
Abstract
Introduction:
Azacitidine (AZA) either single-agent or with donor lymphocytes infusions (DLI) has been used as a salvage treatment for acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS) relapsing after allogeneic hematopoietic stem cell transplantation (HSCT). To date, the majority of data come from patients relapsed after HSCT from full-matched donors.
Methods:
We report a multicenter, collaborative, retrospective analysis of 71 patients with hematologic (n = 40, 56%) and molecular relapse (n = 31, 44%) of myeloid neoplasms after HSCT from alternative donors (mismatched unrelated, n = 39, 55%; haploidentical, n = 29, 41%) consecutively treated at three European centers with AZA ± DLI.
Results:
Median time from HSCT to relapse was 9 months. Additional DLI were given to 33 patients (46%). After a median of four cycles, overall response rate (ORR) was 49% and complete response (CR) rate was 38%. CR lasted for a median of 17 months (range 5–89 months). Median follow-up in the entire cohort was 11 months (range 1–115 months). Event-free survival (EFS) and overall survival (OS) at 1 year were 26% and 53%, respectively. Treatment of molecular relapse granted higher CR rate (65% versus 15%; p = 0.0001), 1-year EFS (43% versus 13%; p = 0.006), and 1-year OS (79% versus 34%; p < 0.001) compared to hematologic relapses. Addition of DLI resulted in significantly higher responses and longer 1-year EFS and OS (Mantel–Byar test, p = 0.004 and p = 0.002, respectively). When applied to our cohort, the APSS-R score confirmed its ability to stratify patients into distinct prognostic groups with significantly different response rates (p = 0.0005) and survival (p < 0.0001). Treatment was well tolerated, with the incidence of late acute and chronic graft-versus-host disease of 27% and 18%, respectively.
Conclusion:
AZA ± DLI proved feasible and effective in AML and MDS relapsing after HSCT from alternative donors. Despite modest efficacy among hematologic relapses, pre-emptive treatment with AZA ± DLI fared better in molecular relapse. Additional DLI contributed to improving efficacy and ensuring longer survival.
Keywords
Introduction
Allogeneic hematopoietic stem cell transplantation (HSCT) still represents the only potentially curative treatment option for the majority of patients with acute myeloid leukemia (AML) and high-risk myelodysplastic syndromes/myeloproliferative neoplasms (MDS/MPN). Over the last decades, the outcome of HSCT has progressively improved, due to both advances in transplantation techniques and supportive care.1,2 Nonetheless, the incidence of disease relapse has largely remained unchanged and still represents the major cause of treatment failure. 3 Overall, about 30% of patients undergoing HSCT for AML and MDS will finally relapse, although rates up to 80% are reported depending on disease, patient, and transplantation features.3–7 The prognosis of relapsed patients remains poor. After different salvage treatments, such as intensive chemotherapy (IC), donor lymphocytes infusions (DLI), or second HSCT, complete response (CR) is obtained only in about 30% of patients and fewer than 20% achieves long-term outcomes.3–7 Interestingly, long-term survival appeared to rely mainly on the achievement of CR with cytoreductive therapies, followed by immunological consolidation with either DLI or subsequent HSCT.5–8 However, IC are burdened by severe toxicities, representing a major limit for less fit and heavily pre-treated patients, especially in the early post-transplantation period.
The hypomethylating agents (HMA), azacitidine (AZA), and decitabine either single-agent or in combination with DLI have been increasingly used in last years as salvage treatment for AML and MDS relapsing after HSCT.9–31 The rationale relies on both anti-leukemic and immunomodulating effects. 32 HMA have shown to induce the upregulation of several leukemia-associated and minor-histocompatibility antigens that were previously epigenetically silenced, and of HLA class-I, HLA class-II, and costimulatory molecules, and to increase the responses of tumor-specific CD8 + T cells.33–43 AZA is also reported to upregulate inhibitory pathways and to induce the expansion of regulatory T cells.44–47 Despite potentially hampering tumor-specific T cells alloreactivity, immunoregulatory properties might in part prevent or attenuate graft-versus-host disease (GvHD) in the post-transplantation setting.48,49 HMA also showed lower toxicity compared to IC. Focusing on AZA, the majority of data come from retrospective studies and four non-randomized prospective trials. Despite heterogeneity, the most relevant studies showed tolerability and efficacy, with response rates of 15–50% in hematologic relapses and 27–67% in case of pre-emptive therapy for molecular relapse. Overall survival (OS) at 2 years was 12–54% in the former group and 25–69% in the latter group (Table 1).9–26,31
Retrospective and prospective studies investigating AZA ± DLI as a treatment of post-transplantation relapse.

AZA, azacitidine; CR, complete response; DLI, donor lymphocytes infusions; GvHD, graft-versus-host disease; Haplo, haploidentical donor; MAC, myeloablative conditioning regimen; MMUD, mismatched unrelated donor; Molec, molecular; Morph, morphological; MSD, matched sibling donor; MUD, matched unrelated donor; ORR, overall response rate; OS, overall survival; Props, prospective; Pts, patients; Retr, retrospective.
Notably, the patients analyzed till now had mainly received HSCT from fully matched sibling donors (MSD) and matched unrelated donors (MUD), while few mismatched unrelated donors (MMUD) and haploidentical donors (haplo) have been reported, without specific subgroup analysis. Therefore, less is known about AZA ± DLI after HSCT from alternative donors, where HLA mismatches could represent a matter of concern. 50 In this setting, immunomodulating effects of both AZA and DLI could elicit, besides the expected graft-versus-leukemia effect, a potentially severe and life-threatening GvHD.
We report a multicenter, collaborative, retrospective analysis of 71 patients with AML and MDS/MPN relapsed after HSCT from alternative donors and consecutively treated with AZA ± DLI. The aim of the study is to evaluate efficacy and feasibility of treatment to identify factor predictive of response and survival and to compare results with the literature.
Methods
Study design
From December 2009 to July 2019, 71 patients were consecutively treated with AZA ± DLI for relapse of AML or high-risk MDS/MPN after HSCT from alternative donors. Alternative donors included MMUD (unrelated donor with maximum 1 allelic/antigenic mismatch at either HLA-A, -B, -C, -DRB1 or -DQB1 locus), family haploidentical (sibling or other relative sharing only one HLA-haplotype with recipient) and unrelated umbilical cord blood (CBU). Patients were treated at three different European centers: San Raffaele Scientific Institute in Milan (Italy), University Hospital Carl Gustav Carus in Dresden (Germany), and University Hospital in Duesseldorf (Germany).
According to institutional policies, the indication for treatment with AZA was either hematologic or molecular relapse post-HSCT not eligible to clinical trials and further IC because of general condition and previous refractoriness. AZA was given as first salvage treatment; patients receiving additional anti-leukemic agents other than DLI and those who received maintenance therapy prior to relapse were excluded. Hematologic relapse was defined as either bone marrow (BM) blast count ⩾ 5%, appearance of blasts in peripheral blood (PB) or extramedullary relapse. Molecular relapse was defined as recurrence or progressive increase in disease markers after HSCT, without evidence of hematologic relapse. Methods for the detection of measurable residual disease (MRD) were multiparameter flow cytometry (MFC), real-time quantitative polymerase chain reaction (RT-qPCR) for known mutations (e.g. NPM1 gene), cytogenetical, and fluorescent in situ hybridization (FISH) analysis; in the absence of disease-specific markers, either a WT1 mRNA assay or a decrease in donor chimerism was adopted as a marker of impending relapse (see Supplemental data). The schedules of AZA were either 32 mg/m2 days 1–5 every 28 days or 75 mg/m2 days 1–7 every 28 days. DLI were generally given from the second cycle of AZA, every two cycles and at escalating dose starting from 1 × 105 CD3 + /Kg in haplo and from 1 × 106 CD3 + /Kg in MMUD, as per institutional guidelines. Both AZA dosage and indication to DLI relied on clinical–biological characteristics of patients, features of disease, type of HSCT, and availability of the donor. All patients gave informed consent for treatment with AZA ± DLI. Patients were treated according to current institutional programs on written informed consent for transplantation procedures, biological sampling and use of medical records for research. Patients’ date were de-identified and anonymized. The reporting of this study conforms to the STROBE statement. 51
Response criteria
CR to treatment was defined as BM blasts < 5% in the absence of both circulating blasts and extramedullary disease, but hematological reconstitution was not required for CR, as factors other than underlying disease (e.g. viral infections, GvHD, or drugs) could contribute to cytopenia in the post-transplantation period. For patients in molecular relapse, disappearance of disease markers was defined as CR MRD-negative, whereas persistence was defined as CR MRD-positive. Partial response (PR) was defined as either decrease in BM blast to 5–25% or decrease in pretreatment BM blast by at least 50%. Progressive disease (PD) was defined as either increase in BM/PB blast percentage or new extramedullary disease during treatment, whereas stable disease (SD) as absence of criteria for CR, PR, and SD. 52
Time to response was calculated from the first day of AZA until best response. OS was defined as the time from the first day of AZA until death by any cause or last follow-up. Patients who received a subsequent HSCT were censored at that date. Event-free survival (EFS) was defined as an interval from AZA administration to either relapse or progression or death in remission (whichever came first). The intensity of conditioning regimens was defined according to Bacigalupo et al. 53 HCT-comorbidity index (HCT-CI) and disease risk index (DRI) were defined according to Sorror et al. 54 and Armand et al., 55 respectively. Acute and chronic GvHD were classified according to criteria by Harris et al. and NIH 2014 consensus conference, respectively.56,57 Adverse events (AE) were graded according to CTC-AE v5.0.
Statistics
Continuous variables were summarized using median (range), whereas frequency tables were used for categorical variables. For univariate comparison, cross-tabulation, Fisher’s exact test, and Mann–Whitney test were used. All outcomes were measured from the time of AZA administration. Treatment-related mortality (TRM) was defined as death from any cause while in continuous remission of the primary disease.58,59 Cumulative incidences were estimated for relapse and TRM and to accommodate competing risks. Relapse or progression was a competing risk for TRM. The probabilities of OS and EFS were estimated using the Kaplan–Meyer estimator. Log-rank test was used for univariate comparisons of survival curves, while the Gray’s test was conducted to compare cumulative incidences of competing risks endpoints.60,61 Impact of DLI as time-dependent covariate was tested using the Simon–Makuch plot and Mantel–Byar test. Statistical analyses were performed with R 4.0.4 (R Development Core Team, Vienna, Austria) software.
Results
Patients and treatment
We retrospectively analyzed 71 patients (median age, 56 years) diagnosed with AML (n = 52, 73%) and MDS/MPN (n = 19, 27%) who relapsed after HSCT from alternative donors: 29 patients (41%) had received haploidentical grafts and 39 patients (55%) received grafts from MMUD; furthermore, transplantation from single CBU was performed in three patients (4%). The majority of the patients had high-risk and advanced-stage disease at transplantation: DRI was high in 33 patients (46%) and very high in 11 patients (16%); 28 patients (40%) had active disease at transplantation. A myeloablative conditioning regimen was adopted in 37 patients (52%), whereas GvHD prophylaxis mainly relied on ATG-based (40 patients, 56%) and post-transplantation cyclophosphamide (PTCy)-based platforms (24 patients, 34%). Details on patients, disease, and transplantation characteristics are shown in Table S1.
Overall, 31 patients (44%) presented with molecular relapse, whereas 40 patients (56%) had an overt hematologic relapse, including 3 patients with persistence of disease after HSCT (Table 2). The median time from HSCT to relapse (TTR) in the entire cohort was 9 months (range 1–112 months). Among molecular relapse, TTR was 8 months (range 1–55 months). Methods of MRD detection were RT-qPCR in 17 patients (54%), MFC in 3 patients (10%), cytogenetical analysis in 4 patients (13%), and chimerism in unsorted BM mononuclear cells and sorted CD34 + PB cells in 4 (13%) and 3 patients (10%), respectively. Among hematologic relapses, TTR was 10 months (range 1–112 months) and median blast percentage in BM was 13% (range 5–77%). None of them presented with isolated extramedullary relapse; one patient had multiple localizations of leukemia cutis concurrent to relapse in BM. Clinical characteristics of patients at HSCT were well balanced between the types of relapse (Table S2). Compared with MMUD, a greater number of patients diagnosed with AML (p = 0.012) with higher HCT-CI (p = 0.047) and more heavily pre-treated before HSCT (p = 0.0007), and a more common use of BM as stem cell source (p = 0.0002) and PTCy as GvHD prophylaxis (p < 0.0001) were reported among haploidentical transplantation (Table S3).
Clinical and biological characteristics of patients at relapse.

FISH, fluorescent in situ hybridization; GvHD, graft-versus-host disease; HSCT, allogeneic hematopoietic stem cell transplantation; IST, immunosuppressive therapy; MRD, measurable residual disease; PB, peripheral blood; RT-qPCR, real-time quantitative polymerase chain reaction.
Before relapse, 30 patients (42%) were diagnosed with all-grade and 7 patients (10%) with grade III–IV acute GvHD. In the same time-period, 16 patients (23%) had all-grade and 9 patients (13%) had moderate/severe chronic GvHD. At relapse, 27 patients (38%) were still on immunosuppressive therapy (IST): 26 patients successfully discontinued IST during first AZA cycle, while 1 patient presented a reflare of acute GvHD (Table 2).
The median time between relapse and first administration of AZA was 18 days (range 0–73 days). The majority of patients (n = 58, 82%) received AZA 75 mg/m2. Any difference emerged in AZA dosage according to the type of relapse, while more patients after haplo transplantation received 32 mg/m2 schedule than MMUD (n = 8, 28% versus n = 0, respectively; p = 0.0008). Overall, patients received a median of four AZA cycles (range 1–37 cycles), without differences among subgroups (Table 3). However, 39 patients (46%) received DLI in combination with AZA. DLI were given more commonly among MMUD than haplo (n = 24, 61% versus n = 9, 31%, respectively; p = 0.016). Median number of DLI per patient was 2 (range 1–4) and median cumulative amount of CD3 + cells/kg per patient was 2.1 × 106 (range: 0.1–62.5 × 106) (Table 3). Reasons for not giving DLI in 38 patients were PD (n = 17), recent or active GvHD (n = 9), donor unavailability (n = 4), achievement of CR with AZA alone (n = 1), and leukemia relapse with HLA-loss (n = 4).
Characteristics of salvage treatment in overall population and subgroups.

AZA, azacitidine; DLI, donor’s lymphocytes infusions; HSCT, allogeneic hematopoietic stem cell transplantation; MMUD, mismatched unrelated donor.
“p” statistically significant was highlighted in bold.
Response and outcome
Overall, 27 patients (38%) achieved CR and 8 patients (11%) achieved PR, accounting for an ORR of 49%. Higher ORR (n = 20, 65%) and CR (n = 20, 65%) were observed in molecular relapses compared to hematologic relapses (n = 15, 38% and n = 7, 15%, respectively; p = 0.03 and p = 0.0001, respectively). Even considering MRD-negative CR, response rate remained higher in molecular than hematologic relapse (n = 14, 45% versus n = 1, 3%; p < 0.001). Any difference in ORR and CR emerged between the types of donor, although MRD-negative CR was higher in MMUD (n = 10, 26%) compared to haplo (n = 5, 17%; p = 0.004). Median time to CR was 109 days (range 51–300 days), corresponding to four AZA cycles (range 1–8). Median duration of CR was 17 months (range 5–89 months). In addition, 34 patients (48%) had PD (Table 4).
Response to treatment and outcomes in overall population and subgroups.

AZA, azacitidine; CR, complete response; DLI, donor lymphocytes infusions; EFS, event-free survival; MMUD, mismatched unrelated donor; MRD, measurable residual disease; ORR, overall response rate; OS, overall survival; PD, progressive disease; PR, partial response; SD, stable disease; TRM, treatment-related mortality.
“p” statistically significant was highlighted in bold.
After a median follow-up of 11 months (range 1–115 months), median EFS in the entire cohort was 6 months (range 1–90 months) and EFS at 1 year was 26% (CI 95%: 16–36%). Median OS was 7 months (range 1–90 months), with an OS at 1 year of 53% (CI 95%: 40–64%) (Figure 1(a)). Patients with molecular relapse showed higher 1-year EFS (43% versus 13%, p = 0.006) and 1-year OS (79% versus 34%; p < 0.001) than hematologic relapses (Figure 1(b)). No significant difference of survival emerged between haplo and MMUD. At 1-year, cumulative incidence of relapse was 73% (CI 95%: 61–82%), whereas treatment-related mortality (TRM) was 1% (CI 95%: 1–7%) (Table 4).
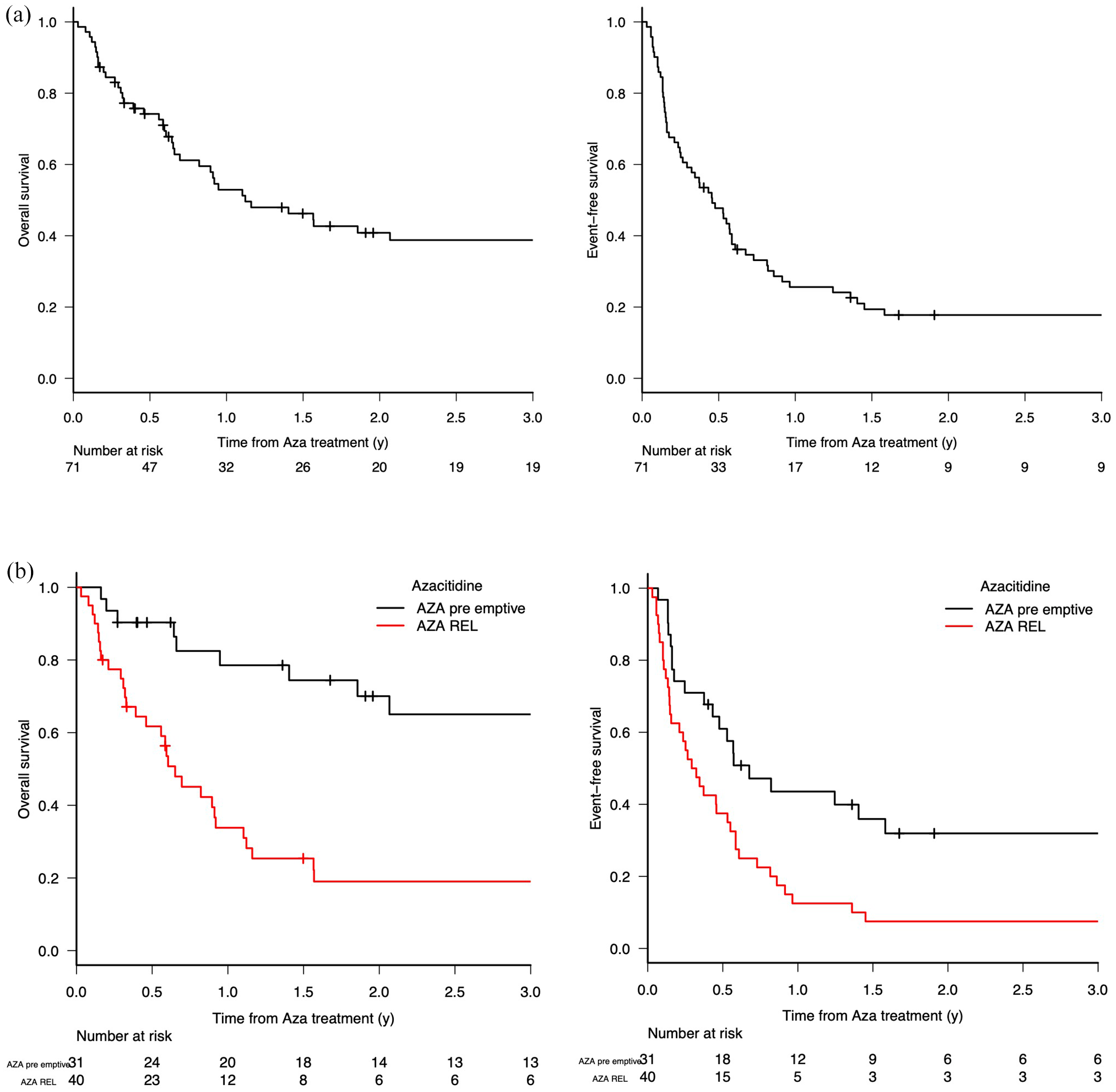
OS and EFS after treatment with AZA ± DLI in the entire cohort and according to the type of relapse.
However, 17 out of 33 patients receiving DLI achieved CR (51%), compared to 10 out of 30 patients receiving AZA single-agent (26%; p = 0.03) (Table S4). To assess the potential benefit of DLI, we plotted Simon–Makuch plots for OS and EFS of patients with or without DLI. Overall, addition of DLI correlated with both longer 1-year EFS (42% versus 17%; Mantel–Byar test, p = 0.004) and 1-year OS (73% versus 31%; Mantel–Byar test, p = 0.002) than AZA single-agent (Figure 2).

Simon–Makuch plots of OS and EFS in patients receiving AZA + DLI compared to AZA.
At data cut-off, 31 patients were alive and 13 patients who achieved CR maintained response without further treatment: 10 patients with molecular and 3 patients with hematologic relapse; 4 patients in haplo and 9 patients in MMUD group. Overall, 34 patients received further treatments at PD, including 11 patients who received a subsequent HSCT. Of those, 3 patients (27%) deceased, whereas 8 patients (67%) are alive and free of disease after a median of 15 months (range 0–100 months). At last follow-up, 40 patients had succumbed from underlying disease (n = 31), infections (n = 4), GvHD (1), second neoplasia (n = 1), and complications of subsequent HSCT (n = 1).
Predictors for response and OS
Univariate analysis identified molecular relapse, BM blasts at relapse < 13% (median at relapse) and the addition of DLI as predictors for CR. The same factors appeared as predictive for both EFS and OS at 1 year. In univariate analysis, time between HSCT and relapse < 6 months also predicted 1-year OS (Table 5).
Univariate analysis of risk factors for response and outcomes.

CR, complete response; DLI, donor lymphocytes infusions; EFS, event-free survival; HSCT, allogeneic hematopoietic stem cell transplantation; MMUD, mismatched unrelated donor; OS, overall survival.
Threshold of 13% was chosen as it represents the median BM blast percentage at morphological relapse.
GvHD and AE
Incidence of all-grade and grade III–IV acute GvHD was 27% (n = 19) and 13% (n = 9), respectively. Acute GvHD occurred after a median of two AZA cycles (range 1–8). Indeed, MMUD suffered more from all-grade acute GvHD (n = 15, 38%) compared to haplo (n = 4, 14%; p = 0.031). However, 10 out of 19 patients developing acute GvHD had received DLI (Table 6). The overall incidence of chronic GvHD was 18% (n = 13), occurring after a median of 3.5 AZA cycles (range 1–8). Eight patients (11%) had moderate/severe chronic GvHD. No significant difference in incidence emerged among subgroups. Therefore, 5 out of 13 patients developing chronic GVHD had received AZA + DLI (Table 6).
Incidence of acute and chronic GvHD in overall population and subgroups.
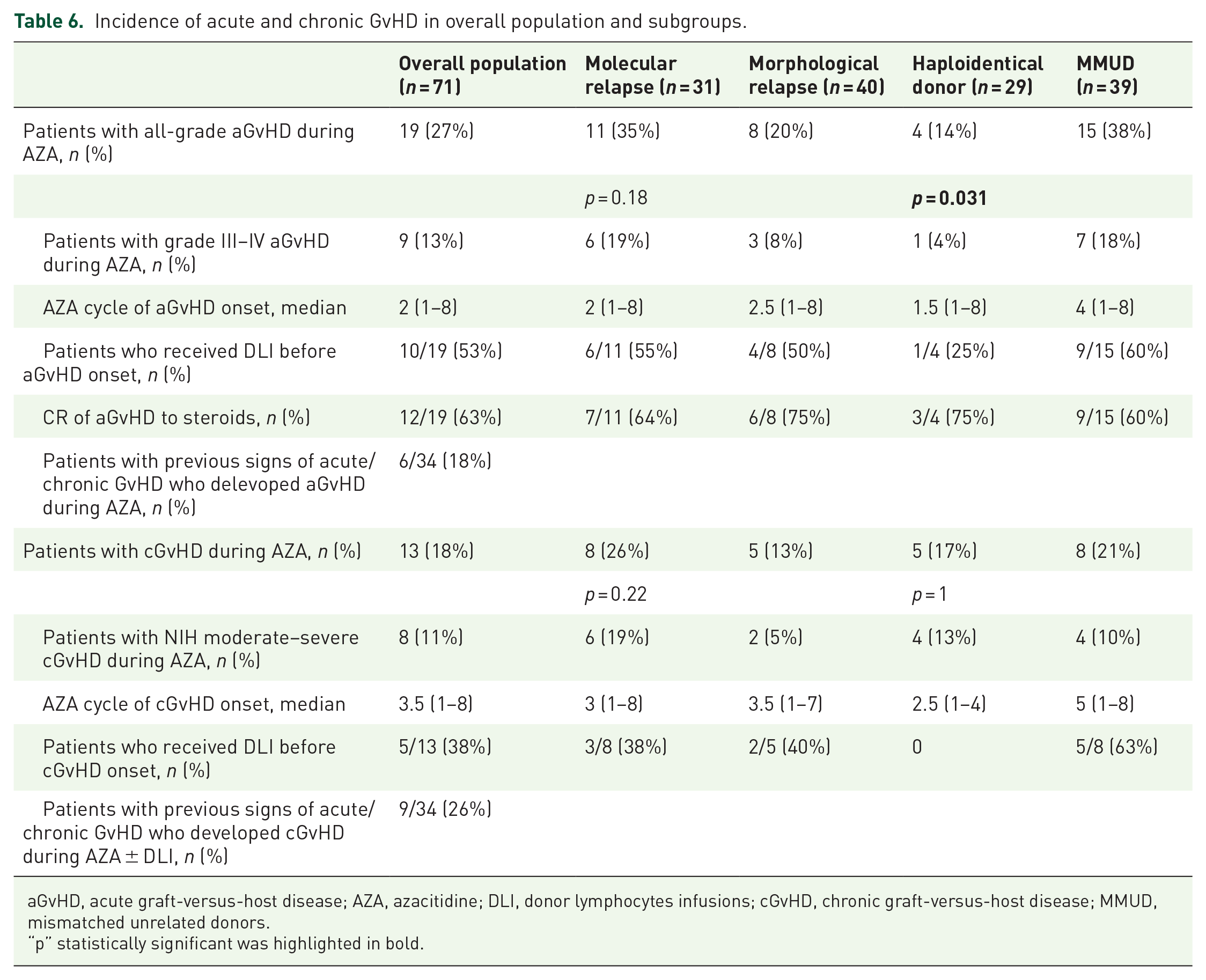
aGvHD, acute graft-versus-host disease; AZA, azacitidine; DLI, donor lymphocytes infusions; cGvHD, chronic graft-versus-host disease; MMUD, mismatched unrelated donors.
“p” statistically significant was highlighted in bold.
Among 41 patients evaluable, most common grade III–IV AE during salvage treatment were hematological: neutropenia (83%), thrombocytopenia (54%), and anemia (42%). Non-hematological grade III–IV AE were mainly infections: febrile neutropenia (32%), pneumonia (10%), invasive fungal infections (6%), and sepsis (2%).
Validation of the AZA prognostic scoring system for relapse after transplantation
In the attempt to stratify patients eligible to AZA-based salvage treatments and to predict response and survival, Rautenberg and colleagues recently developed a new prognostic tool: the AZA Prognostic Scoring System for Relapse after transplantation (APSS-R). 18 In this score, 1 point was assigned for molecular relapse and 2 points for hematologic relapse; for an interval between HSCT and relapse ⩾ 6 months, 0 points were assigned, while 1 point was given for an interval < 6 months. APSS-R clearly stratifies patients into three subgroups (favorable = 1 point, intermediate = 2 points, unfavorable = 3 points), with CR rates of 71%, 39%, and 29%, respectively, and 2-year OS rates of 64%, 38%, and 27%, respectively. 18 When applied to our cohort, we observed CR rates of 76%, 31%, and 13%, whereas OS was 94%, 46%, and 25% at 1-year, respectively. The model confirmed its ability to stratify patients into distinct prognostic groups with significantly different response rates (p = 0.0005) and survival (p < 0.0001) (Table S5) (Figure 3).

OS in the entire cohort according to APSS-R.
Discussion
This study represents, to the best of our knowledge, the first report analyzing in details AZA ± DLI as salvage treatments for AML and MDS/MPN relapsed after HSCT from alternative donors.
When using treatments able to modulate graft alloreactivity, as both AZA and DLI, HSCT from alternative donors represents a particular condition, because of the potentially increased risk of life-threatening GvHD due to donor–recipient HLA disparity. Moreover, HSCT from alternative donors are often performed in advanced-stage disease and burdened by greater toxicities, thus representing a matter of concern for subsequent salvage treatments. Indeed, this is the case of our cohort, characterized by heavily pre-treated patients, high-risk disease, and early recurrence post-HSCT. Nonetheless, administration of AZA 75 mg/m2 proved feasible and tolerance. As expected in the early post-transplantation period, most frequent AE were hematological toxicities and infectious complications, directly related to severe neutropenia induced by treatment. Anyway, TRM remained low.
In our series, we observed an ORR of 49% and CR rate of 38%, EFS at 1- and 2-year of 26% and 18%, respectively, and OS at 1- and 2-year of 53% and 41%, respectively. These data compared favorably with studies on ‘standard’ salvage treatments, reporting CR rate of about 30% and 2-year OS between 10% and 20%.5–7 Our results also resembled those available in literature on post-transplantation AZA ± DLI, characterized by CR rates of 15–67% and a 2-year OS of 12–69% (Table 1).9–31
The burden of leukemia at relapse appears to profoundly influence both response and outcomes. Two retrospective studies found that pre-emptive intervention at MRD reoccurrence leads to higher response and longer survival than treatment at hematologic relapse.18,26 Furthermore, the prospective phase II trial RELAZA-2 reported 53% of CR MRD-negative and a 2-year OS of 62% among patients relapsed post-HSCT, comparably higher than historical controls. 16 In our cohort, univariate analysis identified patients treated at molecular relapse as having significantly higher response rate, EFS, and OS than hematologic relapses. No difference emerged in the number of AZA cycle administered. Pre-emptive treatment with AZA ± DLI led to durable remissions in a considerable proportion of patients, as reflected by the 2-year EFS of 32%. As the duration of CR was particularly long-lasting (median 17 months), even for those patients experiencing PD, pre-emptive therapy might represent a valid intervention, able to delay overt hematologic relapse and to postpone the need for more intensive treatments, allowing recovery from transplant-related toxicities. Therefore, despite prospective, randomized trials are warranted, our results reinforce the value of close post-transplantation MRD monitoring and rapid pre-emptive intervention in case of MRD positivity. On the contrary, AZA ± DLI showed modest efficacy in case of hematologic relapse, probably due to the high proliferative rate of the disease and the insufficient anti-leukemic effect. Nonetheless, trying to identify patients who could benefit from AZA, univariate analysis identified burden of disease in BM as predictive of both response and outcomes. Whereas in the setting of hematologic relapse, IC could still play a role in disease control, in patients with targetable molecular lesions in the combination of either IC or HMA with novel target drugs, such as FLT-3 and IDH1-2 inhibitors, showed promising results.62–67 Moreover, in those patients without targetable mutations, recent results from the combinations of HMA with BCL-2 inhibitor Venetoclax appeared promising.68–70 HMA are also employed as maintenance strategies after HSCT in high-risk patients. Beside the risk of overtreatment, conflicting results emerged from initial studies.32,71,72 Nonetheless, post-HSCT maintenance could still be an option for high-risk patients without disease-specific markers and drug-targetable molecular features. Following encouraging results of oral AZA as maintenance in AML, 73 results are awaited from ongoing trial in the setting of HSCT.74,75
Focusing on type of donor, AZA ± DLI appeared equally effective in both MMUD and haploidentical setting. The lower rate of MRD-negative CR observed among haplo might be related to a selection bias of more aggressive and heavily pre-treated diseases in our cohort. Considering the burden of previous toxicities, haplo also more often received AZA 32 mg/m2.
In previous studies, the most frequently reported predictive factors of response and survival were molecular-only relapse, burden of disease at relapse, and TTR.13,17,18,26 In our cohort, we confirmed these factors, together with the combination of DLI to AZA. Notably, molecular-only relapse emerged as a strong predictor of both response and outcomes in univariate analysis. Many authors tried to develop prognostic scores that are able to identify patients who more capable to benefit from AZA ± DLI. A first attempt was made by Craddock et al. with the ‘AZA Relapse Prognostic Score’ (ARPS), considering burden of disease in BM and TTR. 13 Despite its validity, the ARPS was tested only in patients with hematologic relapse. This appears as a possible limit, considering both increasing evidence and real-life practice favoring MRD-driven pre-emptive interventions. Recently, Rautenberg et al. proposed a novel scoring system, the APSS-R, developed from a single-center retrospective analysis and based on type of relapse and TTR. 18 When applied to our cohort, the APSS-R was able to clearly stratify patients even in the setting of alternative donors. Therefore, APSS-R might become a useful tool to predict outcomes in all patients receiving AZA post-transplantation.
The effective role of DLI is still a matter of debate. As DLI appeared necessary in consolidating responses to IC in post-transplantation relapses,5,6,8 their contribution when given together with AZA is less clear. A large retrospective study by Schroeder et al. initially reported on a possible benefit. 26 Conversely, Craddock et al. 13 found no impact of DLI both on response and survival. Notably, this study included only hematologic relapses and the majority of patients received DLI in the absence of a clinical response. A prospective study on pre-emptive AZA without DLI also showed consistent but not durable responses. 23 Recently, Rautenberg et al. 18 reported higher response rates and significant survival advantage in patients receiving DLI for both molecular and hematologic relapses. In our experience, we confirmed that the addition of DLI to AZA significantly improved response rates and correlated with longer EFS and OS compared to AZA single-agent.
In our population, the incidence of both acute and chronic GvHD before relapse was consistent with historical data on alternative donors.50,76–78 Despite HLA mismatches, during and shortly after treatment with AZA ± DLI, we observed an incidence of all-grade acute and chronic GvHD consistent with previous studies (Table 1).9,10–26 Besides the limit of small numbers, a previous diagnosis of GvHD and administration of DLI did not impact on the incidence of GvHD during salvage treatment. The incidence of GvHD in our study compared favorably also with that reported by haploidentical DLI.79–81 Indeed, the different incidence of acute GvHD between the types of donors appeared to mainly rely on the relatively low incidence observed among haplo. Possible explanations could be a greater use of BM as HSC source and PTCy as GvHD prophylaxis in haplo. Notably, sirolimus was also adopted in combination with PTCy in many haploidentical HSCTs in our cohort, a platform of GvHD prophylaxis reported to favor the expansion of regulatory T cells.82,83
Limitations of this study include retrospective non-randomized nature, limited numbers only allowing univariate analysis, the possibly biased-selected population and heterogeneity of treatments. Multicentricity might limit the single-center effect in the management of patients.
Conclusion
AZA either single-agent or in combination with DLI proved feasible and effective in treating patients with AML and MDS/MPN relapsing after HSCT from alternative donors. The treatment was well tolerated, with an acceptable burden of toxicities and GvHD. In case of overt hematologic relapses, the salvage treatment with AZA ± DLI showed a modest efficacy. In this setting, combinational strategies of either IC or HMA with novel target drugs and Venetoclax might play a role. Conversely, AZA fared better in the setting of MRD. Pre-emptive treatment of molecular relapse granted higher response rate and longer outcomes, leading to durable remissions in a considerable proportion of patients. Even for those patients finally experiencing PD, pre-emptive therapy might represent a valid intervention, able to delay overt hematologic relapse, and to postpone the need for more intensive treatments. Our results reinforce the need of close post-transplantation MRD monitoring and the value of early pre-emptive interventions. When applied to our cohort, APSS-R clearly stratified patients in distinct prognostic subgroups, thus appearing as a useful tool to predict outcomes even for alternative donors. Finally, we confirmed the benefits of DLI in combination with AZA, as their role appeared essential in obtaining better responses and ensuring longer survival.
Supplemental Material
sj-docx-1-tah-10.1177_20406207221090882 – Supplemental material for Azacitidine and donor lymphocytes infusions in acute myeloid leukemia and myelodysplastic syndrome relapsed after allogeneic hematopoietic stem cell transplantation from alternative donors
Supplemental material, sj-docx-1-tah-10.1177_20406207221090882 for Azacitidine and donor lymphocytes infusions in acute myeloid leukemia and myelodysplastic syndrome relapsed after allogeneic hematopoietic stem cell transplantation from alternative donors by Carmine Liberatore, Maria Teresa Lupo Stanghellini, Francesca Lorentino, Luca Vago, Matteo Giovanni Carrabba, Raffaella Greco, Sarah Marktel, Andrea Assanelli, Francesca Farina, Consuelo Corti, Massimo Bernardi, Jacopo Peccatori, Katja Sockel, Jan Moritz Middeke, Johannes Schetelig, Anika Bergmann, Christina Rautenberg, Fabio Ciceri, Martin Bornhäuser, Thomas Schroeder and Friedrich Stölzel in Therapeutic Advances in Hematology
Footnotes
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.F. received honoraria from Jazz Pharmaceuticals, served on advisory boards for Medac GmbH and Novartis. B.M. received honoraria from Celgene/BMS, Alexion, Novartis, MSD; travel grants from Celgene/MSD; served on advisory boards for BMS and Jazz Pharmaceuticals. C.M.G. declared consultancy for Janssen, Novartis, and Abbvie. S.T. declared research funding and consultancy for Celgene/BMS. R.C. received travel grants from Jazz Pharmaceuticals and Celgene/BMS; lecturing from Abbvie, Celgene/BMS, and Jazz Pharmaceuticals. MTLS has received travel grants from Neovii Biotech; honoraria from Incyte; served on advisory boards for Novartis and Mallinckrodt Pharmaceuticals. L.C., L.F., V.L., G.R., M.S., A.A., F.F., C.C., B.M., P.J., S.K., M.J.M., S.J., B.A., and C.F. declare no competing financial interests.
Ethics approval,consent to participate
Six patients in Duesseldorf cohort were treated within the prospective phase II trial (NCT00795548). Data have been reported previously 24 but were updated for this analysis. All patients gave informed consent for treatment with AZA ± DLI. Patients were treated according to current institutional programs on written informed consent for transplantation procedures, biological sampling, and use of medical records for research (Ethical approvals: ALMON study approved by San Raffaele Institutional Ethical Committee on date 19/10/2007; Düsseldorf ethic Approval No. 4138/5309; TU Dresden Ethical Approval No. EK132042018). Patients’ date was de-identified and anonymized.
Availability of data and materials
All data produced in the present study are available upon reasonable request to the authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.