
Abstract
Background:
Our aim was to identify health-related quality-of-life (HRQoL) issues and symptoms in patients with haematological malignancies (HMs) and develop a conceptual framework to reflect the inter-relation between them.
Methods:
A total of 129 patients with HMs were interviewed in a UK multicentre qualitative study. All interviews were audio recorded, transcribed and analysed using NVivo-11.
Results:
Overall, 34 issues were reported by patients and were grouped into two parts: quality of life (QoL) and symptoms. The most prevalent HRQoL issues were: eating and drinking habits; social life; physical activity; sleep; and psychological well-being. Furthermore, most prevalent disease-related symptoms were: tiredness; feeling unwell; breathlessness; lack of energy; and back pain. The most prevalent treatment side effects were: tiredness; feeling sick; disturbance in sense of taste; and breathlessness.
Conclusions:
Both HMs and their treatments have a significant impact on patients’ HRQoL, in particular on issues such as job-role change, body image and impact on finances.
Introduction
Haematological malignancies (HMs) include neoplasms of myeloid and lymphoid cell lines 1 with an expected UK incident rate of 38,740 per annum. 2 The non-Hodgkin’s lymphomas are the most prevalent HMs in the UK, followed by leukaemias and other lymphomas. 3 The World Health Organization (WHO) defines the primary objectives of cancer diagnosis and treatment as cure, prolongation of life and improvement of the quality of life (QoL). 4 The maintenance of patients’ well-being is a fundamental goal of medical practice. Although treatments have the potential to cure or prolong life in some patients, the evidence suggests that health-related QoL (HRQoL) of patients with HM is significantly affected by the disease and its treatments.5–11 Until recently, it was assumed that measurement of an individual patient’s QoL as an endpoint was specific to clinical-trial scenarios evaluating efficacy of a single treatment. However, it is reported that the QoL information used during outpatient consultation may influence treatment decision making and result in changes in the current interventions or initiation of new ones. Thus, the assessment of QoL in routine clinical practice in patients with HMs is greatly needed and there is much demand from haematologists. This, alongside clinical care, could monitor response to treatment, focus on goals of care, identify unmet patients’ needs and facilitate patient–physician communication.12–14
Planning provision of patient care requires incorporating patients’ views and lived experience of disease and treatment. Given the rapid uptake and success of several treatments, HM is being transformed from a disease that one died from to a disease that one lives with. Hence, experiential patient evidence is a cornerstone of patient-centred care. Issues related to burden of the disease and treatment, information about the disease and the treatment, support factors, body image, insecurity, financial and insurance-related issues are generally overlooked, 15 thus it is essential to further explore and identify the importance of these issues from HM patients’ perspectives.
Some recent systematic literature reviews highlighted how HM negatively affects patients’ overall HRQoL and reported psychological, social, professional, financial, sexual, cognitive and physical well-being as significant areas of such impact.15,16 Furthermore, the authors emphasised the importance of assessing HRQoL in the early course of care in order to adopt interventions which could improve physical and mental functioning. 16 Another systematic review conducted describes how the burden of disease increases with the ageing population.17,18
A recent systematic literature review was published in 2019 with an aim to identify HRQoL issues important to patients with HMs, and the HRQoL instruments used both in routine clinical practice, as well as in clinical research. 15 The review unfolds the evidence gap in the qualitative literature as well as the gap in the conceptual coverage among the identified instruments currently used in haematology. Among the 24 identified qualitative studies reviewed, only 3 reported sampling to redundancy (saturation), which is an important sampling criterion for qualitative studies. Moreover, the review reflected that current instruments do not cover important issues such as worrying/uncertainty about future, eating and drinking habits, being a burden to others, being judged by other people, travelling, going on holidays, difficulty with leaving the house, appearance/body image and sleeping patterns. 15 This highlights the need for conducting a well-structured qualitative study using sampling-to-redundancy methodology to better understand the lived experience with different HMs from a patient’s perspective. The aims of the study were: (a) to explore the impact of a wide range of HMs and their treatment on patients’ HRQoL and symptoms, from their own perspective; and (b) to develop a conceptual framework based on the identified HRQoL issues and ‘signs and symptoms’.
Methods
Patient recruitment
The inclusion criteria were: ability to give informed written consent; being diagnosed with HM as per the most recent WHO classification; 19 any state of the disease (stable, progressing or remission); any stage of the treatment (due to start the treatment, on treatment or finished treatment); and ability to read and write in English. A purposive sampling was chosen, including various types of HM, different states of the disease and treatment and geographical location, as such that the sample would be representative of the target population. Patients from 10 different HMs were recruited into the study including: acute myeloid leukaemia (AML), acute lymphoid leukaemia (ALL), chronic myeloid leukaemia (CML), chronic lymphoid leukaemia (CLL), multiple myeloma (MM), myelodysplastic syndromes (MDS), myeloproliferative neoplasm (MPN), Hodgkin lymphoma (HL), indolent non-Hodgkin lymphoma (INHL) and aggressive non-Hodgkin lymphoma (ANHL). Non-Hodgkin lymphoma (NHL) patients were categorised as indolent or aggressive based on rate of progression and irrespective of cell type (B/T cell). For example, diffuse large B-cell lymphoma and lymphoblastic lymphoma were grouped into ANHL, and follicular lymphoma and adult T-cell lymphoma were grouped into INHL. The MPN category included myelofibrosis, essential thrombocythemia and polycythemia vera. The principal investigator from each participating centre or respective clinical nurses confirmed the type of diagnosis as listed above and categorised the patients as progressing, in remission or stable.
The stable, progressing, remission state of the disease was completely based on disease progression irrespective of whether a patient was on treatment. Therefore, patients could be on a treatment, awaiting treatment or off treatment. The primary focus was to be inclusive and the views of all types of patients to be considered and to understand the impact of the disease without limiting it to a particular stage or status of the treatment. Each study participant was assigned a unique identification number to allow collection of anonymised sociodemographic characteristics.
Patient research partner
A patient research partner (RE) diagnosed with CLL, was closely involved throughout the study as a member of the research team and carried out patient interviews. He will be referred to as ‘patient research partner’ throughout the paper.
Patient interview guide
A draft version of the ‘patient interview guide’ was prepared following discussion with the ‘patient research partner’ and was finalised after pilot testing with five patients (Table 1). Both interviewers had undergone qualitative interview research training at the University of Hertfordshire for carrying out patient interviews.
Suppinfo: patient interview guide.

QoL, quality of life.
Procedures
This study employed face-to-face interviews with open-ended questions related to HRQoL and symptoms. Patients with different types of HM were interviewed from six secondary care hospitals in England and Wales, United Kingdom, from both inpatient and outpatient settings. Interviews were audio recorded and transcribed verbatim. Of all the transcriptions, 10% were randomly selected and validated by an independent interviewer (i.e. patient research partner) who was not involved in the transcription. This was done to confirm that all the transcripts fully reflected what had been reported by the patients. All the patients were encouraged to be honest, open and as detailed as possible. As there is no set sample size for such research, the criteria used in this study was ‘sampling to redundancy’ that is, interviewing people until a saturation point is reached and no new theme or sub-theme emerges. 20 Since patients with 10 different HMs were recruited into the study, it was deemed prudent to aim for establishing saturation for each of the 10 HMs.
Data processing and analysis
The content analysis of all the transcribed interviews was performed using the NVivo 11 qualitative analysis software. 21 The conventional content analysis approach was used to allow different HRQoL categories and the names of the categories to flow from the data rather than using any preconceived categories.22,23 The initial coded segments were clustered into categories that led to theme development following Saldana’s codes to theory model. 24 The coding was carried out by PG and RE separately and was discussed to reach consensus. Any unresolved discrepancies were then further discussed with the third reviewer, the adjudicator (SS), to reach a decision. Furthermore, the final list of coded themes and sub-themes was then discussed among a panel of experts involving two haematologists, three patient-reported outcome measure (PROM) experts, a patient-advocacy group representative and a patient with HM. The relationship between the themes and sub-themes was based on the concurrence, antecedents or consequences that helped develop the conceptual model. 25
Analysis of the transcriptions commenced after the first five interviews and was consistent with a constant comparison technique where new data was examined in the light of emerging themes. This technique helped to insure the ‘fit’ between the data and developing themes and added credibility to the findings. The coding followed the cross-analysis to identify issues and symptoms specific to disease type, disease state, age and sex.
Although, technically, the terms ‘signs’ and ‘symptoms’ are different, but the patients used them interchangeably. Therefore, all the findings were classified into two categories: HRQoL issues; and signs and symptoms. The classification of the themes and sub-themes into two categories was based on the underlying cause from the patients’ perspective. For example, if a patient reported difficulty moving around in the house due to tiredness, then tiredness, which is the proximal impact of the disease or the treatment, was classified into the ‘sign and symptom’ category, whereas the distal impact of tiredness, that is, difficulty moving around in the house, was categorised into HRQoL issues.
Results
Socio-demographics characteristics of the study participants
A total of 129 patients (male = 76–58.9%; mean age = 61.12 years; median age = 65 years; age range = 18–88 years) with median time since diagnosis of 2 years (range = 19 days to 23 years) were recruited into the study (Table 2). There was a difference in median age between different HMs, as expected; MM, CLL, MDS and MPN were diagnosed mostly in older patients, whereas HL and CML were diagnosed in a younger patient population. In addition, AML, CLL, CML and ALL were more prevalent in males compared with females. A total of 50 (38.6%) patients had other comorbidities [the most prevalent were arthritis (7), asthma (4), hypertension (6), diabetes (4)], of whom 5 had other types of cancers [prostate cancer (3), lung cancer (1), skin cancer (1)]. The median duration of the interviews was 26 min (range = 11–54 min).
Socio-demographic characteristics of the study participants (n = 129).

ALL, acute lymphoblastic leukaemia, AML, acute myeloid leukaemia ANHL, aggressive non-Hodgkin lymphoma; CLL, chronic lymphoid leukaemia; CML, chronic lymphoid leukaemia; HL, Hodgkin lymphoma; INHL, indolent non-Hodgkin lymphoma; MDS, myelodysplastic syndromes; MM, multiple myeloma; MPN, myeloproliferative neoplasm; SD, standard deviation.
Saturation point
After every five interviews, transcriptions were analysed to check for saturation point. The new themes and sub-themes were emerging until the 120th patient was recruited into the study. To confirm the saturation, we continued interviewing seven patients from the same hospital sites, followed by two new patients from a different geographical location, separated by a period of 2 months. The additional nine interviews did not generate any new theme(s) for any of the 10 HMs and therefore saturation was confirmed.
Health-related quality-of-life themes generated by patients with HM
Following the content analysis of all transcribed interviews, the issues were coded into themes and sub-themes. This resulted in a list of overall 34 categories of issues identified to be important from the patients’ perspective. After reaching consensus among the panel, these issues were then grouped under two parts: HRQoL issues (impact); and symptoms (Table 3).
Health-related quality-of-life themes and symptoms reported by patients with haematological malignancies.

A sample of the 34 categories of issues identified will be described fully here in two parts: part I, QoL issues; and part II, symptoms. A more detailed version of the manuscript will be available from the authors on request.
Part I: quality-of-life issues
Eating and drinking habits
Concerns related to eating and drinking habits were raised by 117 patients of whom 30% were in the age group of 65–75 years and 45% between age group 35–65 and were more prevalent in males (61%). Forty-two (36%) of these patients were in the early course of their disease (less than a year). A total of 58 patients changed their eating and drinking habits after being diagnosed or as a result of treatment [Table 4: 1(a, b)] and 48 patients reported a decrease in their appetite during or after treatment [Table 4: 1(c)]. Conversely, 13 patients reported an increase in appetite, which was mainly associated with steroids prescribed during treatment [Table 4: 1(d)], 29 patients reported they had stopped drinking alcohol since their diagnosis and 28 reported reduced alcohol intake, whereas 2 patients reported an increase in alcohol consumption as a reaction to their diagnosis [Table 4: 1(e)].
Patient quotes.

ALL, acute lymphoid leukaemia; AML, acute myeloid leukaemia; CLL, chronic lymphoid leukaemia; CML, chronic myeloid leukaemia; FL, follicular lymphoma; INHL, indolent non-Hodgkin lymphoma; MDS, myelodysplastic syndrome; MM, multiple myeloma; MPN, myeloproliferative neoplasm; NHL, non-Hodgkin lymphoma.
Social life and participatory function
A total of 86 patients (66%) with different HMs reported issues relating to their social life and participatory functions. Twenty-eight (32.6%) of these patients were diagnosed less than a year ago and 35 (40.7%) were still in the ‘active’ disease state. Only 20% of the patients diagnosed 5 years ago reported impact on social life and participatory function. Most of the patients were known to have a clinically exploitable immune system because of the disease and treatments and 21 patients were housebound due to severe neutropenia. The patients discussed difficulty with being isolated and they could not go out in ‘crowds’ because they were susceptible to infections [Table 4: 2(a)]. For other patients, the issue was mainly a physical inability, as they did not have enough strength to move [Table 4: 2(b)]. Further concerns were related to ‘eating or drinking out’; for many patients, their social life involved going to the restaurants for meals or going to the pub [Table 4: 2(c)].
Physical well-being and independence
A total of 70 patients (54%) reported limitations in physical activity. This was experienced in the early course of the disease and was raised by 38 (54.3%) patients who were retired, with the highest being among the 65–75 years’ age group. Tiredness, lack of energy and low muscular strength were the main reasons for limited physical activities [Table 4: 3(a)]. Eight patients were having difficulty in going up or down the stairs and five patients reported difficulty in walking up or down the hill. Immobility made them dependent on their caregiver for even basic daily activities [Table 4: 3(b, c)].
Psychological well-being and attitude towards treatment
Maintaining a sense of psychological well-being and being positive towards life is very difficult for HM patients. Sixty-four (50%) patients reported concerns relating to their psychological well-being. The patients expressed how traumatic and emotional their diagnosis has been. Fourteen patients expressed disappointment and frustration about the diagnosis and the treatment. One patient expressed suicidal thoughts because of the condition [Table 4: 4(a)]. Forty-three (33%) patients mentioned that they were distressed during and after the treatment. Similarly, 27 (21%) discussed their worries about treatment, their families and about their physical appearance.
When asked about any concerns, 27 patients expressed their worries. Most of these patients were worried about their future health, work, studies, family and finances. Three patients expressed uncertainty about the future being really disappointing. Seven patients who were in remission mentioned that they were always thinking and worried about relapse.
Daily activities/chores and home management
A total of 62 patients (48%) experienced negative impacts on their daily activities, 25 (40.3%) of whom were diagnosed less than a year ago. Seventeen patients (13%) mentioned that they had stopped or did less cooking because of lack of energy and tiredness. Fifteen patients (12%) were not able to do any work, 13 of whom were still on treatment at the time of the interview [Table 4: 5(a)]. Furthermore, 4 patients reported difficulty in taking a shower and 3 had problems with dressing up [Table 4: 5(b)]. Nine patients discussed the difficulty in going for their regular shopping [Table 4: 5(c)].
Sexual life
Sexual feelings and attitude may change for a person at different points in life; in particular, for those with a chronic life-threatening disease. To this end, 55 patients (43%) reported concerns regarding their sexual life. Male patients (69%) were affected more than females (30.9%). A total of 14 (26%) of these were diagnosed 2–4 years ago and 22 (40%) were on remission. Most of their concerns were particularly during the early course of their disease and treatment [Table 4: 6(a)]. The main reasons for impaired sexual life were tiredness, lack of energy, lack of confidence, skin bruises, scars, disappointment and frustration because of the disease and treatment. Seven patients expressed concerns about their body image.
Work life, study and the ability to manage finances
Fatigue had significant effect on workers, affecting their physical functioning/work performance and ability to concentrate. A total of 55 patients (42%) reported a negative impact on their work life, of whom 10 had to take early retirement. In addition, three patients had given up their jobs, two were dismissed and three made redundant. Seven patients experienced a change in their job-role function, as they could not cope with the demands of their previous role or because their job was given to someone else [Table 4: 7(a)]. Three patients had to close their business, as they were spending most of their time in the hospital or recovering in bed at home [Table 4: 7(b)]. The main reasons for the impact on work life as reported by the patients were tiredness, amount of time spent in hospital for diagnostic procedure and treatments, and inability to concentrate. Two students could not continue their studies and had to take a break because of the treatment.
A total of 36 patients reported difficulty in managing their finances, of whom 31% were in the 25–45 age group and, interestingly, 42% in remission [Table 4: 7(c–e)]. Furthermore, there was also no or limited support for the self-employed who were greatly affected financially, as they did not have any employer providing paid sick leave.
Part II: disease-related symptoms and treatment side effects
When asked what kind of symptoms they experienced at the time of diagnosis, before they started treatment, 102 different symptoms were reported (Table 5). With respect to disease-specific symptoms: 15 patients, all with lymphoma, reported ‘night sweats’; 18 patients experienced ‘back pain’, of whom those with MM were affected the most; 21 patients suffered from ‘lack of energy’, of whom the AML patients were affected the most (5); 16 reported ‘weight loss’ with the highest in CML patients (4); 7 patients experienced ‘bone ache’ of whom the MM patients (5) were highly affected; and 9 were affected by ‘lump on the neck’, with the highest among those with HL (5). In contrast, 13 patients reported ‘no symptoms’, out of which 4 (30.8%) were CLL, 3 (23.1%) CML and 3 (23.1%) MPN patients. Eight (88.9%) of nine cases of ‘chest pain’ were reported by males.
Disease-related symptoms and treatment side effects reported by patients with haematological malignancies.
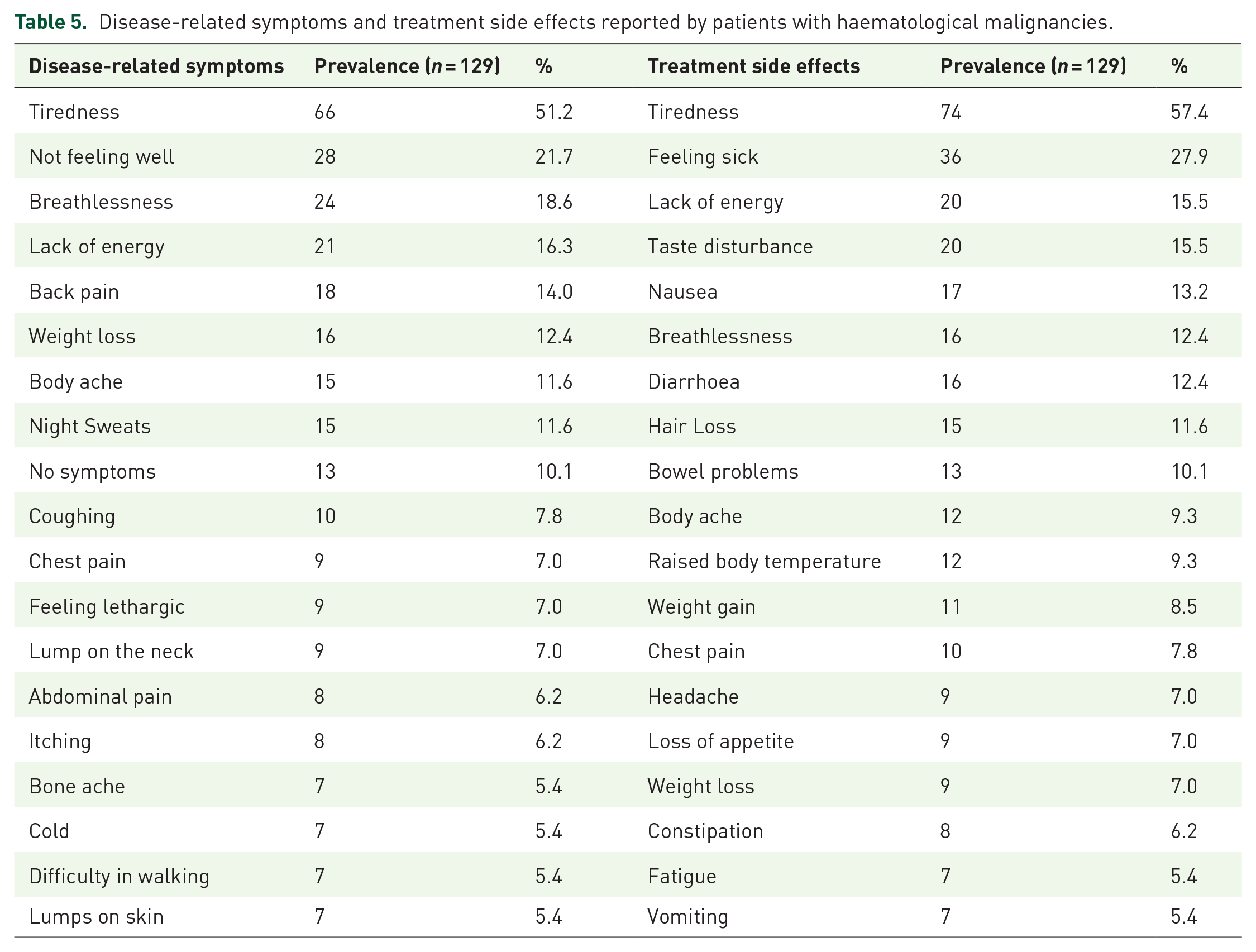
A total of 121 side effects were reported when patients were asked if they had experienced any side effects with their treatment (Table 5). Breathlessness was observed the highest in the CML patients (4 of 16), and 5 of the 16 cases were among the 65–75 age group. Four of the eight reported constipation cases were patients with ANHL. Hair loss was highly reported by the ANHL patients (7 of 15 cases). Male patients were highly affected by body ache (10 of 12), diarrhoea (11 of 16), headache (8 of 9) and nausea (10 of 16).
Conceptual model
A revised conceptual model, which superseded the initial hypothesised conceptual model, was developed to help to understand the relationship between the themes and how they have been classified in this research (Figure 1). The model shows relevant concepts, organised by type, with the proximal impact (i.e. areas directly impacted by the disease or the treatment) on the left and the distal impact (i.e. indirect and long-term effect of the disease and the treatment) on the right. All the signs and symptoms reported by more than five patients and the impact of the diagnostic and treatment procedures were found to be more proximal. Further, impact on social limitation and physiological well-being was found to be a more distal impact of the disease.

Conceptual model for impact on HRQoL for patients with HMs.
Discussion
The primary purpose of this research was to better understand the experiences of adult patients living with haematological malignancy. This study goes beyond the general qualitative research methodology by recruiting 129 patients using purposive sampling techniques to reach saturation point for each of the 10 HMs in order to improve their generalisability across individual HMs. The HRQoL issues and signs and symptoms reported in the other studies are among those identified through this qualitative research.5–11,15 However, this study goes beyond the common themes reported by previous qualitative research and has identified HRQoL issues such as ‘eating and drinking, sleep, delayed diagnosis, duration of treatment, medication management, blood transfusions’, and sign and symptoms such as ‘lumps, abdominal pain, itching, taste disturbance, and loss of appetite’ which were reported by HM patients in this study with high prevalence and significantly affecting patients’ lives. Furthermore, this study has also identified that only 10% of patients did not experience any symptoms at all prior to their diagnosis or remission. The comprehensive qualitative analysis including identification of the proximal and distal determinants impacting HRQoL carried out in this study clearly reflect the intricate picture of the patients’ lives and all the areas that are greatly affected by the disease and its treatments.
The key symptoms, as well as treatment side effects, reported by all the patients, were tiredness and fatigue, which support the findings of previous studies.26,27 In addition, this study has identified that patients with HM suffer from a great deal of anxiety and depression5,28 and has clarified the main reasons behind this emotional behaviour; that is, the unmet need of these patients with respect to psychological support. Interestingly, not a single patient mentioned that he/she was offered any psychosocial screening and/or rehabilitation. Further, we also found a communication gap between the patients, consultants and hospital staff which created a delay in diagnosis/treatment which, in turn, prevented them being able to express their feelings. Moreover, the waiting time for the appointments, blood test or scan results contributed to anxiety and impaired psychological well-being. Diagnostic procedures, such as bone marrow test and biopsy, and treatment procedures, like blood transfusion, were identified as the main burden of disease.
The findings clearly indicate how the disease and side effects of treatments affect relationships. Many patients during the interviews expressed that they were not comfortable talking about issues related to their personal and sexual life to the consultant and/or other hospital staff. The impaired psychological and physical well-being and duration of treatments were the main reasons for the negative impact on work life, which have also been reported in previous studies.29,30
Conclusion
The evidence generated by this study clearly suggests that HRQoL of patients with HM is significantly affected by the disease and its treatments and the relationship between the different HRQoL issues is more complex than it appears.
The conceptual framework developed may help the clinicians and clinical practice staff to successfully implement the knowledge translation interventions in their practice. Such a framework can assist uptaking the evidence on patients’ HRQoL, identify its proximal and distal impact and discuss with the patients a tailored intervention on an individual basis. This framework would also act as a bridge between research and practice.
Study limitations
Although some of our findings support previously published studies, it should be noted that the study is qualitative in nature and not a hypothesis-testing one. Thus, it did not lend itself to statistical analysis. The heterogeneity in the sample might be considered as another limitation of the study, but the saturation point for both ‘HRQoL issues’ and ‘signs and symptoms’ across different HMs was achieved and is consistent with the research question. However, no such study has been performed previously and therefore, it is unique in the sense of involving patients with all kinds of HMs. Furthermore, the study recruited patients from secondary care hospitals in the UK and therefore has a form of geographical limitation and may not be representative of the HM population outside the UK.
Clinical implications
There are no clinical implications of this study.
Footnotes
Acknowledgements
The authors would like to thank the input of all the study participants and participating centres for their support throughout the study.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Consent for publication
All the authors gave their consent for publication of the manuscript.
Ethics approval and consent to participate
Multicentre ethics approval was obtained from the NRES South West Bristol, UK (ref 14/SW/0033) followed by individual research-and-development approvals from all the participating centres. Signed informed consent was obtained from all study participants.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
The author(s) disclose receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the European Haematology Association Scientific Working Group ‘Quality of life and symptoms’ through unrestricted grants from Novartis, Bristol Myers Squib and Sanofi.