk of having a severe or critical COVID-19 disease course compared with patients with solid cancers. In addition, Mehta and colleagues 29 reported a significantly higher mortality rate in hematological patients (37%) compared with patients with solid tumors (25%). For this reason, there was an urgent need for adequate protection against COVID-19 in this population. As the COVID-19 vaccines became available for hematological patients, several studies investigated serologic responses to the vaccines in hematological patients. In the majority of investigated participants in the study by Petzer and colleagues, 30 a humoral response to the vaccines was measured. However, in studies by Pascale and colleagues 31 and Haggenburg and colleagues, 32 a great diversity of SARS-CoV-2 antibody responses in accordance with different types of hematological diseases and therapies was observed. Another study showed that hematological patients, especially those diagnosed with multiple myeloma, were at higher risk for a breakthrough infection after being partially or fully vaccinated with mRNA COVID-19 vaccines compared with cancer patients with a solid tumor. 33 Therefore, also vaccinated hematological patients are still advised to minimize their risk of getting infected with COVID-19 by measures like social distancing and the use of personal protective equipment (PPEs). 34
As it is now well established from a variety of studies that cancer patients, and especially hematological patients, are at increased risk of developing physical and psychological consequences of the COVID-19 pandemic, exploring the psychological well-being of these patients in Italy, one of the countries hardest hit by COVID-19, is an urgent need. The first cases of COVID-19 in Italy were detected in February 2020. Therefore, Italy was the first European country to face the COVID-19 outbreak. 34 As the cases spread very rapidly with a high mortality rate, on March 9, Italy also became the first country in Europe to enter a nationwide lockdown. The Italian government decided to close all schools and non-essential businesses and shops until May 18.19,35 Also, gatherings in parks and other public areas were prohibited. 36 Individual physical activity and walking dogs were only possible close to one’s residence. Active transportation was only allowed for essential workers or for visits to a grocery store or pharmacy. 37 Given the fact that Italy has one of the highest numbers of COVID-19 deaths in Europe with one of the strictest lockdowns, increased attention has already been paid to the impact of COVID-19 on Italian people. The survey conducted by Rossi and colleagues 38 has shown high levels of PTSS, depression, anxiety, perceived stress, and adjustment disorder symptoms in the Italian GP. To date, only a limited number of studies have investigated the impact of the COVID-19 pandemic on the mental health status of hematological patients in Italy. Thus far, only one study by Romito and colleagues 19 was conducted to evaluate the psychological status during the COVID-19 lockdown in a subgroup of hematological outpatients receiving anti-neoplastic treatment for lymphoproliferative diseases, in a non-COVID Cancer Center Institute in southern Italy. 19 This study included 77 outpatients with lymphoma in their study using the Hospital Anxiety and Depression Scale, which established that 36% of their patients had anxiety, 31% suffered from depression, and 36% were found to fulfill the diagnostic criteria for post-traumatic stress disorder.
As far as is known, this is the first report to investigate the impact of changes in disease management and socioeconomic modifications during the first part of the COVID-19 pandemic on the mental well-being of Italian hematological patients. Consistent with the investigation of Romito and colleagues, 19 the Depression Anxiety Stress Scale (DASS-21) questionnaire is employed to evaluate the levels of depression, anxiety, and stress in the Italian hematological patient population. Subsequently, this study investigates if there is a link between increased DASS scores and modifications in the management of hematological diseases and employment status of these patients during the COVID-19 pandemic. The GP was used as a control group.
Methods
Study design and participants
In collaboration with AIL (Italian Association for Leukemia, Lymphoma, and Myeloma patients), Bianco Airone (Italian Association for patients with onco-hematological pathologies), and National Research Council, a survey was designed using the DASS-21. This survey was distributed among HP in 20 different Italian regions between April and August 2020. To avoid face-to-face contact, this anonymous self-report questionnaire was administered online via the websites of AIL and Bianco Airone. Participants were recruited by snowball sampling. This study was performed in line with the current Italian privacy legislation; because of the nature of the survey, no IRB approval was necessary and informed consent was requested before entering the survey. The reporting of this study conforms to the Checklist for Reporting Results of Internet E-Surveys statement (Supplemental material). 39
The survey has been developed by the authors based on earlier literature.39,40 The survey for the sample group consisted of 44 questions, divided into 3 different sections. The survey took around 10–20 min for participants to complete. In the first part of the survey, socio-demographic data were collected on age, gender, residential area, employment status, hematological diagnosis, year of diagnosis, and current disease status. The survey for the control group lacked questions regarding hematological pathology, but the remaining part of the survey was identical. The second part of the survey consists of the DASS-21–short version. 40 The DASS-21 questionnaire contains 21 questions to measure depression, anxiety, and stress levels. These three subscales each consist of seven questions. The participants could respond to the questions on a 4-point scale, ranging from ‘it never happened to me’ (0) to ‘it almost always happened to me’ (3).40,41
Total scores for each subscale are calculated as the sum of the scores to all corresponding questions and multiplied by 2 in order to be comparable with the scores of the long version of the DASS-21 questionnaire, which contains 42 items. From here on, the depression, anxiety, and stress scores on the DASS-21 subscales will be together referred to as mental health scores.
The third part of the survey was designed to ascertain the participants’ experiences of diagnostic procedures, treatment, and communication with their practitioners during the COVID-19 pandemic. This part of the questionnaire began with three close-ended questions. The first two questions were regarding the information patients received from their general practitioner and hematologist concerning their hematological disease during the COVID-19 emergency. The third question asked the patient if the COVID-19 crisis has caused any changes to their treatment plan. Following, participants were asked to rate different aspects of disease management during the COVID-19 period, such as the communication with their treatment center, the accessibility of their treatment center, and the access to their (health care) services. This part of the questionnaire utilized a 3-point Likert-type scale, ranging from 0 (no inconvenience) to 2 (serious inconvenience). In the final part of the questionnaire, participants were asked what they are most in need of in this period of the COVID-19 pandemic. Using a 5-point Likert-type scale ranging from 1 (not important) to 5 (very important), each question asked participants to indicate the importance of different aspects of healthcare during the COVID-19 emergency. For example, their need for home care, economic and psychological support, access to treatment centers, COVID-19 tests, and PPEs. At the end of the questionnaire, patients were asked to suggest improvements in the healthcare system for a future emergency.
Statistical analysis
To evaluate the internal homogeneity of the questionnaire, reliability was measured with Cronbach’s alpha. Depression, anxiety, and stress rates in HP were compared with GP as a control group. Data analysis was performed using the R software. Logistic regression analysis was performed to predict the association of HP/GP and employment status to DASS scores. Odds ratios (OR) were calculated by linear regression analysis. We consider a p value less than or equal to 0.05 as significant.
Results
In the period between April and August 2020, a total of 2240 surveys, 1113 HP and 1127 GP, were collected. Not all respondents have completed all sections. For this reason, only 1071 HP and 1127 GP were included for analysis. These two population groups are homogeneous in age, gender, and distribution among the Italian regions (Table 1).
Population distribution among Italian regions.

GP, general population; HP, hematological patients.
Data are n (%).
General characteristics
Table 2 shows the socio-demographic characteristics of the study participants. The median age of both HP and GP was 50 years (range: HP 11–93, GP 13–85). The majority were female (61% HP, 68% GP) and employed (54% HP, 69.2% GP). The year of diagnosis of hematological disease ranges from 1965 to 2020. Table 3 shows the distribution of diagnoses among patients with hematological diseases. Out of all 1071 patients, the majority were in active treatment (58.2%). Of these, 56.4% received outpatient treatment, 40.1% treatment in day hospital, and 3.5% received inpatient treatment at the time of administration of the survey; 41.8% of the total patient group was off therapy.
Socio-demographic characteristics of participants.

p Values were determined by the chi-square test and unadjusted for age and sex.
p < 0.05 is considered to be significant.
Hematological diseases.

Data are n (%).
Disease management and socioeconomic modifications
As shown in Table 4, the majority of HP did not continue to work during the pandemic (63.7%), compared with 36.3% who did continue. On the contrary, in the GP group, 33.8% stopped working during the COVID-19 crisis, compared with 66.2% who continued to work. As shown in Figure 1, their reasons to stop working were layoffs (10.9% HP, 15.9% GP), lack of work (8.1% HP, 15.6% GP), vacation/ parental leave (4.4% HP, 3.5% GP), reduced business activity for economic reasons (2.2% HP, 3.3% GP), occasional work (2.1% HP, 5.7% GP), and seasonal employment (0.6% HP,1.1% GP).
Employment status of participants during the COVID-19 pandemic.

Data are n (%).
p < 0.05 is considered to be significant.

Participants’ reasons to stop working during the COVID-19 pandemic.
As mentioned in the introduction, restrictions on visits and lab/instrumental exams, reduced equipment supply, and a paucity of PPEs for health care providers and patients affected normal routine care. As can be seen from Figure 2, more than half of the patients who responded to this question (n = 1106) experienced difficulties finding PPEs during the COVID-19 period. Out of this group of patients, 11.7% reported that, at the time of the survey, this problem still persists. However, for 43.9% of the patients, the problem of finding PPEs was solved at the time of this questionnaire. Only 6.1% of the patients reported that they have received PPEs from facilities like ‘Protezione Civile’ (Italian Civil Defense) and ‘Servizio Sanitario Nazionale’ (National Health System).
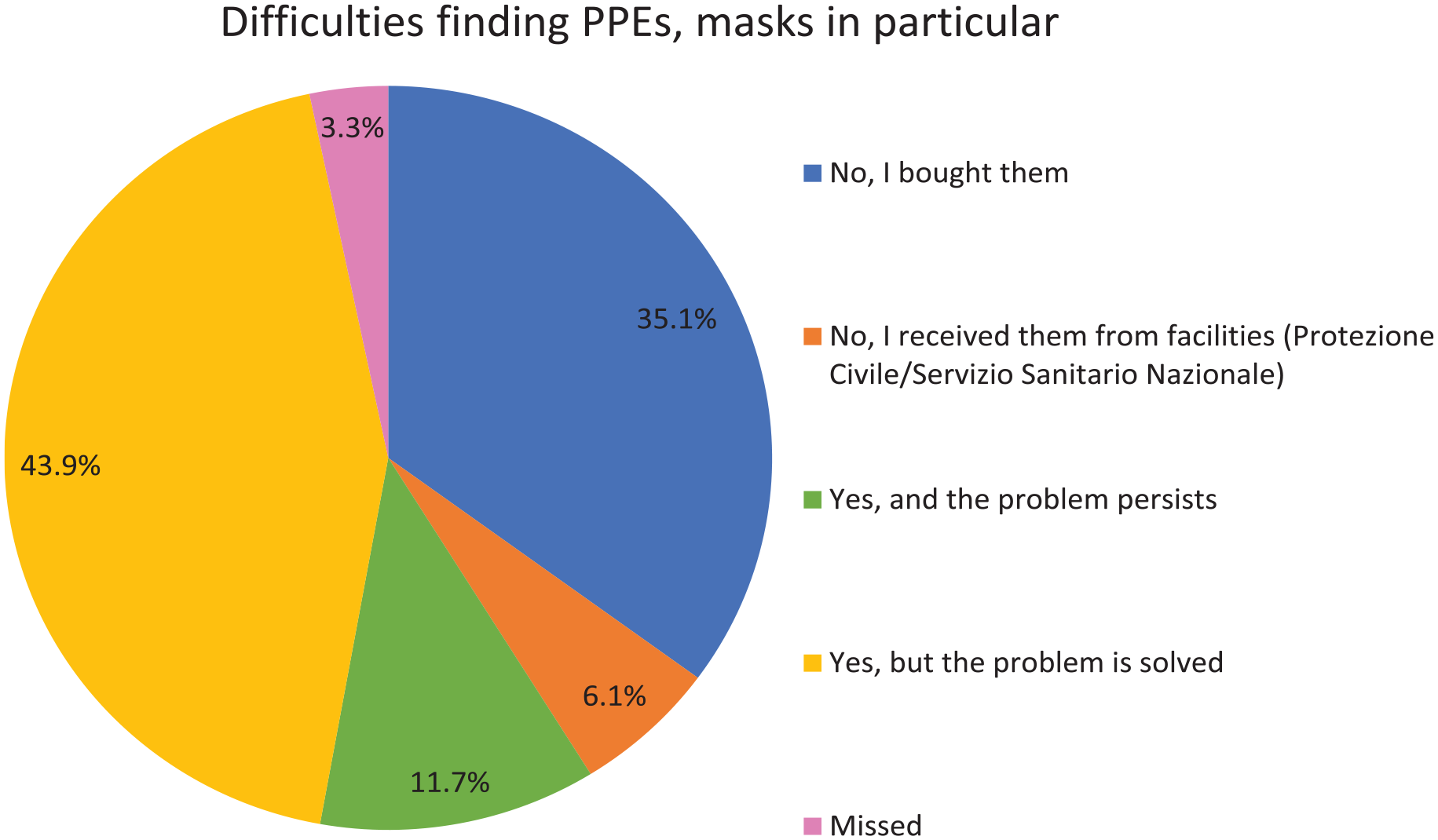
Personal Protective Equipment (PPEs) n = 1106.
Concerning communications with physicians, as shown in Figure 3, 40.5% of all patients who responded to the question (n = 1106) had no contact with their general practitioner (GPr) during the COVID-19 period, of which 36.8% were in active treatment and 48.6% out of the ‘only controls’ patient group. In addition, Figure 3 presents an overview of the information content received from the GPr. It is apparent from this table that another principal part of the patients (n = 362) in both treatment groups only had contact with their GPr regarding electronic prescriptions of drugs (38.3% active treatment versus 27.7% only controls). A total of 17.4% (n = 192) of the patients reported having received information regarding preventive measures for COVID-19 (18% in active treatment, 17.6% only controls). A minority of patients (3.1% in active treatment, 2.7% only controls) indicated that they have received information about extended treatment plans. Respondents were also asked about the information they received from their hematologist (Figure 4). A total of 48.1% of the patients in active treatment received information about preventive measures for COVID-19, compared with 28.5% of patients who only visit the doctor for controls. In this group, 52.4% did not have any contact with a hematologist in the COVID-19 period, next to 23.5% of the patients who were in active treatment. A total of 14.6% of the patients with only controls and 22.4% of the patients in active treatment received information about extended treatment plans. The minority of patients received information regarding the correct use of PPEs (6.0% in active treatment, 4.6% only controls). Interestingly, the percentages of patients who reported that their treatment plan was postponed or rescheduled during the COVID-19 period are higher compared with the percentages of patients who reported having received information about postponing or rescheduling their treatment plan. Figure 5 shows that 37% of the patients in active treatment said that their diagnostic plan (e.g., diagnostic tests, therapies, and administration) was postponed or rescheduled during this COVID-19 period. This percentage is even higher in the group of patients with only appointments for controls, namely, 41.7%.

Information received from a general practitioner.

Information received from a hematologist.
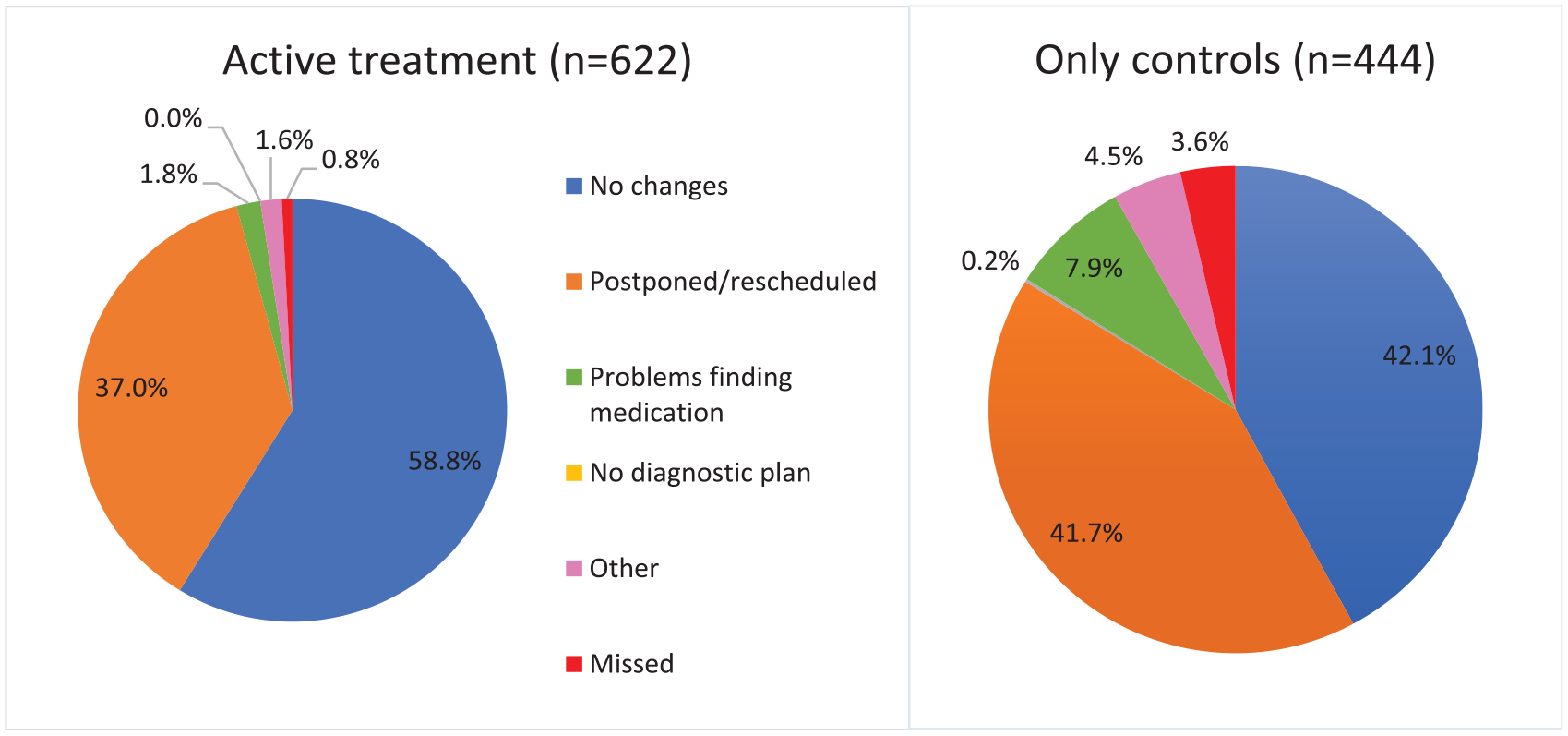
Changes in the diagnostic plan.
As shown in Figure 6, the majority of respondents were receiving outpatient or day hospital care at the time of this survey, and in this setting, the most complaints were identified and shown in Table 5. Serious inconvenience to access to hospital services (toilets, seats available in the waiting rooms, food/drink supplies) during wait times, was noted, respectively, in 17.2%, 17%, and 12.2%, while 38.9%, 24.7%, and 19.3% of the patients reported mild inconvenience.

Type of treatment.
Patients’ inconvenience ratings on health care services during the COVID-19 period.

Data are n (%).
Regarding caregivers’ support, 13.3% reported mild inconvenience to provided accompaniment by caregivers and 10% for the support of the caregiver during consultations with a doctor. An important note is that no one other than the patient was allowed to enter the consulting room, and in some cases the hospital, during the COVID-19 pandemic in Italy. Serious inconvenience caused by these aspects was noted by 10.2% and 6.9% of the patients. Mild inconvenience to communication with the treatment center, access to medicines necessary for one’s disease, and public transport to reach the treatment center were reported by, respectively, 22.3%, 9.6%, and 5.6%, next to serious inconvenience by 9.9%, 4.9%, and 11.2%. In the case of hospitalized patients, 8.1% noted mild inconvenience to communication with caregivers and family members during the COVID-19 pandemic, next to 10.2% of the patients who reported serious inconvenience. The non-mentioned percentages are the percentages of patients who reported no inconvenience.
Figure 7 shows patient perceptions of importance related to health care during the COVID-19 pandemic. A total of 66.3% of patients considered receiving attention from their hematologist as important, of which 47.9% considered it very important. Access to COVID-19 tests, access to PPEs, receiving information and assistance from the government/regions/municipalities, and receiving information regarding living with a hematological disease in the COVID-19 pandemic are considered very important by almost 1 out of 2 patients, 46.1%, 45.6%, 44.3%, and 46.7%, respectively. Hospitality services for caregivers who have to wait outside the consulting rooms or hospitals are important according to 39.3% of the patients, of which 27.2% consider it very important. Comparable results were found on facilities to make sure the caregiver can accompany the patient, 38.3% reported this as important, thereof 25.8% as very important. Useful tools to facilitate communication with the treatment center were rated as important by 45.7% of the patients and as very important by 32.9% of them. Next to that, patients consider useful tools to facilitate communication between caregivers and/or family members and hospitalized patients as less important, namely, 34.9%. Interestingly, home care, accommodation facilities near the treatment centers, and transport facilities to reach the treatment center are rated as unimportant for approximately half of the patients, respectively, 48.8%, 51%, and 47.3%. Economic support is important for 41%, of which 30.8% rate it as very important. Psychological support represents an important need for about 1 out of 2 respondents (49.3%), thereof 35% rated psychological support as very important.

Perceived importance of aspects of health care during the COVID-19 pandemic, as rated by patients.
DASS scores
A total of 1105 HP participants and 1127 GP participants responded to the DASS questionnaire. The DASS-21 subscales severity scores are shown in Figure 8. There was a significant relationship between the two populations and the DASS scores (p < 0.0001). As shown in Figure 9, the HP reported significantly higher levels of depression (OR 0.947, 95% CI 0.966–0.982, p < 0.001), anxiety (OR 0.948, 95% CI 0.939–0.958, p < 0.001), and stress (OR 0.984, 95% CI 0.977–0.992, p < 0.001) compared with the GP. The prevalence rates of mild depression, stress, and anxiety in the HP are, respectively, 13%, 7.9%, and 26.6%, compared with 13.6%, 4.9%, and 27.6% in GP. Higher rates of moderate depression, anxiety, and stress were found in hematological patients, respectively, 18.6%, 18.4%, and 18% in HP, compared with 16.1%, 10.6%, and 14.2% in GP. HP participants also score higher on severe depression (7.7% versus 7.0%), anxiety (7.3% versus 4.9%), and stress (12.4% versus 11.5%). Moreover, extremely severe depression, anxiety, and stress have been more commonly found in HP, respectively, 12.9% compared with 7%, 18.1% compared with 9.6%, and 7.1% compared with 5.3% GP. As shown in Figure 10, a significant relationship has been found in stress between employed and unemployed patients (OR 1.015, 95% CI 1.000–1.030, p = 0.044), as well as in the control group (OR 1.024, 95% CI 1.010–1.039, p = 0.001). In addition, employment status is significantly related to anxiety in both the HP (OR 1.039, 95% CI 1.021–1.057, p < 0.001) and the GP (OR 1.033, 95% CI 1.015–1.052, p < 0.001) and also has a significant relationship with depression in the HP (OR 1.025, 95% CI 1.010–1.040, p = 0.001) and GP (OR 1.048, 95% CI 1.032–1.064, p = 0.001).

Prevalence of different levels of depression, anxiety, and stress in HP (patients, n = 1105) and GP (control, n = 1127).

DASS scores for patient/control.

DASS scores for employed/unemployed status during the COVID-19 group stratified in patient/control.
Discussion
The purpose of this study was to investigate whether there is a link between increased levels of depression, anxiety, and stress and the changes observed in the management of hematological diseases and the employment status of Italian hematological patients during the initial phase of the COVID-19 pandemic. As mentioned in the introduction, only 1 study has examined the psychological status during the COVID-19 lockdown in a subgroup of 77 hematological outpatients receiving anti-neoplastic treatment for lymphoproliferative diseases, in a non-COVID Cancer Center Institute in southern Italy. 20 Our study includes a large group of Italian hematological patients during the first phase of the COVID-19 pandemic and compares this group with a non-hematological control group.
Regarding the DASS questionnaire, this study has revealed significantly higher depression, anxiety, and stress levels in the hematological patient population than in the GP. Our results are comparable with the findings of other studies analyzing the mental health status of people with chronic diseases. As mentioned in the introduction, prior studies have indicated that chronic physical health issues, such as diabetes, heart diseases, and cerebrovascular diseases, have been linked to an increased risk of developing mental health problems during the COVID-19 pandemic, with findings showing a higher likelihood of depression, anxiety, and stress among female respondents with chronic non-communicable diseases, 16 chronic diseases identified as a risk factor for anxiety disorders, 13 and a significant association between comorbid physical health problems and depression, anxiety, and stress among Chinese healthcare workers. 17 Furthermore, Romito and colleagues 19 compared the depression, anxiety, and stress levels of their patients’ population with earlier studies of patients diagnosed with lymphoproliferative neoplasms and stated that these levels are significantly higher during the COVID-19 pandemic. These findings can be understood by considering the unique nature of the COVID-19 pandemic as a stressor. Unlike the negative mental health consequences of natural disasters, where the damage is localized to a specific area and people could have possibilities to escape, or the identifiable enemy in wars. 14 This could especially affect people who are already vulnerable due to physical health issues, such as our group of hematological patients.
Interesting findings have emerged regarding employment status. First, the occurrence of unemployment or job resignations during the COVID-19 pandemic is more prevalent among hematological patients. Second, higher levels of depression, anxiety, and stress, as measured by the DASS questionnaire, are significantly associated with employment status in both patients and controls. These results align with the findings of Posel and colleagues, 42 who discovered that individuals who maintained their employment during the pandemic experienced significantly lower levels of depression compared with those who lost their jobs.
It is important to highlight that this study was conducted during the initial phase of the pandemic when no treatments or vaccines were available. As previously reported by Passamonti and colleagues, 43 hematological patients face an increased risk of severe COVID-19 symptoms due to their compromised immune systems. Consequently, the need for COVID-19 treatments and vaccines may be even more critical among hematological patients compared with the GP. Romito and colleagues 19 stated that 75% (n = 58) of their subgroup of hematological patients reported heightened worries since the onset of the COVID-19 pandemic, with 32.46% (n = 25) expressing concerns about the risk of infection. Additional concerns included potential treatment delays, infected family members, social distancing from loved ones, financial difficulties, and challenges in accessing medical care. These reported difficulties align with our findings, as the majority of our participants reported challenges in obtaining PPEs, and some mentioned treatment postponements and difficulties in reaching their General Practitioner. These factors, combined with limited social interactions due to lockdown restrictions, likely contribute to an increased risk of psychological issues among hematological patients.
Limitations
This study has several important limitations. First, as self-reported questionnaires were used, there is a potential for recall bias in our data. Also, due to the web-based design of the survey, this study is also vulnerable to selection bias as individuals without Internet access were not able to take part in the study and respondents could choose for themselves whether or not to participate in this study. This limitation could affect the overall sample representation and the extent to which the findings can be applied to the broader population. Furthermore, the cross-sectional design of this study makes it challenging to establish long-term cause-and-effect relationships between the COVID-19 pandemic and the mental health of patients with hematological conditions. Moreover, as our study was conducted during the initial phase of the pandemic, the psychological outcomes may have evolved in the long term. It would be valuable to assess the long-term psychological effects of the COVID-19 pandemic on this patient group. Finally, our results only illustrate the mental health statuses of hematological patients within Italy. Given the different treatment approaches and, not insignificant, the variety in COVID-19 restrictions across the world, it is assumed that the mental conditions of hematological patients in other countries differ. It would be interesting to conduct more studies assessing the mental health of hematological patients in other hospitals throughout the world. Furthermore, it is crucial to examine the psychological effects on other vulnerable populations. This knowledge will enable the development of suitable strategies and interventions to protect the mental health of populations at risk of experiencing severe psychological issues during future crises, similar to the COVID-19 pandemic.
Clinical implications
Despite these limitations, this research significantly contributes to our understanding of the mental health impact of the COVID-19 pandemic. However, there remains a lack of knowledge regarding strategies to mitigate the mental health consequences for hematological patients in such a pandemic. Thus, we recommend further studies with a focus on patients’ perceptions and experiences of disease management and socioeconomic adjustments during the COVID-19 pandemic. This would enable the development of recommendations to enhance the mental health support provided to hematological patients in future pandemics.
Conclusion
This study revealed significantly higher levels of depression, anxiety, and stress among hematological patients compared with the GP during the initial phase of the COVID-19 pandemic. The need to delay treatment for these patients was a potential factor contributing to their psychological impact. Our findings also demonstrated a statistically significant relationship between employment status and DASS scores for depression, anxiety, and stress in both the GP and hematological patients.
The findings contribute to our understanding of the mental health impact of the pandemic on hematological patients and highlight the need for tailored support and interventions. To fully understand the long-term psychological effects of the COVID-19 pandemic, further longitudinal research is needed to compare hematological patients with the GP and explore effective strategies for managing mental health in similar crises.
Supplemental Material
sj-docx-1-tah-10.1177_20406207231190683 – Supplemental material for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy
Supplemental material, sj-docx-1-tah-10.1177_20406207231190683 for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy by Marianna De Muro, Annelot Julia Janssen, Sergio Amadori, Paolo de Fabritiis, Dante Sabatino, Pasquale Niscola, Lorenza Torti, Malgorzata Monika Trawinska, Cristiano Tesei, Felice Bombaci, Mario Tarricone, Monica Bocchia, Carmen Fava, Sara Galimberti, Alessandra Iurlo, Luigia Luciano and Elisabetta Abruzzese in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-2-tah-10.1177_20406207231190683 – Supplemental material for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy
Supplemental material, sj-docx-2-tah-10.1177_20406207231190683 for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy by Marianna De Muro, Annelot Julia Janssen, Sergio Amadori, Paolo de Fabritiis, Dante Sabatino, Pasquale Niscola, Lorenza Torti, Malgorzata Monika Trawinska, Cristiano Tesei, Felice Bombaci, Mario Tarricone, Monica Bocchia, Carmen Fava, Sara Galimberti, Alessandra Iurlo, Luigia Luciano and Elisabetta Abruzzese in Therapeutic Advances in Hematology
Supplemental Material
sj-docx-3-tah-10.1177_20406207231190683 – Supplemental material for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy
Supplemental material, sj-docx-3-tah-10.1177_20406207231190683 for Impact on mental health, disease management, and socioeconomic modifications in hematological patients during the COVID-19 pandemic in Italy by Marianna De Muro, Annelot Julia Janssen, Sergio Amadori, Paolo de Fabritiis, Dante Sabatino, Pasquale Niscola, Lorenza Torti, Malgorzata Monika Trawinska, Cristiano Tesei, Felice Bombaci, Mario Tarricone, Monica Bocchia, Carmen Fava, Sara Galimberti, Alessandra Iurlo, Luigia Luciano and Elisabetta Abruzzese in Therapeutic Advances in Hematology
Footnotes
Acknowledgements
We thank all the patients, volunteers who participated in this study, and colleagues who helped spread the survey. We also thank Bianco Airone, GIMEMA, Linfoamici, and all patients’ advocacies.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.