
Abstract
Background:
ATP-competitive tyrosine kinase inhibitors (TKIs) are the current standard of care for patients with chronic phase-chronic myeloid leukemia (CP-CML) in the first-line and second-line (2 L) setting. Treatment after 2 L is not clearly established.
Objective:
The objective of this study was to summarize the available evidence to compare the efficacy and safety of interventions in the treatment of CP-CML patients who had received ⩾2 prior TKIs.
Design:
A systematic literature review was performed.
Data source and methods:
A systematic literature review (SLR) of studies published until May 2021, reporting clinical outcomes in adult patients with CP-CML who had received ⩾ 2 prior TKIs was performed. Studies were identified through the database searches via Ovid platform (Embase, MEDLINE Epub Ahead of Print, In-Process and Other Non-Indexed Citations, and Cochrane Central Register of Controlled Trials), the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP), bibliographic search of relevant reviews, and proceedings from the previous 3 years of the key conferences in the field of oncology.
Results:
Our search identified 38 relevant studies. Among the identified studies of the current third-line treatments, the major molecular response (MMR) rate for ponatinib was 19.0–66.7%, 23.3–25.5% for asciminib, 19.2% for omacetaxine, and 13.2% for bosutinib at 6 months. The complete cytogenetic response (CCyR) rate was 21.4–64.8% for ponatinib, 38.7–40.8% for asciminib, 18–24.2% for bosutinib, and 16.1% for omacetaxine at 6 months.
Conclusion:
The findings from current SLR demonstrated the lack of data for patients with CML treated with ⩾2 TKIs. TKIs such as asciminib, ponatinib, and bosutinib are valid options for those patients. Further research is needed to identify the best treatment option for patients with CML receiving later lines of therapy.
Introduction
Chronic myeloid leukemia (CML) is a rare type of myeloproliferative disorder of blood stem cells. 1 It is characterized by the reciprocal translocation between chromosomes 9 and 22, forming an abnormal chromosome (the Philadelphia chromosome), which results in the generation of oncoproteins from the BCR-ABL1 fusion gene, driving the pathogenesis of CML.1,2 The identified risk factors for CML include exposure to ionizing radiation, older age, and male gender.3,4 Untreated CML progresses from the chronic phase (CP) to the advanced phase, which comprises the accelerated phase (AP) and the blastic phase (BP).5,6 CML represents approximately 15% of all new cases of leukemia in the United States, with an annual incidence of 1.9 per 100,000 people.3,7 In Europe, the annual incidence of CML is 0.7–1.0 per 100,000 people, with the median age of diagnosis being 57–60 years. 8 According to the American Cancer Society, approximately 9110 new cases of CML were estimated to occur in the United States in 2021, with approximately 1220 deaths due to CML. 7
ATP-competitive tyrosine kinase inhibitors (TKIs) are the current standard of care for patients with chronic phase-chronic myeloid leukemia (CP-CML), particularly in the first-line (1 L) and second-line (2 L) setting.5,6,9 The National Comprehensive Cancer Network (NCCN) and European LeukemiaNet (ELN) guidelines recommend the use of first-generation (imatinib) or second-generation (2G; nilotinib, dasatinib, or bosutinib) TKIs as the frontline therapy.5,6,9 Almost half of all imatinib-treated patients develop resistance or intolerance to treatment, and among them 30–40% of patients treated with 2G TKIs require a switch within 5 years of treatment. 1 Treatment sequence after 2 L is not clearly established as TKIs are often cycled and patients have limited options on account of resistance or intolerance to treatments. 1 Ponatinib, a third-generation (3G) TKI, is approved and recommended for the treatment of CP, AP, or BP-CML patients who are resistant or intolerant to prior TKIs.5,6,9 Bosutinib, a 2G TKI is also approved to treat patients who had resistance or intolerance to prior ⩾ 2 TKI.10,11
Thus, the objective of this SLR was to systematically identify and summarize the available evidence in the treatment of CP-CML patients who had received ⩾2 prior TKIs.
Methods
This SLR was conducted in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 12 and the National Institute for Health and Care Excellence (NICE) 13 guidelines.
Study inclusion criteria
The population of interest was that of adult patients with CP-CML who had received ⩾2 TKIs prior to study enrollment. Studies with a mixture of CP-CML and AP-CML patients or with a mixture of patients with <2 prior TKIs and ⩾2 prior TKIs were also considered for inclusion if they had reported outcomes of interest for subgroups where ⩾80% of patients matched the target population. Interventions of interest included omacetaxine, olverembatinib, allogeneic stem cell transplantation (allo-SCT), hydroxycarbamide, radotinib, and asciminib, as well as TKIs recommended in the NCCN, European Society for Medical Oncology (ESMO), and ELN clinical practice guidelines, either as monotherapy or in combination with other treatments.5,6,9,14–18 Controlled and non-controlled clinical trials, as well as prospective and retrospective observational studies, were included in this SLR. Only English-language publications were included, and no timeframe restriction was applied. Detailed eligibility criteria are presented in Supplementary Table S1.
Literature search
Comprehensive searches from the date of inception until May 2021 were conducted for the following databases using the Ovid platform: Embase, MEDLINE Epub Ahead of Print, In-Process and Other Non-Indexed Citations, and Cochrane Central Register of Controlled Trials (CENTRAL) using the following search terms: ‘chronic myeloid leukemia’ AND (asciminib OR nilotinib OR dasatinib OR imatinib OR bosutinib OR ponatinib OR hydroxycarbamide OR omacetaxine OR ‘stem cell transplant’ OR olverembatinib OR ‘best supportive care’). Supplementary Tables S2–S4 provide details of the search strategy used. A bibliographic search of relevant reviews was also conducted to identify additional studies. Proceedings from the previous 3 years of the key conferences in the field of oncology were searched for relevant abstracts. To identify any ongoing or completed clinical trials that met the inclusion criteria but did not have results published or publicly available, the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) was also searched.
Study selection and data extraction
Based on the predefined eligibility criteria (presented in Supplementary Table S1), first-level screening of the studies was conducted based on the titles and abstracts, which was followed by second-level screening of the full-text publications. Data (study characteristics, interventions, patient characteristics, and outcomes) from the studies selected after second-level screening were extracted in a predefined extraction grid. Screening and data extraction were performed by two independent reviewers, and any conflicts in the decisions of the two reviewers were resolved by a third independent reviewer. Data for the outcomes of interest were extracted as continuous and dichotomous outcomes. Data from Kaplan–Meier curves and figures were extracted using DigitizeIt.
Outcomes
The following outcomes were extracted: major molecular response (MMR) at any reported time point, defined as a value of ⩽0.1% BCR-ABL1 on the international scale; complete cytogenetic response (CCyR) at any reported time point, defined as a value of 0% Philadelphia chromosome–positive (Ph+) metaphases in the bone marrow; time to MMR or CCyR from the start date of therapy; overall survival (OS) at any reported time point, defined as the time from start of treatment to the date of death; progression-free survival (PFS) at any reported time point, calculated from the start date of therapy to the date of progression or death; event-free survival (EFS) at any reported time point, considered from the date of treatment started to occurrence of any event (i.e. loss of any response, progression to advanced disease phases or switching to any other treatment); and general safety outcomes including any-cause adverse events (AEs) of any grade or grade 3/4, treatment-related AEs of any grade or grade 3/4, serious AEs, treatment discontinuation due to AEs, and treatment-related deaths.19–22 MMR, CCyR, OS, PFS, and EFS were reported as proportion of patients (n, %) achieving the response at different time points. However, time to MMR and CCyR were reported in months.
Assessment of study quality
All included randomized trials were critically appraised for their quality using the Cochrane Collaboration’s Risk of Bias assessment tool. Study-level biases based on six key domains were evaluated: sequence generation; allocation concealment; blinding of participants, personnel, and outcome assessors; incomplete outcome data; selective outcome reporting; and other sources of bias. 23 The results were described using the risk-of-bias summary (i.e. authors’ judgment of each risk of bias for each study). The Newcastle-Ottawa Scale (NOS) risk of bias assessment tool for cohort studies was used to assess the quality of the included single-arm and observational studies to evaluate any bias based on selection of study group, comparability of the groups, and ascertainment of exposure or outcomes. 24
Results
A total of 12,844 potentially relevant publications were retrieved from the database (n = 12,384) and manual searches (n = 460). After the screening process, 75 publications describing 38 studies met the eligibility criteria. Of the 75 identified publications, 31 were full-text publications and 44 were conference abstracts. The main reasons for exclusion included study population not of interest, study designs not of interest (e.g. meta-analyses, case reports, in vivo/in vitro studies, and cost-effectiveness analysis), and ‘other’ reasons (e.g. conference proceedings, summaries, and narrative reviews). The trial flow in the SLR is presented using the PRISMA flow diagram (Figure 1).
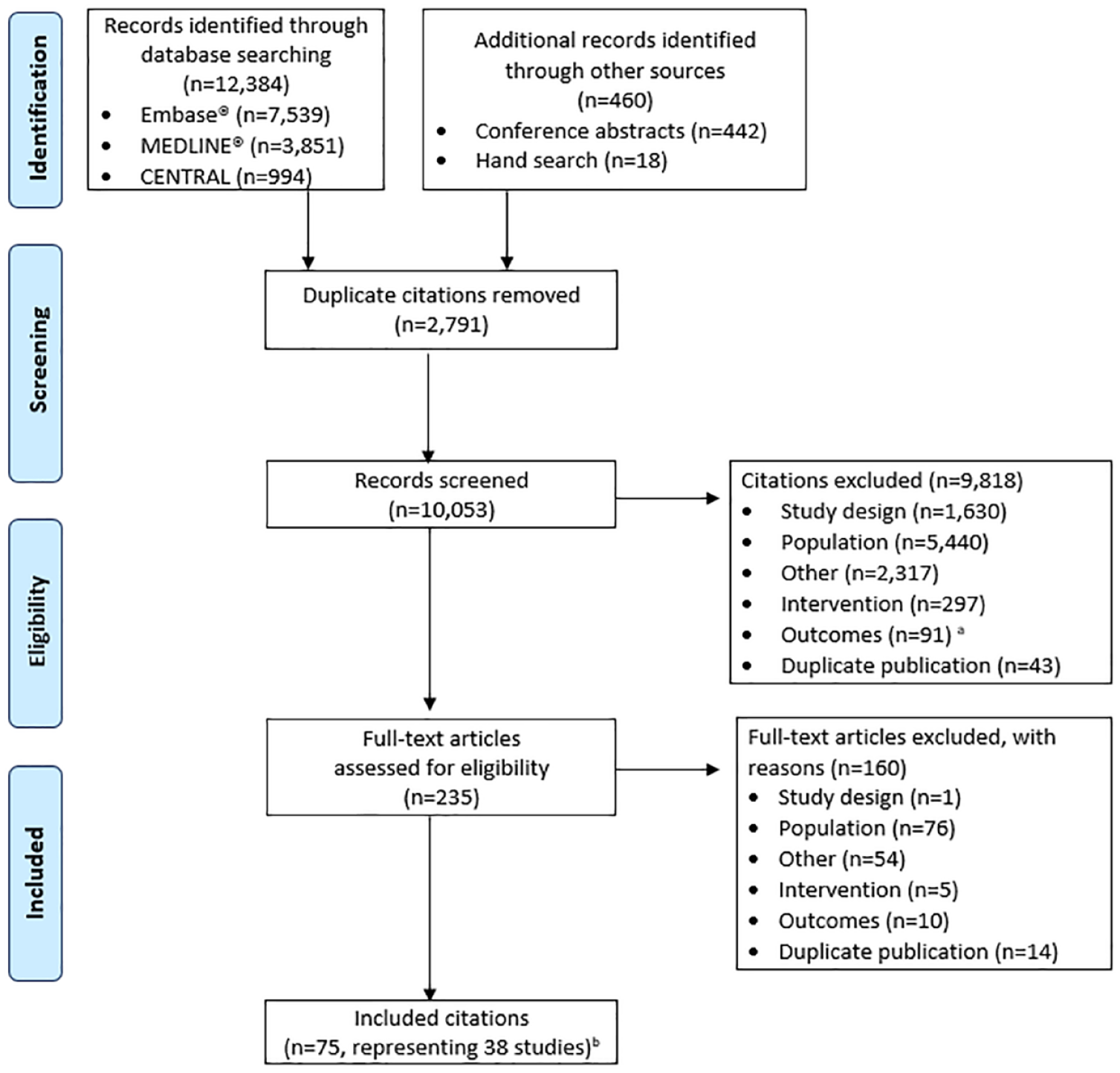
PRISMA flow diagram.
Study characteristics
Of the total 38 included studies, 2 were randomized trials (ASCEMBL and OPTIC), 13 were single-arm clinical trials, and the remaining 23 were observational studies (4 prospective studies, 18 retrospective studies, and 1 prospective and retrospective cohort study). Study and patient characteristics of the included studies are summarized in Supplementary Table S5. ASCEMBL was the only randomized trial that involved a head-to-head comparison of asciminib with bosutinib. 25 The other randomized trial (OPTIC) compared different doses of ponatinib.26,27 Majority of the studies were conducted in multicenter settings (n = 25), while the remaining were conducted at a single center (n = 10) or did not specify the study settings (n = 3). Most of the studies were conducted either in the United States or in a European country (n = 20). The evidence from the identified studies was largely focused on ponatinib (n = 11), followed by bosutinib (n = 8), nilotinib and/or dasatinib (n = 8), asciminib (n = 3), omacetaxine (n = 2), and olverembatinib (n = 2). There was limited evidence for PF-114 and alloSCT, with only one study on each. Few studies (n = 11) evaluated patients receiving different interventions in a single arm.
Quality of studies
Based on the Cochrane Collaboration’s Risk of Bias Tool for randomized trials, the ASCEMBL study was conducted well and had an overall low risk of bias, while the OPTIC trial had an overall unclear risk of bias as loss to follow-up was not reported and all patients were not evaluable for efficacy (Supplementary Table S6). Both studies had a high risk of detection bias by the outcome assessor. The single-arm trials and observational studies performed well on the NOS with a quality score ranging from 3 to 6 stars, with majority of the studies scoring ⩾ 4 stars (Supplementary Table S7).
Evidence on efficacy
Complete cytogenetic response
The CCyR rate was reported in 31 studies. An overview of studies reporting CCyR is summarized in Table 1. The CCyR rate ranged from 16.1% with omacetaxine to 64.8% with ponatinib at 6 months, and the corresponding values at 12 months were 16.2% to as high as 83.9% with bosutinib.28–31 Among the included interventions, the CCyR rates ranged from 38.7% at 6 months to 66% at 10.2 months for asciminib,20,32 16.2% at 12 months to 83.9% at 12 months for bosutinib,30,31 6% at 15 months to 69.6% at 40.8 months for ponatinib,33,34 4% at 19.1 months to 16.1% at 6 months for omacetaxine,28,35 36.8% at 12.8 months to 65.9 at 7.9 months for olverembatinib,36,37 24% at 12 months to 31% at 16 months for nilotinib,19,38 and 11% at 16 months to 46.2% at 12 months for dasatinib.19,39 The median time to CCyR was reported as 4.8 months in a study of ponatinib-treated patients. 40
Overview of response outcomes reported in the included studies.

L, second-line; 3 L, third-line; 4 L, fourth-line; CCyR, complete cytogenetic response; CML, chronic myeloid leukemia; MMR, major molecular response; NR, not reported, OITI, Observational study of Iclusig® (ponatinib) Treatment in patients with CML in Italy; OPTIC, Optimizing Ponatinib Treatment In CML; PACE, Ponatinib Ph+ ALL and CML Evaluation; TOPASE, Therapeutic Observatory of Ponatinib About Safety and Efficacy.
Outcomes reported are for the non-T315I-mutated population.
Evaluable for 31 patients.
Evaluable for 86 patients.
Reported as BCR-ABL1IS ratio ⩽ 1%.
Reported for patients on 3 L treatment, N = 21.
A total of 41 patients were evaluated for MMR.
A total of 133 patients evaluated for CCyR.
From the principal Khoury et al., 21 publication.
Only 12 patients evaluable for CCyR in Tan et al. 39
Outcomes reported for T315I-negative patients.
Reported for 6 patients.
Major molecular response
MMR was reported in 35 studies, and an overview of studies reporting MMR is summarized in Table 1. The MMR rate ranged from 10.5% with omacetaxine to as high as 66.7% with ponatinib at 6 months of follow-up and was 14–35% with ponatinib at 12 months of follow-up.26,27,29,35,42 Among the included interventions, the MMR rates ranged from 23.3% at 6 months to 41% at 10.2 months for asciminib,20,32 13.2% at 6 months to 76.4% at 24 months for bosutinib,25,30 14% at 6 months to 66.7% at 6 months for ponatinib,27,29 10.5–19.2% at 6 months for omacetaxine,28,35 14.7% at 12.8 months to 48.8% at 7.9 months for olverembatinib,36,37,55 13% at 16 months to 33.3% at 12 months for nilotinib,19,22 and 20.8% at 12 months to 33.3% at 16 months for dasatinib.19,39
In the included studies, the overall median time to MMR was approximately 3–9 months for asciminib, 4–6 months for ponatinib, and 3.3 months for bosutinib.20,25,41,56,57 The median time to MMR in patients with CP-CML, regardless of T315I mutation status, was reported to be 2.92 months for asciminib, 3.29 months for bosutinib, and 4 months for ponatinib.25,41 However, specifically in the non-T315I-mutated population, the median time to MMR was 6 months for ponatinib and 8.8 months for asciminib.20,29
Overall survival
OS was reported in 18 studies, and an overview of studies reporting 1- to 5-year rates of OS are summarized in Table 2. The 1-year OS rate ranged from 91% with bosutinib to 100% with ponatinib.21,30,42 The 5-year OS rate ranged from 65% with mixed TKIs (dasatinib, nilotinib, bosutinib, and ponatinib) to 96% with bosutinib.48,58 In the majority of studies, OS was not reached. Among the included interventions, bosutinib reported highest OS at 2 years, 47 ponatinib at 1 year, 42 and dasatinib or nilotinib at 3 years. 49 In the CML-203 study, the median OS in patients treated with omacetaxine was 30.1 months. 35 In the studies where patients treated with asciminib, OS was not reported. Overall, OS rates decreased from 1 to 5 years.
Overview of survival outcomes reported in the included studies.

allo-SCT, allogeneic stem cell transplantation; EFS, event-free survival; OITI, Observational study of Iclusig® (ponatinib) Treatment in patients with CML in Italy; OPTIC, Optimizing Ponatinib Treatment In CML; OS, overall survival; PACE, Ponatinib Ph+ ALL and CML Evaluation; PFS, progression-free survival; TKI, tyrosine kinase inhibitor.
Evaluable for 267 patients.
Evaluable for 41 patients with ⩾ 2 L.
Evaluable for 93 patients.
Evaluable for 91 patients.
Without prior hematologic resistance to TKI therapy.
With prior hematologic resistance to TKI therapy.
Progression-free survival
PFS was reported in eight studies, and the reported 1- to 5-year PFS rates across studies are summarized in Table 2. PFS rates at 1 year ranged from 77% with bosutinib to 87% with ponatinib.21,60 Only two studies reported the 5-year PFS rate (54% with dasatinib or nilotinib and 53% with ponatinib).61,59 Among the included interventions, bosutinib reported highest PFS at 2 years, 57 ponatinib at 3 years, 34 and dasatinib or nilotinib at 5 years. 51 In majority of the studies, PFS was not reached, and the median PFS was reported in three studies, ranging from 7 months for omacetaxine to 45 months for ponatinib.27,28,35
Event-free survival
EFS was reported in seven studies, and the reported 1- to 5-year EFS rates across studies are summarized in Table 2. Only the PACE study reported the EFS rate at 1 year (94%) during and after discontinuation of ponatinib treatment (with a median follow-up of 15 months). 61 Majority of the studies reported 3-year EFS rates ranging from 28.6% to 76.4% with dasatinib/nilotinib.50,58 In patients with prior hematologic resistance to TKI therapy, the 3-year EFS rate was reported as 28.6%, whereas in patients without prior hematologic resistance to TKI therapy it was 64.7%. 50 The 4-year EFS rate was only reported in a study evaluating allo-SCT (66.7%) in patients who were previously treated with imatinib or 2G TKIs. 59 A 5-year EFS rate of 85% was reported with bosutinib 51 and 22% with dasatinib/nilotinib. 59
Evidence on safety
The safety outcomes reported in the included studies are presented in Table 3. Any-cause AEs were reported in all patients (~100%) on bosutinib, olverembatinib, ponatinib, omacetaxine, and asciminib.20,21,25,30,35,37,47,61 Five studies evaluated any-cause AEs of grade 3/4, and the incidence was reported to be the highest among bosutinib-treated patients.20,21,25,30,47 Treatment-related AEs of any grade were reported in all patients (100%) on olverembatinib over the follow-up of 12.8 months, in 88.2% of patients on bosutinib over 14.9 months, in 58% (over 9.2 months) to 63.5% (over 14.9 months) of patients on asciminib, and in 53.6% of patients on ponatinib over 23.7 months.25,32,37,59 The rates of serious AEs were the highest in patients receiving ponatinib (65.5%) over 56.8 months, followed by omacetaxine (58.1%) over 19 months.28,51 Treatment discontinuations due to AEs were 46.3% for nilotinib/dasatinib over 14 months, 3.7% (over 25.2 months) to 26.4% for bosutinib (over 30.4 months), 12% (over 12.9 months) to 22.6% (over 56.8 months) for ponatinib, and 5.8% for asciminib over 14.9 months.21,25,30,31,41,42,48,49,61,62 Treatment-related deaths were reported to be the highest in omacetaxine studies, ranging from 3% to 4% over 19 months.28,35
Reported safety outcomes in the included studies.

L, second-line; 3 L, third-line; AE, adverse event; CML, chronic myeloid leukemia; PACE, Ponatinib Ph+ ALL and CML Evaluation; OITI, Observational study of Iclusig® (ponatinib) Treatment in patients with CML in Italy.
Outcomes reported are for the non-T315I-mutated population.
Reported for patients on 3 L treatment, N = 21.
From the principal Khoury et al., 21 publication.
Reported for all 82 patients, including 14 patients who were in advanced phase.
All patients in the entire any-phase CML population experienced ⩾1 treatment-related AE.
Discussion
This SLR sought to provide a comprehensive overview of the efficacy and safety of treatments in patients with CML who had received ⩾2 prior TKIs. Since most studies evaluated a single intervention, there is a paucity of direct comparative evidence in this patient population. Only two randomized trials, ASCEMBL and OPTIC, compared asciminib to bosutinib and different doses of ponatinib, respectively.
Among all the interventions, ponatinib and asciminib demonstrated higher MMR and CCyR rates at 6 months of follow-up. The median time to MMR in patients with CP-CML, regardless of mutation, was the lowest with asciminib followed by bosutinib and ponatinib. It was observed that OS, PFS, and EFS were not reached for majority of the interventions in the included studies due to short follow-up period. MMR was the most frequently assessed and reported outcome in almost all the studies. MMR is a more convenient and sensitive measurement to detect residual disease than conventional cytogenetics. 62 Furthermore, studies also suggest a significant impact of MMR on the rates of PFS and EFS, making it a suitable outcome for comparison. 62 Hence, MMR may provide a valid option to consider as a surrogate for long-term survival, especially when studies with matured survival data are not available, as observed in the current SLR. 63
Although most CML patients have a near normal life-expectance with the use of TKIs, treatment interruptions associated with AEs and/or lack of response are a known occurrence. 9 Efficacy decreases with each progressive line of therapy. 1 Management of CP-CML after failure of two TKIs poses a clinical challenge. Furthermore, treatment guidelines for such heavily pretreated patients are lacking. 1 There are limited data demonstrating the clinical benefit of switching to a different ATP-competitive TKI in the 3 L setting as sequential use of ATP-competitive TKIs is associated with increased rates of resistance and intolerance resulting in higher rates of disease progression or death. 1 The standard of care beyond 2 L therapy is not well defined by the NCCN and ELN guidelines. The selection of a 3 L TKI may also depend on a patient’s comorbidities, prior AEs, mutation profiles, drug interactions, and compliance issues, and there are limited options, such as ponatinib (also for T315I mutations), bosutinib, omacetaxine and recently approved asciminib for patients with CP-CML with failure after ⩾2 TKIs. 1 Novel treatment options are needed for the patient population that requires treatment in the 3 L setting and beyond. 1 The lack of data is affirmed by the findings of this SLR.
This SLR highlights that the available studies have heterogeneity in the reported outcomes in terms of the definitions of outcomes (e.g. PFS), the time points at which response outcomes were reported, in the inclusion of patients with mutations, and inconsistency in reporting the outcomes separately for the 3 L CP-CML population. These limitations make the comparison of efficacy of the different interventions difficult and not very meaningful, emphasizing the need for an indirect treatment comparison which will help clinicians to decide on the best treatment for patients with CP-CML after failure of ⩾2 TKIs. In the absence of precise guidelines, these data gaps add to the clinical challenge of deciding on the most appropriate treatment options in patients who are intolerant or resistant to 2 L therapy with 2G/3G TKIs. 64
When the literature search was performed, there were no publications on head-to-head comparisons of asciminib with interventions other than bosutinib. Only the ASCEMBL trial compared asciminib with bosutinib in patients treated with >2 prior TKIs. When the ASCEMBL study was designed, the optimal dose of ponatinib was being reassessed in the ongoing OPTIC trial, and its practical use warranted caution and potential avoidance in patients with cardiovascular comorbidities. Although ponatinib would have been the logical comparator considering the target patient population and efficacy of the drug, however, due to certain major safety concerns of ponatinib in ongoing clinical trial the OPTIC, the final dose of ponatinib was being decided by the trial investigators. Therefore, based on best available evidence and feasibility at the time of initiation of ASCEMBL trial, bosutinib appeared to be the best fit among the existing comparative treatments for patients treated with ⩾ 2 prior TKIs and hence was chosen as the comparator treatment to asciminib in the ASCEMBL trial. An unanchored indirect treatment comparison provides an alternative mechanism to assess the relative treatment effect of CML therapies. A matching indirect treatment comparison of interventions for the treatment of patients with CP-CML who have received ⩾2 prior TKIs is the subject of a separate manuscript.
Very few studies evaluated interventions other than TKIs (allo-SCT and omacetaxine), and most of the available evidence suggests TKIs as promising 3 L treatment options in patients with CP-CML, though subsequent 2G TKIs may have limited value after failure of a prior 2G TKI. 64 This observation was further supported by the findings of the study by Garg et al., 19 who followed 48 patients treated successively with three TKIs (starting with imatinib, followed by dasatinib and nilotinib in 2 L or 3 L) and found that while a response was induced in some patients, it was not durable. As cycling of 2G TKIs has limited therapeutic value which creates the need for an early consideration of treating patients with a 3G TKI (ponatinib) or exploring interventions with novel mechanisms of action, especially for patients showing resistance to 2G TKIs in both the 1 L and 2 L of therapy. Ponatinib is associated with significant cardiovascular side effects. However, these side effects can be partially mitigated with lowering the dose as soon as patients achieve BCR:ABL1 level < 1% based on the OPTIC trial data.
Bosutinib trials have indicated a risk of gastrointestinal disorders, including diarrhea, abdominal pain, and nausea, which impacted the quality of life.10,11 Olverembatinib was efficacious with manageable treatment-related AEs including thrombocytopenia, anemia, leukopenia, and neutropenia in heavily TKI-pretreated patients with CP-CML. 36 Dasatinib and nilotinib as 3 L therapy in patients with CP-CML had shown transient response along with substantial discontinuation rate due to toxicity and disease transformation. 49 As recommended by ELN, TKIs can be cardiotoxic and should be used with caution in patients with heart failure. Nilotinib has been reported to be associated with arterial pathology, both peripheral and coronary, whereas dasatinib has been reported to be associated with pleura and lung complications.5,65 Asciminib, the first Specifically Targeting the ABL Myristoyl Pocket (STAMP) inhibitor, appeared to be efficacious and safe therapeutic option in patients without previous exposure to ponatinib. However, the frequency of arterial-occlusive events was relatively high in asciminib treated patients as compared with bosutinib-treated patients.66,67 Another study conducted by Hughes et al. 20 evaluated patients with CML who were resistant to or had unacceptable side effects from ponatinib and reported achieving MMR with asciminib. The interim results of the ongoing ASCEMBL trial show that asciminib is associated with cytopenias and increased lipase. In addition, it was associated with a very low rate of treatment discontinuation due to AEs, making it a promising novel drug. 25
The main strengths of this SLR include a robust search strategy for a structured literature search, including data from conference proceedings of previous 3 years, and an assessment of the methodological quality of the included articles by two separate individuals. However, the evidence retrieved in the current review has a few limitations. First, only English-language publications were included, which may restrict a wholesome review, albeit the majority of articles are published in English. A high number of conference abstracts (n = 44) were included in this SLR, which ensured inclusion of the most recent evidence. Furthermore, despite the predefined eligibility criteria for inclusion of studies, a large amount of heterogeneity was observed among the included studies owing to differences in the number and nature of prior TKIs received by the patients, baseline T315I mutation status, and cytogenetic response status. Paucity of randomized trials was another limitation of this SLR. Considering CP-CML is a chronic disease requiring potentially lifelong treatment, follow-up data for longer periods are required to determine the long-term survival outcomes; however, some of the studies reported only the short-term follow-up data owing to early termination or ongoing status of the trial.
These limitations also emphasize the need for statistical analytical approaches for estimating the comparative efficacy of different interventions, which would account for the underlying differences between the studies. Despite these limitations, the current SLR provides a comprehensive overview of the evidence on currently available and novel treatment options for CML patients in later lines of therapy. This may help clinicians and decision-makers assess the feasibility of performing further analytical comparisons between interventions relevant to the target population.
Conclusion
The findings from the current SLR indicate that evidence comparing 3 L treatments is limited. In the absence of matured survival data, MMR may provide a valid option as a surrogate outcome for long-term survival assessment. TKIs, such as ponatinib, asciminib, or bosutinib, are valid options for patients with CP-CML previously treated with ⩾ 2 TKIs. Further research to identify the best approach for treating those patients is warranted, including large-scale clinical trials or registries with longer follow-up periods.
Supplemental Material
sj-docx-1-tah-10.1177_20406207221150305 – Supplemental material for Therapy for patients with chronic phase-chronic myeloid leukemia previously treated with ≽2 tyrosine kinase inhibitors: a systematic literature review
Supplemental material, sj-docx-1-tah-10.1177_20406207221150305 for Therapy for patients with chronic phase-chronic myeloid leukemia previously treated with ≽2 tyrosine kinase inhibitors: a systematic literature review by Ehab Atallah, Lovneet Saini, Rodrigo Maegawa, Tanvi Rajput, Regina Corbin and Ricardo Viana in Therapeutic Advances in Hematology
Footnotes
Acknowledgements
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.