
Abstract
Autologous stem-cell transplantation (ASCT) remains an integral part of treatment for previously untreated, and may have value in the treatment of relapsed patients with, multiple myeloma (MM). The addition of novel agents like immunomodulators and proteasome inhibitors as induction therapy before and as consolidation/maintenance therapy after ASCT has led to an improvement in complete response (CR) rates, progression-free survival (PFS) and overall survival (OS). With advances in supportive care, older patients and patients with renal insufficiency are now able to safely undergo the procedure. The data concerning the timing of ASCT (early in the disease course or at first relapse), single versus tandem (double) ASCT and the role and duration of consolidation and maintenance therapy post ASCT remain conflicting. This review aims to discuss the evolution of stem-cell transplant over the past 3 decades and its current role in the context of newer, safer and more effective therapeutic agents.
Introduction
Multiple myeloma (MM) is the second most common hematological malignancy accounting for nearly 10% of all hematological malignant disorders and 0.9% of all cancer deaths every year.1,2 Until the mid 90s, a combination of corticosteroids and melphalan was the standard treatment for patients with MM which gave a median survival of 3 years or less. 3 However, the introduction of autologous stem-cell transplant (ASCT) in combination with high-dose chemotherapy (HDCT) improved the median survival to 7 years.4,5 With the emergence of safer and more effective novel therapies like immunomodulatory drugs (IMiDs) including thalidomide, lenalidomide and proteasome inhibitors (PIs) including bortezomib, the outcomes have vastly improved. 6 More recently, pomalidomide, carfilzomib, ixazomib, daratumumab and elotuzumab have been approved for treatment of MM. 7 The availability of these safer and more effective agents has raised doubts about using ASCT as first-line therapy, especially because both chemotherapy and ASCT only prolong progression-free survival (PFS) and overall survival (OS), and do not produce a cure. Though allogeneic transplant offers a potential for cure, it is at a cost of increased treatment-related morbidity and mortality.
In this review, we aim to discuss the evolution of stem-cell treatment for the management of MM, including its role as part of initial therapy, in relapsed and refractory patients, associated complications, pros and cons of early versus delayed ASCT as well as single versus tandem ASCT.
Conventional chemotherapy versus stem-cell transplant
ASCT has been the mainstay of therapy in young (<65 years) transplant-eligible patients with MM. The trials comparing chemotherapy alone with ASCT have conflicting results. The impact of ASCT on complete response (CR) rates as well as on PFS and OS as compared with chemotherapy according to various studies are shown in Table 1.
Conventional chemotherapy versus ASCT.
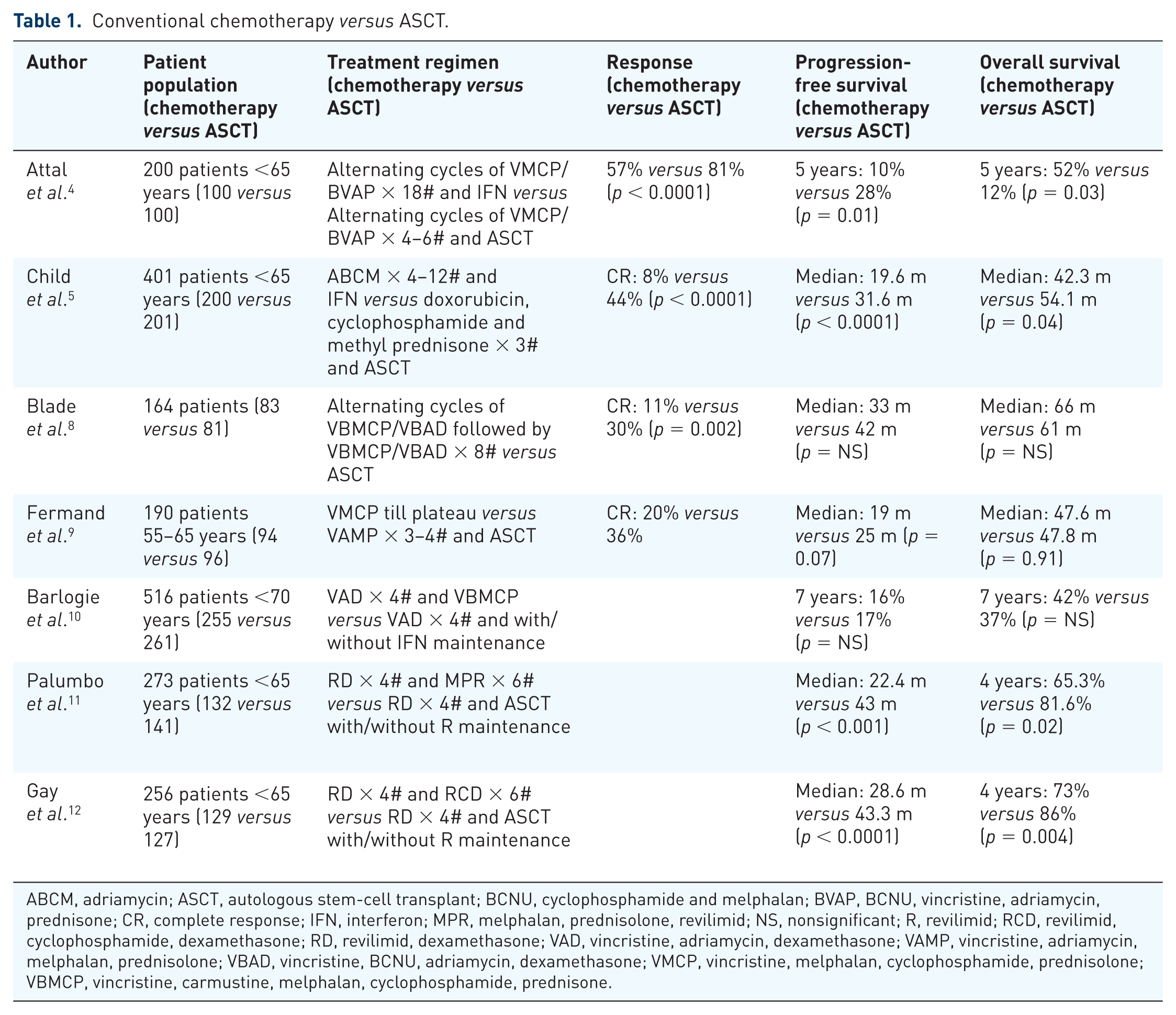
ABCM, adriamycin; ASCT, autologous stem-cell transplant; BCNU, cyclophosphamide and melphalan; BVAP, BCNU, vincristine, adriamycin, prednisone; CR, complete response; IFN, interferon; MPR, melphalan, prednisolone, revilimid; NS, nonsignificant; R, revilimid; RCD, revilimid, cyclophosphamide, dexamethasone; RD, revilimid, dexamethasone; VAD, vincristine, adriamycin, dexamethasone; VAMP, vincristine, adriamycin, melphalan, prednisolone; VBAD, vincristine, BCNU, adriamycin, dexamethasone; VMCP, vincristine, melphalan, cyclophosphamide, prednisolone; VBMCP, vincristine, carmustine, melphalan, cyclophosphamide, prednisone.
A meta-analysis comprising 2411 patients indicated that the combined hazard of progression was 0.75 [95% confidence interval (CI) 0.59–0.96] and death was 0.92 (95% CI 0.74–1.13) with upfront ASCT as compared with standard-dose chemotherapy. However, most of the studies included in the meta-analysis were conducted using older lesser effective chemotherapeutic regimens. Also, the impact of ASCT at relapse may have led to similar OS among those who received chemotherapy. 13 As novel therapies can produce CR rates comparable with ASCT, a question arose: whether the use of these newer agents, alone or in combination, will delay or eliminate the need for ASCT. Palumbo and colleagues showed a survival advantage with high-dose melphalan plus ASCT versus consolidation with melphalan, prednisone, lenalidomide after IMiD-based doublet induction. 11 However, these two subgroups were not a part of the original four-group design of the study. Also, a recent study by Attal and colleagues showed that the use of ASCT after induction with a triplet regimen using a combination of PIs and IMiDs delays progression but doesn’t improve OS. 14 Therefore, although ASCT is considered a part of initial therapy, delaying the same until relapse remains an acceptable approach.
Eligibility for transplant
The eligibility for ASCT varies widely among countries, but is based largely upon patient’s age, comorbidities and performance status. In the United States, the upper age limit is flexible up to 75 years for patients with adequate organ function, but in Europe and most other countries, ASCT is performed till the age of 65 years. 15 ASCT is usually avoided for patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 3 or 4 or a New York Heart Association functional status of class III or IV.
Timing of transplant
After stem-cell collection, the patients can either proceed with ASCT upfront (early ASCT) or continue with chemotherapy with a plan to pursue ASCT at the time of relapse (delayed ASCT). There have been various studies which compared the outcomes of early versus delayed ASCT, as shown in Table 2. Although the earlier studies reported an improvement in both PFS and OS with the use of ASCT in initial therapy, 16 the incorporation of novel therapies as triplet regimens in the first-line treatment resulted in an improvement in PFS which did not translate into an OS benefit with early ASCT as compared with delayed ASCT. 14
Early versus delayed ASCT.

ASCT, autologous stem-cell transplant; CR, complete response; NR, not reached; NS, non-significant; R, revilimid; RD, revilimid, dexamethasone; T, thalidomide; TD, thalidomide, dexamethasone; V, Velcade; VAMP, vincristine, adriamycin, melphalan, prednisolone; VGPR, very good partial response; VMCP, vincristine, melphalan, cyclophosphamide, prednisolone; VRD, Velcade, revilimid, dexamethasone.
Induction therapy
Patients eligible for ASCT are given induction therapy for 2–4 m prior to stem-cell collection, in order to reduce the tumor burden, to improve the quality of the graft, lessen symptoms, and diminish end-organ damage.
In the past, melphalan-containing regimens were avoided due to their hematopoietic toxicity and increased risk of myelodysplasia following transplantation. The induction regimen was either dexamethasone based or a combination of steroids with non-alkylators like the vincristine, doxorubicin and dexamethasone (VAD) regimen. 20
In the era of novel therapies, the most commonly used regimens for initial treatment include bortezomib, dexamethasone and lenalidomide (VRD), bortezomib, thalidomide and dexamethasone (VTD), bortezomib, cyclophosphamide and dexamethasone (VCD), and carfilzomib, lenalidomide, dexamethasone (KRD).21–23 Two studies showed the superiority of the triplet regimen, like VRD, over the doublet regimen, like thalidomide–dexamethasone (TD) 24 and bortezomib–dexamethasone (VD) in achieving a better PFS and OS. 21 Other studies have reported improved responses and delayed progression with the use of VTD over other doublet regimens.25,26 Among the triplet regimens, a regimen containing both a PI and an IMiD like VTD and VRD was found to be superior to VCD.21,23
The data concerning impact of the response to induction therapy on outcomes after ASCT remains limited. The Intergroupe Francophone de Myelome (IFM) group evaluated 482 patients enrolled in the IFM 2005-01 trial of induction therapy followed by early ASCT. They found that patients who achieved a very good partial response (VGPR) or better after induction chemotherapy had a longer PFS as compared with those who achieved a VGPR after ASCT (41 m versus 31 m, p = 0.01). 27
Stem-cell mobilization
Apheresis is performed with a goal of collecting a minimum of 2 × 106 CD34+ cells/kg and an optimal dose of 5 × 106 CD34+ cells/kg. 28
The standard regimen used for stem-cell mobilization is granulocyte colony stimulating factor (G-CSF) or G-CSF with cyclophosphamide.29,30 Plerixafor, a chemokine receptor type 4-inhibitor, is mostly reserved for the patients who fail to collect stem cells to G-CSF and G-CSF/cyclophosphamide.31,32
In addition, it should be noted that there have been some data to suggest that prolonged initial therapy with a lenalidomide-based regimen may impair hematopoietic stem-cell collection. Hence, an early mobilization of stem cells, preferably within the first four cycles of initial therapy with lenalidomide is recommended. 33
Conditioning regimen
The standard preparative conditioning regimen used for ASCT in MM is melphalan at a dose of 200 mg/m2, with dose reductions based on age and renal function. In a randomized controlled trial by the IFM group, patients who received melphalan at 200 mg/m2 had a higher survival at 45 m (65.8% versus 45.5%, p = 0.05) with significantly faster hematologic recovery, lower rate of severe mucositis and shorter hospitalizations as compared with those who received melphalan at 140 mg/m2 with 8 Gy total body irradiation (TBI). 34
The impact of reducing the dose of conditioning melphalan on outcomes of patients with MM has been evaluated. Palumbo and colleagues randomized 298 patients to receive tandem ASCT after conditioning with melphalan at a dose of 200 and 100 mg/m2. Melphalan at 200 mg/m2 resulted in a longer PFS (31.4 m versus 26.2 m, p = 0.01) and a trend towards improved OS at 5 years (62% versus 48%, p = 0.13) as compared with 100 mg/m2. The treatment-related mortality was similar in both the groups (3.1% versus 2.9%). 35
There have been several attempts to study the effect of intensification of preparative regimens before ASCT. Studies using conditioning with cyclophosphamide and melphalan (BCNU), etoposide, cytarabine, and melphalan (BEAM), 36 high-dose idarubicin, cyclophosphamide, and melphalan, 37 thiotepa, busulfan, and cyclophosphamide, 38 and busulfan and melphalan 39 did not result in better outcomes while increasing the incidence of toxicities as compared with melphalan at 200 mg/m2. Ongoing trials are currently testing whether outcomes can be improved by augmenting the conditioning with use of newer agents, especially in patients with relapses. Three phase I/II trials used escalated doses of bortezomib along with melphalan as conditioning in patients undergoing ASCT. The overall response rate (ORR) in these studies ranged from 44% to 87% with 51–70% of the patients achieving VGPR or better without any increase in hematological toxicity.40–42 A phase I trial showed that high-dose lenalidomide in combination with melphalan may offer significant potential as a conditioning regimen before ASCT in patients with relapsed MM. 43
Transplant-related toxicity
Savani and colleagues evaluated the complications among 6957 patients with MM who underwent ASCT from 1998 to 2011 in United States using the Nationwide Inpatient Sample (NIS) database. The most common in-hospital complications included stomatitis (44.7%), anemia requiring transfusion (28.5%), febrile neutropenia (16.5%) and bacteremia (15.0%). Despite temporal increase in mean age and comorbidities of patients undergoing ASCT, transplant-related mortality (TRM) reduced (2.9% versus 0.7%, p < 0.01) significantly from 1998 to 2011. Higher Charlson comorbidity index, female sex and use of TBI were associated with higher complications, while mechanical ventilation, acute respiratory failure, acute kidney injury, bacteremia and use of TBI predicted in-hospital mortality post ASCT. 44 Various studies have shown that ASCT can be conducted safely as an outpatient procedure. This not only leads to reduction in morbidity but also provides better cost effectiveness.45–47 At the Mayo clinic, a multidisciplinary model involving nurses, physicians, pharmacists and dieticians and utilizing an electronic database for ordering diagnostic tests and chemotherapy was used in 716 patients undergoing ASCT. A total number of 278 patients treated in an outpatient setting with this model had a 100-day survival rate of 98.9% (99.5% for low risk and 97.2% for high risk). 47
Consolidation therapy
The data regarding the use of consolidation post ASCT in an effort to improve outcomes by deepening the response are limited. Ladetto and colleagues showed that the use of VTD in patients achieving VGPR or better post ASCT led to an increase in CR rates from 15% to 49% and molecular remission from 3% to 18%. 48 However, it was not known whether this deepening of response influenced survival and progression. A recent per-protocol analysis of the Italian myeloma study showed that consolidation with VTD post ASCT resulted in increased CR rates (60.6% versus 46.6%) and prolonged 3-year PFS (62% versus 42%, p = 0.042) as compared with TD. 49 The Nordic Myeloma Study Group randomized bortezomib-naïve patients to bortezomib versus no consolidation after ASCT. There was a trend towards an improvement in PFS (27 m versus 20 m, p = 0.05), but there was no difference in OS between both the groups. 50
Maintenance therapy
Maintenance therapy with lenalidomide and bortezomib appears to be promising in the post-ASCT scenario. Two randomized studies established that the use of low-dose lenalidomide after ASCT until progression led to an improvement in PFS (41 m versus 23 m, p < 0.001 and 50 m versus 27 m, p < 0.001) which also translated into an OS benefit (3 years, 88% versus 80%) in one of the studies. This survival benefit was largely limited to patients who received lenalidomide as induction therapy.51,52 A meta-analysis of 1208 patients also confirmed an improvement in OS (not reached versus 86 m, p = 0.001) with lenalidomide maintenance, but the risk of second primary malignancies was increased (hematological, 6.1% versus 2.8% and solid, 7.3% versus 4.2%). 53 Also, it should be noted that the abovementioned trials did not have a planned crossover in which the placebo arm was treated with lenalidomide upon relapse. In all these studies, lenalidomide was superior to the comparator arm but it cannot be recommended to all patients because the OS benefit has not been widely established and because of concerns of long-term safety. Two randomized trials have also evaluated the role of bortezomib maintenance after ASCT. In the Dutch–Belgian Hemato-Oncology Cooperative Group (HOVON) 65/German Multicenter Myeloma Group (GMMG)-HD4 trial, bortezomib maintenance for 2 years resulted in improved PFS (35 m versus 28 m, p < 0.001) as compared with thalidomide maintenance, especially in patients with renal failure, 13q deletion and 17p deletion. 54 Another study by the Spanish myeloma (PETHEMA) group showed a significant PFS benefit for bortezomib–thalidomide maintenance as compared with thalidomide or interferon-α2b alone. 55 Although these results indicate a benefit for bortezomib maintenance, they are complicated by multidrug treatment during induction and maintenance. Further randomized studies are needed before this can be recommended.
Single versus tandem transplant
With tandem (double) ASCT, patients receive a planned second transplant after recovery from the first procedure. Various studies have been conducted comparing single with tandem ASCT, as shown in Table 3. Earlier studies found a significant improvement in PFS and OS with single transplant versus tandem ASCT. This benefit was largely restricted to patients who did not achieve VGPR or better with the first transplant. 15 With the incorporation of novel therapies as induction prior to ASCT, the majority of patients achieved a deep response. Hence, the role of tandem transplant has become limited over the past decade. Also, a meta-analysis of 1803 patients concluded that tandem transplant was not associated with any advantage in PFS and OS over a single transplant. The response rate was statistically significantly better with tandem ASCT (risk ratio 0.79, 95% CI 0.67–0.93), but with a statistically significant increase in transplant-related mortality (TRM; risk ratio 1.71, 95% CI 1.05–2.79). 56 Despite these results, there has been some evidence that patients with high-risk cytogenetics like 17p deletion do benefit with a tandem transplant.54,57
Single versus tandem ASCT.

ASCT, autologous stem-cell transplant; CR, complete response; VGPR, very good partial response.
Transplant as salvage therapy
Second ASCT is a safe and effective therapy in eligible patients with relapsed MM. Alvares and colleagues found that patients with a PFS of <18 m after first ASCT had a median OS of <6 m whereas those with a PFS of ⩾18 m showed a median OS approaching 3 years. 63 A Mayo Clinic study which reviewed 345 patients who relapsed after ASCT found that the median OS was 10.8 m for patients in the early relapse group (⩽12 m from ASCT) as compared with 41.8 m in the late relapse group (>12 m from ASCT; p < 0.001). Hence, the authors recommended offering novel trials for patients in the early relapse group due to poor outcomes. 64 Sellner and colleagues evaluated 200 patients with MM who relapsed after upfront ASCT and were treated with a second transplant at salvage therapy. The ORR was 80.4% at day 100, while the median PFS and OS after salvage ASCT were 15.2 m and 42.3 m, respectively. Factors associated with improved survival after salvage ASCT included an initial PFS of >18 m after upfront ASCT, bortezomib-containing or lenalidomide-containing therapies for reinduction, response to reinduction, and an International Staging System stage I before salvage ASCT. 65 Most of these studies are based on single-arm data and a Center for Inter-national Blood and Marrow Transplant Research (CIBMTR) study is underway which may provide cut offs for duration of remission to undergo salvage transplant. Also, it should be noted that recent clinical trials have shown impressive results with the use of triplet therapy like the carfilzomib, lenalidomide and dexamethasone (KRD) regimen and daratumumab, lenalidomide and dexamethasone (DRD) regimen in patients with relapsed/refractory MM.66,67 Hence, the benefit of ASCT in patients with relapsed myeloma may be of limited value with the availability of highly efficacious triplet regimens using novel agents.
Role in special populations
Autologous stem-cell transplantation in elderly patients
With improvement in supportive care, the percentage of MM patients aged 70 years and above undergoing ASCT has increased from 6% in 1994–1995 to 25% in 2004–2005. 68 However, there remains a paucity of prospective studies among this patient population owing to exclusion of elderly patients from most randomized trials based on their selection criteria.
Stem-cell mobilization is scant in the elderly population, with a need for more apheresis sessions. 69 Plerixafor has been found to be promising in this situation. 70 The other concern is their ability to withstand the toxicity incurred with myeloablative regimens. Most of the studies done in elderly population have used reduced doses of conditioning melphalan. A retrospective study evaluated survival after ASCT in patients over the age of 70 years. The rate of CR was 20 and 27% after a single or tandem ASCT with a median OS of 13 and 33 m, respectively. Treatment-related mortality was 16% in patients receiving conditioning melphalan at a dose of 200 mg/m2 of melphalan and 2% in patients receiving 140 mg/m2. 71 The CIBMTR analyzed 11,430 MM patients who underwent ASCT between 2008 and 2011. The 3-year PFS and OS were at 42% and 78% for patients in age group 18–59 years, 38% and 75% in age group 60–69 years, and 33% and 72% in age group >70 years, respectively. In a multivariate analysis, increasing age was associated with worse survival (p = 0.0006). 72 Palumbo and colleagues used a scoring system based on age, comorbidities, and cognitive and physical conditions to categorize elderly patients in three groups, namely, fit, intermediate fit and frail, and found that their 3-year OS rates were 84%, 76% and 57%, respectively. 73 However, the relevance of this scoring system has not been demonstrated on the outcomes of the patients undergoing ASCT.
Autologous stem-cell transplantation in renal impairment
In a study of 81 MM patients with serum creatinine > 2 mg/dl who underwent ASCT, it was showed that renal failure has no impact on the quality of stem-cell collections and engraftment. Early TRM was seen in 7% of patients who received melphalan at a dose of 200 mg/m2 (MEL-200) and in 5% of those who received a dose of 140 mg/m2 (MEL-140). All patients had grade III–IV neutropenia, thrombocytopenia and fever. Mucositis was seen in 93% of patients, while vomiting and diarrhea affected 67% of the patients. Mucositis, pulmonary complications, cardiac complications, specifically atrial dysrhythmias, and neurological complications, particularly encephalopathy, were more frequent in the MEL-200 group as compared with the MEL-140 group. Hence, ASCT is feasible in patients with creatinine > 2 mg/dl; the toxicities are more severe and more frequent. It was also found that conditioning with melphalan at a dose of 140 mg/m2 was equally efficacious and had a better toxicity profile as compared with 200 mg/m2 in this patient population. 74 The CIBMTR also studied 1492 MM patients who underwent ASCT for MM between 2008 and 2013. Among these, 1240 patients had normal/mild (⩾60 ml/min) renal insufficiency (RI), 185 patients had moderate RI (30–59 ml/min), and 67 patients had severe RI (<30 ml/min), based on modification of diet in renal disease. It was found that the 5-year PFS for normal, moderate and severe RI was 35%, 40% and 27%, respectively, (p = 0.42); while the 5-year OS was 68%, 68% and 60%, respectively, (p = 0.69). 75
Allogenic stem-cell transplant in multiple myeloma
The only therapy with a potential to produce cure in patients with MM is allogenic stem-cell transplant. The advantages of using an allogeneic graft are the absence of tumor cells and its ability to produce a graft versus myeloma effect. 76 The results from data comparing the efficacy of allogenic stem-cell transplant with ASCT have been conflicting. Krishnan and colleagues evaluated 625 patients with standard-risk MM who received a myeloablative ASCT followed by a nonmyeloablative allogeneic transplant (n = 189, those with matched sibling donor) and tandem ASCT (n = 436, those without a donor). The 3-year PFS (46% versus 43%) and OS (80% versus 77%) were similar between both the groups. Even in a subgroup of 85 patients with high-risk MM, there was no benefit to ASCT followed by nonmyeloablative allogeneic HCT. 77 The PETHEMA group also confirmed that there is no survival benefit with the use of reduced-intensity allogeneic transplant as compared with a second ASCT in patients who failed to achieve a VGPR after first ASCT. 78 In contrast, two other studies have shown an improvement in PFS and OS with nonmyeloablative allogeneic transplantation after ASCT as compared with tandem ASCT.79,80 It should be noted in all these trials, the treatment-related mortality is approximately 10–20% and the rates of acute and chronic graft versus host disease are high. At present, allogenic transplant is reserved for young patients with high-risk myeloma in first or second relapse who are willing to accept the high treatment-related morbidity and mortality risk. 2
Summary
ASCT remains an integral part of treatment for previously untreated, and may have value in the treatment of relapsed patients with, MM. The addition of novel agents before and after ASCT have led to an improvement in CR rates, delay in progression and prolonged OS. Ongoing studies are looking at how the newer drugs can be incorporated in the treatment paradigm as a part of initial therapy, or as conditioning or as consolidation/maintenance to further improve outcomes.