
Abstract
Background:
Blinatumomab showed a higher complete remission (CR) rate and a safe bridging to allogeneic hematopoietic cell transplantation (allo-HCT) in adults with relapsed or refractory B-cell precursor acute lymphoblastic leukemia (R/R BCP-ALL).
Objectives:
We tried to analyze the outcome of blinatumomab compared with the real-world historical data. We expected superior outcome of blinatumomab compared with historical conventional chemotherapy.
Design:
We conducted a retrospective study using real-world data in the Catholic Hematology Hospital.
Methods:
Total 197 consecutive cases of R/R BCP-ALL were treated with conventional chemotherapy (n = 113) or blinatumomab, which was available since late 2016 (n = 84). Patients who achieved CR underwent allo-HCT if donor was available. We conducted a propensity score–matched cohort analysis using 5 criteria of age, CR duration, cytogenetics, previous allo-HCT, and salvage lines between historical group and blinatumomab.
Results:
Each cohort consisted of 52 patients. In blinatumomab group, CR rate was higher (80.8% versus 53.8%, p = 0.006) and more patients proceeded to allo-HCT (80.8% versus 46.2%, p < 0.001). Among the CR patients with available minimal residual disease (MRD) results, 68.6% in blinatumomab group and 40.0% in conventional chemotherapy group were MRD-negative. Regimen-related mortality during the chemotherapy cycles was significantly higher in the conventional chemotherapy group (40.4% versus 1.9%, p < 0.001). Estimated 3-year overall survival (OS) was 33.2% (median, 26.3 months) after blinatumomab, and 15.4% (median, 8.2 months) after conventional chemotherapy (p < 0.001). Estimated 3-year non-relapse mortality were 30.3% and 51.9% (p = 0.004), respectively. In multivariate analysis, CR duration < 12 months showed more relapses and poor OS, and conventional chemotherapy showed higher non-relapse mortality and poor OS.
Conclusions:
Matched cohort analysis showed superior outcomes of blinatumomab compared with conventional chemotherapy. However, large numbers of relapses and non-relapse mortalities continue to occur even after blinatumomab followed by allo-HCT. Novel therapeutic strategies are still needed for R/R BCP-ALL.
Keywords
Introduction
Although the complete remission (CR) rates exceed 90% in adults with B-cell precursor acute lymphoblastic leukemia (BCP-ALL), many patients continue to relapse, with a long-term overall survival (OS) rate of 30–60% after intensive chemotherapy or allogeneic hematopoietic cell transplantation (allo-HCT).1–4 For relapsed or refractory (R/R) BCP-ALL, allo-HCT after achieving CR remains the best curative option. However, it has been difficult to achieve a subsequent CR with conventional chemotherapy due to treatment-related toxicity and insufficient response. In addition, allo-HCT is still associated with high non-relapse mortality (NRM).5–7
Several immune-based treatments, such as bi-specific T-cell engager (BiTE)8,9 and antibody-drug conjugate platforms,10–12 have been introduced and are now used as safe salvage and bridging therapies to allo-HCT. As an alternative to allo-HCT for R/R BCP-ALL, chimeric antigen receptor engineered T-cell therapy (CAR-T) also has been applied in clinical trials, and its general use is approved in some countries. 13 As the first BiTE antibody platform to be demonstrated as a potent therapeutic option, blinatumomab offers an effective safety profile for subsequent allo-HCT and favorable long-term survival outcomes, particularly in patients treated with an earlier salvage line.14–17
Real-world data for blinatumomab, including reports that compare the results of clinical trials to those of historical standard of care, have recently been published.18–20 Previously, we also reported that patients receiving blinatumomab as first-line salvage treatment achieved superior CR rates and favorable survival outcomes after allo-HCT in R/R Philadelphia chromosome (Ph)-negative BCP-ALL, although the follow-up duration was only 1 year. 21
In this study, the clinical outcomes of R/R BCP-ALL treated with blinatumomab were compared with those of a historical cohort receiving conventional intensive chemotherapy [mitoxantrone, etoposide, and cytarabine (MEC)]. We performed a propensity score–matched cohort analysis to make more accurate comparisons.
Patients and methods
Patients according to era of salvage therapy
From March 2009 to February 2021, we analyzed 197 patients with R/R BCP-ALL who were treated with conventional chemotherapy or blinatumomab as salvage therapy at Catholic Hematology Hospital in Korea. In 2016, Korean National Health Insurance approved blinatumomab for patients with Ph-negative BCP-ALL who failed induction chemotherapy or relapsed after chemotherapy or allo-HCT. And then we were able to use blinatumomab for salvage in Ph-positive BCP-ALL patients beginning in 2019. The Institutional Review Board of The Catholic University of Korea approved this study, and written informed consent was obtained from all patients and the details were also de-identified (KC21RISI0613). The study was conducted in accordance with the Declaration of Helsinki. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Salvage therapy regimens
As described in our previous studies, induction chemotherapy was started with a modified regimen of fractionated cyclophosphamide, vincristine, doxorubicin, dexamethasone (hyper-CVAD), and alternating high-dose cytarabine and mitoxantrone.22–25 Patients who failed to achieve CR or relapsed after CR received intensified salvage chemotherapy using an MEC regimen consisting of cytarabine (2 g/m2, every 12 h, days 1–4), mitoxantrone (12 mg/m2, days 1–4), and etoposide (100 mg/m2, days 5–7). Patients with Ph-positive ALL also received tyrosine kinase inhibitors (imatinib or dasatinib).24–28 In patients who revealed minimal residual disease (MRD) at 3 months post-transplant, we applied preemptive tyrosine kinase inhibitors. Since 2016, blinatumomab was used as a monotherapy for all above indications instead of MEC regimen in the same way of our previous study. 21 Before application of blinatumomab, all patients received prephase dexamethasone to reduce leukemic burden and cytokine release syndrome (CRS). During the first cycle, blinatumomab was continuously infused for 4 weeks (9 μg/day for the first 7 days and 28 μg/day thereafter). After a 2-week treatment-free interval, a second 4-week cycle was initiated at a dosage of 28 μg/day from day 1 to day 28. Even after 2016, we applied the MEC regimen to some patients who failed to blinatumomab, while some others were treated with inotuzumab ozogamicin (INO) as it became available for R/R Ph-negative ALL since late 2019.29,30 Doses of INO were administered at 0.8 mg on day 1 of the first cycle (0.5 mg on the day of the second cycle) and 0.5 mg on days 8 and 15. The interval of the first cycle was 28 days, and up to two cycles were approved.
Post-remission therapy and disease related parameters
For patients who achieved CR, allo-HCT was offered as early as possible if a matched sibling donor or unrelated donor with ⩽ 1 mismatched allele was available. If a patient had no available matched sibling or unrelated donor, cord blood transplantation (CBT) or haploidentical-related donor transplantation (HIDT) was considered, and the detailed information is referred to our previous article. 4 The International System for Cytogenetic Nomenclature (ISCN) was used to detect clonal abnormalities, 31 and risk subgroups were classified according to National Comprehensive Cancer Network (NCCN) guidelines. Poor-risk cytogenetics were defined as a complex karyotype of 5 or more chromosomal aberrations, hypodiploidy, and KMT2A rearrangements, while other abnormalities were classified as standard-risk cytogenetics. A CR was defined as ⩽5% bone marrow (BM) blasts, absolute neutrophil count > 1 × 109/L, and platelet count > 100×109/L. Because MRD for Ph-negative ALL was only assessed beginning in 2019, just a part of patients had available MRD data, which made it difficult to analyze in detail. 32
Statistical analysis
The main end point was CR rates. End points of OS, disease-free survival (DFS), cumulative incidence of relapse (CIR), and NRM rates were also compared between the blinatumomab group and conventional salvage group. For efficiency evaluations of CR rates between the two salvage groups, we used a conditional method to calculate sample size. At least 42 patients were needed for each group. In this study, we conducted a propensity score–matched cohort analysis using age, cytogenetics at relapse including Philadelphia (Ph) chromosome, CR duration before relapse, line of salvage, and history of previous allo-HCT. Response rates were compared using Fisher’s exact test. OS curves were plotted using the Simon–Makuch method, considering the effect of allo-HCT as a time-dependent covariate. DFS was plotted using the Kaplan–Meier method for patients who achieved CR after each salvage therapy. CIR and NRM rates were calculated using a cumulative incidence estimate to accommodate competing events, and subgroups were compared with Gray tests. The prognostic significance of covariates affecting OS was determined by a Cox proportional hazards regression model in which allo-HCT was a time-dependent covariate. The prognostic significance of covariates affecting CIR and NRM was determined using Fine-Gray proportional hazards regression for competing events. Multivariate analyses were performed using variables with a p-value < 0.10 in prior univariate analyses. All statistical analyses were performed using R software, version 4.0.3 (R Foundation for Statistical Computing, 2020). Statistical significance was set at a p-value < 0.05.
Results
Baseline characteristics and clinical outcomes of the entire cohort
Baseline characteristics and clinical outcomes of all 197 patients treated with either blinatumomab (n = 84) or conventional salvage regimen (n = 113) are summarized in Table 1 and Supplemental Table 1. Median 2 cycles (range, 1–2) of blinatumomab and median 1 cycle (range, 1–3) of conventional chemotherapy were applied, respectively. Regarding disease status at the time of salvage, 71 (36.0%) were primary refractory (initial induction failure), and 126 (64.0%) were relapses after previous chemotherapy (n = 59, 30.0%) or allo-HCT (n = 67, 34.0%). Among the 126 relapsed patients, the median duration of CR was 7.9 months (range, 1.5–147.3), and 85 patients (79.2%) had a CR duration shorter than 12 months (59 after chemotherapy, 67 after previous allo-HCT). Overall, 132 (67.0%) achieved CR but 19 (14.4%) of them relapsed during the course of therapy. Among the patients in CR, 72 were available with MRD results. MRD negativity was achieved in 30 (41.7%), which was 65.2% in blinatumomab group and 38.5% in conventional salvage group (p = 0.028). Regimen-related mortality was 20.8%; all but one was after conventional chemotherapy. Finally, 118 (59.9%) proceeded to allo-HCT. After a median follow-up duration of 36.5 months (range, 6.2–131.2), 3-year OS was 25.9% [95% confidence interval [CI], 19.3–33.0] and NRM was 35.9% (95% CI, 28.9–43.0). Among the patients achieving CR, estimated 3-year CIR was 36.9% (95% CI, 27.8–46.1) and 3-year DFS was 30.8% (95% CI, 21.9–40.1).
Baseline characteristics and outcomes of the entire cohort (n = 197).

BM, bone marrow; BMR, bone marrow relapse; CR, complete remission; EMR, extramedullary relapse; HCT, hematopoietic cell transplantation; MRD, minimal residual disease.
Propensity score–matched cohort and response to treatments
We created propensity score–matched cohorts assigning 52 patients to each salvage group. Between the two groups, the proportions of patients with adjusted parameters were identical (Table 2). Comparative clinical outcomes for the two matched cohorts are shown in Table 3. During the period after conventional chemotherapy, 21 patients (40.4%) died due to regimen-related hematological toxicity – most involved septic shock followed by multiorgan failure, while only one patient (1.9%) died during blinatumomab cycles. The CR rate was 80.8% after blinatumomab, which was significantly higher than the 53.8% seen in the conventional group (p = 0.006). MRD results were available in 35 patients in blinatumomab and 10 in conventional chemotherapy. MRD negativity was achieved in 68.6% in blinatumomab while in 40.0% in conventional group. Overall, 42 patients (80.8%) proceeded to allo-HCT in the blinatumomab group. Among 28 patients who achieved CR after conventional chemotherapy, 4 relapsed, and 24 patients (46.2%) proceeded to allo-HCT. The results were consistent across first-line and second-line subgroups.
Baseline characteristics of the two matched cohort.
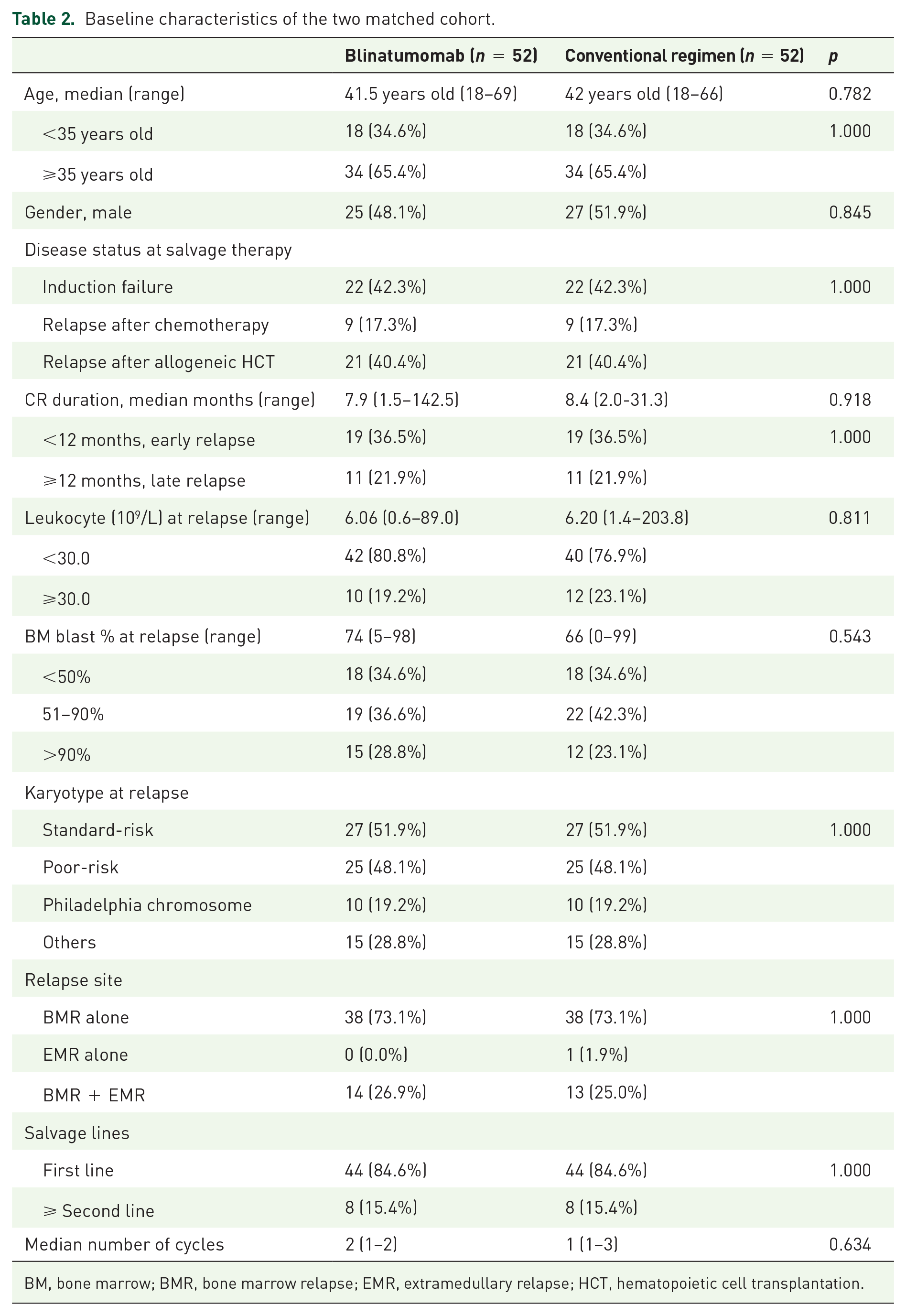
BM, bone marrow; BMR, bone marrow relapse; EMR, extramedullary relapse; HCT, hematopoietic cell transplantation.
Clinical outcomes according to two matched cohort.

CR, complete remission; HCT, hematopoietic cell transplantation; MRD, minimal residual disease.
Survival outcomes after matched cohort analysis
At the time of analysis, 24 patients (46.2%) died (12 due to leukemia progression, 11 due to transplantation-related NRM, and 1 due to blinatumomab-related NRM) in the blinatumomab group, while in the conventional group, 46 patients (88.5%) died (p < 0.001; 19 due to leukemia progression, 6 due to transplantation-related NRM, and 21 due to chemotherapy-related NRM). As a result, the estimated 3-year NRM of the conventional group was 51.9%, which was significantly higher than the 30.3% seen in the blinatumomab (p = 0.004; Figure 1(a)). However, among patients achieving CR, the 3-year CIR rate was not significantly different between the blinatumomab and conventional groups (46.9% versus 50.0%, respectively; p = 0.419; Figure 1(b)). To date, 28 patients (53.8%) in the blinatumomab group and 6 (11.5%) in the conventional group remained alive, and the estimated 3-year OS rate for patients treated with blinatumomab was 33.2% (median, 26.3 months), which was significantly higher than the 15.4% (median, 8.2 months) of the conventional group (p < 0.001; Figure 1(c)). Among patients who achieved CR, the 3-year DFS rates in the blinatumomab and conventional groups were 24.7% (median, 17.0 months) and 21.4% (median, 9.1 months), respectively (p = 0.140; Figure 1(d)). In multivariate analysis (Table 4), early relapse with CR duration < 12 months was associated with a higher CIR rate [hazard ratio (HR) = 2.25; 95% CI, 1.07–4.75; p = 0.033], while members of the conventional group (HR = 2.82; 95% CI, 1.48–5.38; p = 0.001) and advanced-line salvage (HR = 2.19; 95% CI, 1.09–4.39, p = 0.027) had higher NRM rates. As a result, early relapse with a CR duration < 12 months (HR = 1.63; 95% CI, 0.99–2.66; p = 0.053) and the conventional group (HR = 2.82; 95% CI, 1.69–4.72; p < 0.001) showed significantly inferior 3-year OS in this study.
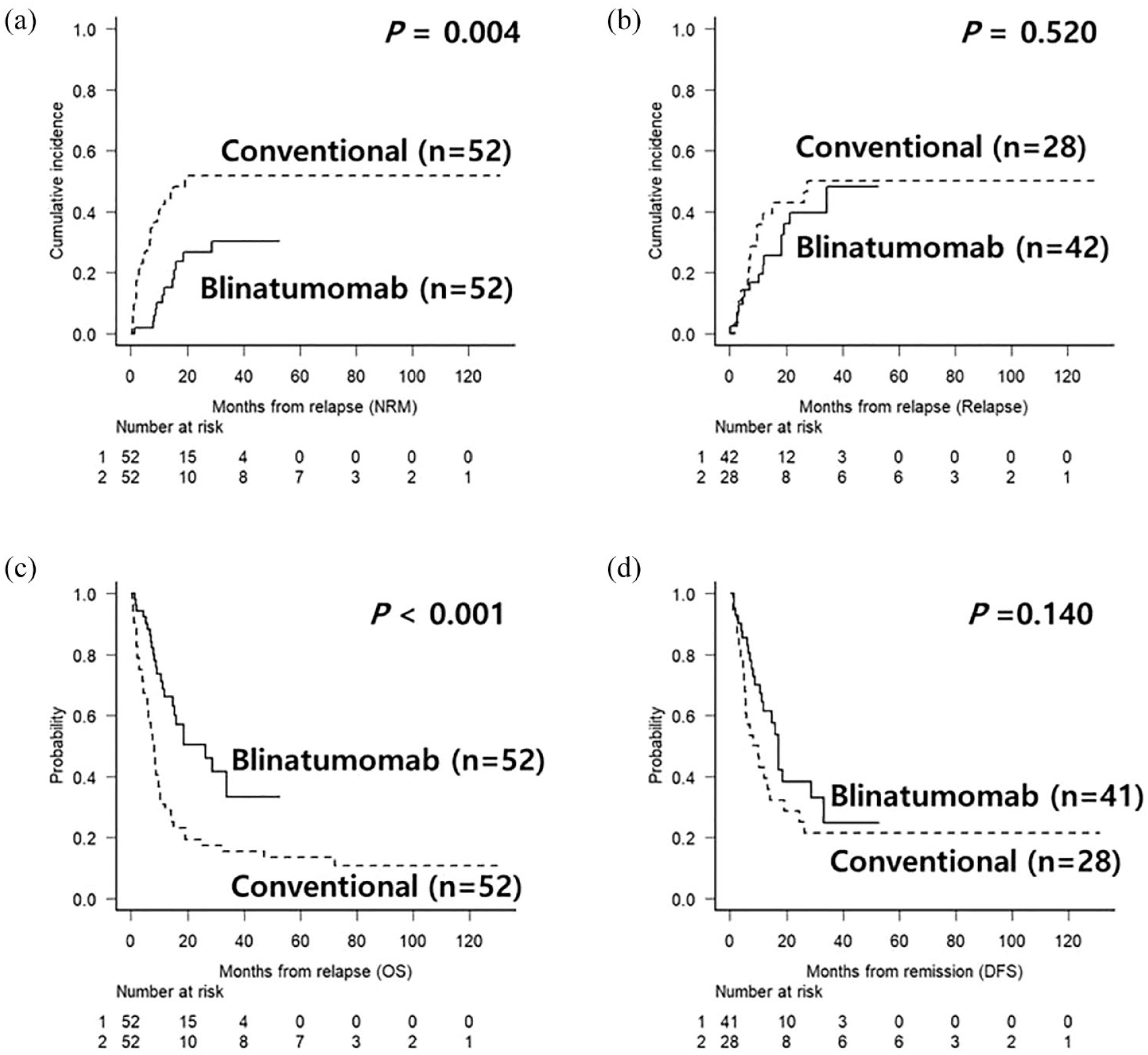
Clinical outcomes after salvage therapy using blinatumomab versus conventional salvage regimen. (a) Non-relapse mortality. (b) Cumulative incidence of relapse after remission achievement. (c) Overall survival. (d) Disease free survival after remission achievement.
Uni- and multivariate analysis to identify affecting factors for outcomes of patients with relapsed or refractory ALL.

CI, confidence interval; CIR, cumulative incidence of relapse; CR, complete remission; HCT, hematopoietic cell transplantation; HR, hazard ratio; NRM, non-relapse mortality; OS, overall survival.
Subgroup analysis and toxicity profile
We also performed subgroup analyses according to age, salvage line, Ph-chromosome, and allo-HCT. Our data showed superior 3-year OS rates in both the blinatumomab subgroup of patients <35 years (57.1% versus 16.7%; p = 0.013, Figure 2(a)) and the subgroup of patients ⩾35 years (21.8% versus 14.7%; p = 0.005, Figure 2(b)) compared with conventional chemotherapy. In the first-line salvage subgroup analysis, the 3-year OS rate was 33.5% after blinatumomab and 18.2% after conventional chemotherapy (p = 0.002; Figure 2(c)), and it was 43.8% after blinatumomab and 0.0% after conventional chemotherapy (p = 0.004) in the advanced-line subgroup analysis (Figure 2(d)). The results were also valid in both Ph-positive ALL (42.2% versus 10.0%; p = 0.017) and Ph-negative ALL (34.3% versus 16.7%; p = 0.002) subgroups. In the subgroup of patients who underwent allo-HCT, the 3-year OS rate was 37.5% (median, 23.7 months) after blinatumomab and 33.3% (median, 8.6 months) after conventional chemotherapy (p = 0.189). The 3-year post-allo-HCT CIR and NRM rate after blinatumomab versus conventional chemotherapy was 31.6% versus 45.8% (p = 0.088) and 25.0% versus 33.8% (p = 0.543). The most frequent and severe adverse events in both salvage groups were hematologic toxicities such as neutropenia and thrombocytopenia. Hematological toxicities were more profound after conventional chemotherapy; all in the group suffered from grade IV neutropenia, 92.9% experienced neutropenic fever, and 38.0% presented with septic shock followed by multiorgan failure. In the blinatumomab group, febrile neutropenia was observed in 59.5% and grade IV neutropenia was observed in 15.4% of patients. Fever after blinatumomab was confused with low-grade CRS, when it occurred at an earlier period after blinatumomab infusion. Overall, we recorded CRS in 23.8% of patients, but most were grade II and safely manageable, and grade III CRS was observed in 5.9% of patients. Blinatumomab-induced neurologic events occurred in 11.9% of patients and grade III or IV events were observed in 7.1% of patients. Detailed symptoms associated with neurologic events included tremors, confusion, ataxia, somnolence, and loss of consciousness with stroke-like features.

Subgroup analysis of OS between blinatumomab versus conventional salvage regimen. (a) OS in younger age subgroup. (b) OS in older age subgroup. (c) OS in first-line salvage group. (d) OS in advanced-line salvage group.
Discussion
Since blinatumomab has been available for R/R BCP-ALL patients, CR rates have improved, and more patients have proceeded to allo-HCT. In our previous analysis of treatment outcomes of blinatumomab as a first-line salvage, a persistent CR was achieved in 21 of 32 patients (65.6%) and their MRD response was 75%, leading to allo-HCT in 20 patients (62.5%). 21 Although the follow-up duration was relatively brief, our previous study provided evidence of early real-world experience with blinatumomab as a first-line salvage. However, it is now important to determine long-term survival outcomes and conduct real-world comparative analyses with conventional chemotherapy.
In this study, we examined long-term treatment outcomes for blinatumomab and compared the results with historical chemotherapy. The use of a historical comparative data set is accompanied by concerns about potential bias related to selection, misclassification, and confounding factors. We first identified and compared outcomes for 84 patients treated with blinatumomab with outcomes for 113 patients treated with conventional salvage therapy. The age distribution and proportions of patients with early relapse and poor-risk karyotypes were significantly different between the two groups. To reduce the risk of selection bias and provide a more reliable comparison, we conducted a propensity score–matched cohort analysis by matching the proportion of patients ⩾ 35 years of age and those with a poor-risk karyotype, Ph-chromosome, primary disease status such as induction failure and post-HCT relapse, CR duration < 12 months, and first-line salvage. Nevertheless, because the two comparator groups reflect different eras of salvage therapy, it remains challenging to address the unidentified time-dependent elements, as a conventional regimen was used until late 2016, while blinatumomab was used in Ph-negative ALL since late 2016 and in Ph-positive ALL since 2019.
Previously, the phase 3 clinical trial data for blinatumomab were compared with historical data of standard of care by propensity-score matching for the important parameters. The results differed significantly between the two treatment groups in R/R BCP-ALL patients (time to relapse, age distribution, and salvage line) 18 and in BCP-ALL patients with MRD (age, gender, cytogenetics, leukocyte count, and MRD level). 19 They used weighting procedures to account for differences in the distribution of several prognostic factors that varied across the calendar period, possibly reducing the time-dependent effects. The R/R BCP-ALL data after blinatumomab treatment showed a superior response rate (49.3%) and 1-year OS rate (39.0%), which were approximately double those of the historical data (a response rate of 26.7% and 1-year OS rate of 17.2%). 18 Our data, which included a longer follow-up duration compared with previous reports, also revealed a superior 3-year OS rate after blinatumomab (33.2% versus 15.4%). The CR rate was 80.8% in the blinatumomab group, which was significantly higher than the 53.8% seen in the conventional salvage group. MRD response was achieved in 68.6% in patients with blinatumomab-induced CR while 40.0% in chemotherapy-induced CR, although not all patients were available with MRD results. Our current study revealed blinatumomab to be associated with a higher CR rate, higher MRD response rate, significantly lower regimen-related mortality, and superior survival outcomes compared with conventional chemotherapy, which is consistent with previous findings.
From a different point of view, the CR rate (53.8%) after conventional chemotherapy was higher than what we expected (~30%) based on previous reports.5,6,18 In addition, in patients who achieved CR after conventional chemotherapy, no inferior outcomes were observed compared to blinatumomab in terms of CIR, DFS, and post–allo-HCT OS. Nevertheless, most patients in the conventional group suffered from a serious infection or septic shock due to severe neutropenia, thrombocytopenia, or symptomatic mucositis. Regimen-related mortality after conventional chemotherapy was very high (40.4%) in this study compared with that of previous clinical trials. 15 In contrast, just a few serious adverse events were observed after blinatumomab except for some transient neurological symptoms or grade I or II CRS that subsided soon after appropriate management.
Because just a few real-world studies of blinatumomab have been published,21,33,34 our study might be a useful reference as a real-world comparative data. However, several issues should be addressed. First, survival improvement may be due to blinatumomab retreatment or the use of INO, which supplies another opportunity for safe salvage and bridging to the next allo-HCT. In this study, four patients in the blinatumomab group received INO for post-blinatumomab salvage. We should keep in mind that this comparative study might rather reflect an era of rapid development of novel agents. Next, according to recent long-term survival data in Ph-negative R/R BCP-ALL, 17 we could see the survival outcomes were reduced to less than 20% after 3 years of follow-up. Also in the current study, although 3-year OS after blinatumomab was superior to the conventional group, up to 70% of patients eventually died or relapsed.
Because currently available blinatumomab monotherapy followed by allo-HCT continues to show poor long-term OS, more effective treatment strategies are required. Some recent trials suggest that combining blinatumomab or INO with low-intensity chemotherapy shows promising survival benefits for patients with R/R BCP-ALL and in elderly patients.35,36 In addition, blinatumomab is regarded as more beneficial when administered as first-line salvage.37,38 We expect the effect of blinatumomab could be maximized if it is used as early as possible as a frontline therapy combined with reduced toxicity chemotherapy with other targeted agents such as INO or tyrosine kinase inhibitors. Foa et al. 39 conducted a phase 2 study of a chemotherapy-free regimen of dasatinib plus blinatumomab in newly diagnosed Ph-positive ALL patients. They reported that the CR rate was 98%, with only one death during the induction-consolidation period and an estimated 18-month OS rate of 95% after a chemotherapy-free regimen followed by allo-HCT in high-risk patients. The outcome was promising regardless of age, as indicated by the low mortality.
We compared long-term survival outcomes in patients with R/R BCP-ALL treated with blinatumomab against the results of conventional chemotherapy. We attempted to reduce the risk of bias associated with a comparative study that uses historical data and different treatment periods by conducting a propensity score–matched cohort analysis, but this study still has limitation of MRD data lacking and as a single center data. In conclusion, our data could show that blinatumomab was associated with favorable outcomes compared with patients treated with conventional therapies, but we are still realizing poor survival outcomes of R/R BCP-ALL even after successful bridging to allo-HCT. Newer and more sophisticated approaches for adult ALL will be required to improve survival rates.
Supplemental Material
sj-docx-1-tah-10.1177_20406207231154713 – Supplemental material for Superior survival outcome of blinatumomab compared with conventional chemotherapy for adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia: a propensity score–matched cohort analysis
Supplemental material, sj-docx-1-tah-10.1177_20406207231154713 for Superior survival outcome of blinatumomab compared with conventional chemotherapy for adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia: a propensity score–matched cohort analysis by Jae-Ho Yoon, Daehun Kwag, Jong-Hyuk Lee, Gi June Min, Sung-Soo Park, Silvia Park, Sung-Eun Lee, Byung-Sik Cho, Ki-Seong Eom, Yoo-Jin Kim, Hee-Je Kim, Chang-Ki Min, Seok-Goo Cho, Jong Wook Lee and Seok Lee in Therapeutic Advances in Hematology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.