
Abstract
Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 receptor antagonist represents the current standard of care to prevent atherothrombotic recurrences in patients with acute coronary syndrome (ACS). However, despite the use of DAPT, the recurrence rate of cardiovascular ischemic events still remains high. This persistent risk may be in part attributed to the sustained activation of the coagulation cascade leading to generation of thrombin, which may continue to play a key role in thrombus formation. The use of vitamin K antagonists (VKAs) as a strategy to reduce atherothrombotic recurrences after an ACS has been previously tested, leading to overall unfavorable outcomes due to the high risk of bleeding complications. The recent introduction of non-VKA oral anticoagulants (NOACs), characterized by a better safety profile and ease of use compared with VKA, has led to a reappraisal of the use of oral anticoagulant therapy for secondary prevention in ACS patients. The present article provides an overview of the rationale and prognostic role of oral anticoagulant therapy in ACS patients as well as recent updated clinical data, in particular with NOACs, in the field and future perspectives on this topic.
Keywords
Introduction
Cardiovascular disease in general and the development of an acute coronary syndrome (ACS) in particular is among the leading causes of morbidity and mortality. 1 The main pathophysiological mechanism leading to an ACS is represented by thrombus formation in the coronary artery following erosion or rupture of an atherosclerotic plaque. 2 After initial plaque erosion/rupture, a cascade of events driven by cellular (i.e. platelets) and plasma (i.e. coagulation factors) components leading to thrombus formation has a pivotal role in this process. Thrombus formation in the coronary artery ultimately culminates in complete or partial vessel occlusion contributing to the constellation of signs and symptoms that characterize patients presenting with an ACS.2–4 In particular, most patients presenting with an ST-segment-elevation myocardial infarction (STEMI) have a completely occluded coronary artery, while patients with non-ST-segment elevation ACS (NSTE-ACS) are more commonly characterized by partial vessel occlusion. 2
These pathophysiological considerations underscore how inhibition of both platelets and coagulation factors are essential for the treatment and secondary prevention of ACS patients. Dual antiplatelet therapy (DAPT) including aspirin and a P2Y12 receptor antagonist represents the gold standard antithrombotic treatment regimen to prevent atherothrombotic recurrences.5,6 Currently, three oral P2Y12 receptor inhibitors including clopidogrel, prasugrel and ticagrelor are approved for clinical use in ACS patients.7–9 Prasugrel and ticagrelor are characterized by enhanced potency over clopidogrel and better net clinical outcomes in ACS patients.7,8 Accordingly, guidelines support their preferential use in ACS settings.10–13 Anticoagulant therapy, typically parenteral agents, is commonly used in the acute phase of ACS presentations. However, following the introduction of DAPT, the use of oral anticoagulant therapy, in particular vitamin K antagonists (VKAs), for long-term management of ACS patients has been largely abandoned. Nonetheless, the recent introduction of non-VKA oral anticoagulants (NOACs), characterized by a better safety profile and ease of use compared with VKAs, has led to a reappraisal of the option of using oral anticoagulant therapy for secondary prevention in ACS patients. 14
The present manuscript will present an overview of the rationale and potential role of oral anticoagulant therapy in patients with ACS, as well as the available clinical data in the field and future perspectives on this topic. The use of oral anticoagulants for other indications, including atrial fibrillation (AF), among patients with coronary artery disease (CAD) will not elaborated in this manuscript and is described in details elsewhere.15,16
Platelet activation and coagulation cascade
Thrombus formation after rupture or erosion of an atherosclerotic plaque in the arterial wall is known to be the main pathophysiological mechanism leading to the development of an ACS.2–4 After plaque rupture or superficial erosion, a cascade of events consisting of platelet adhesion, activation and aggregation in conjunction with thrombin formation contributes to thrombus formation and vascular occlusion.2–4 In particular, von Willebrand factor (vWF) that binds to the collagen on the exposed extracellular matrix at the site of plaque rupture or erosion interacts with the glycoprotein (GP) Ib/V/IX receptor complex on the platelet surface.3,4,17,18 Subsequently, collagens from the subendothelium at the site of vascular injury bind to GP VI on the platelet surface. This leads to conformational changes in platelet structure and release of various factors which promote platelet activation, including thromboxane A2 (TxA2), adenosine diphosphate (ADP) and thrombin.3,4,18 The final process of platelet activation is represented by the conformational change of the platelet GP IIb/IIIa receptor to its active form, which allows it to bind to fibrinogen, promoting platelet aggregation and contributing to final thrombus formation (Figure 1).
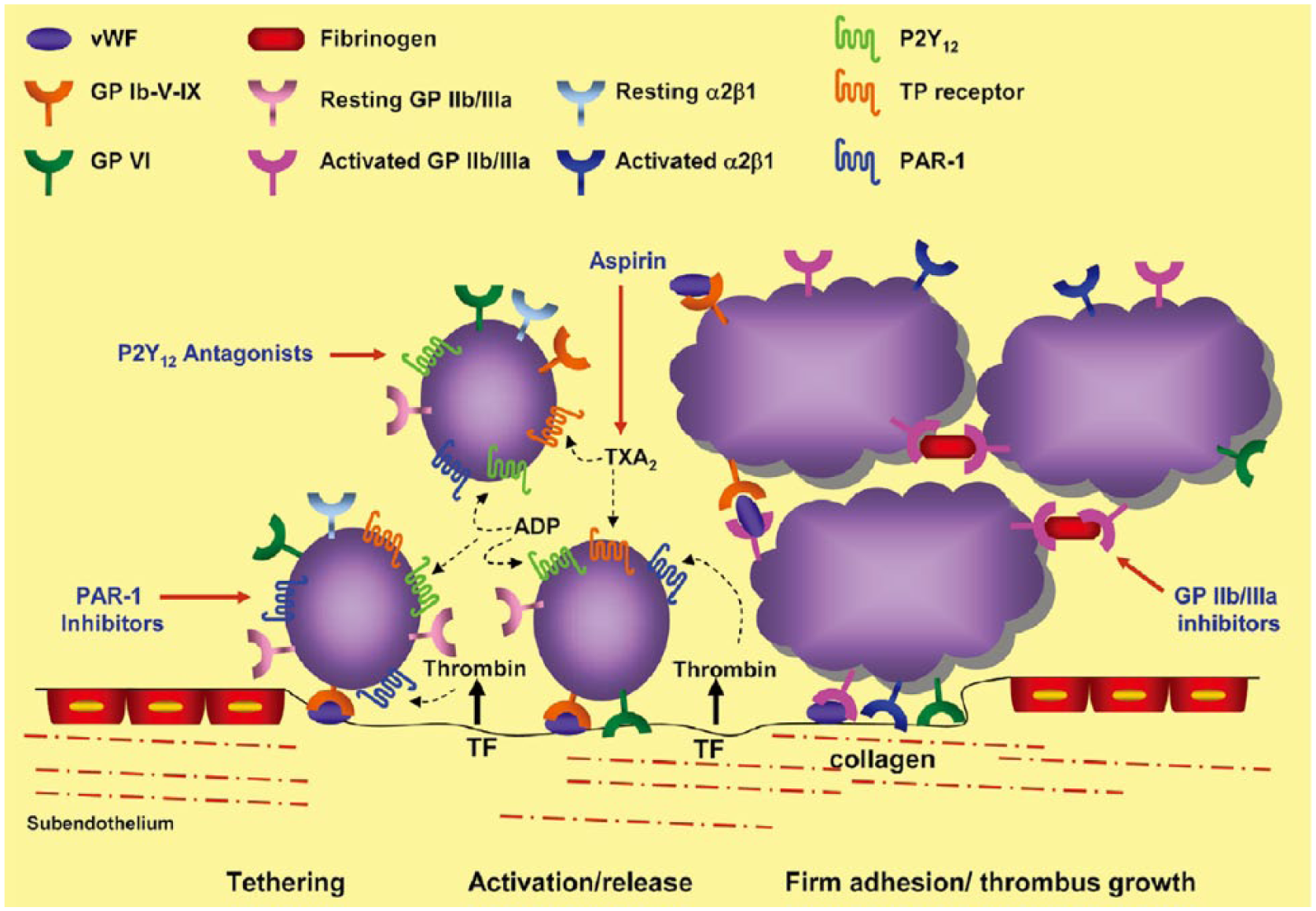
The process of platelet adhesion and aggregation.
In parallel with the platelet cascade described above, the exposed extracellular matrix also induces activation of the coagulation cascade which leads to thrombin generation.4,19 Tissue factor (TF), locally exposed to the plasma at the site of plaque rupture, binds to Factor VIIa (FVIIa) to form an activated TF/FVIIa complex. This complex activates Factor IX and Factor X into Factor IXa and Factor Xa. The following combination of Factor IXa and Factor VIIIa form the intrinsic tenase (FVIIIa/FIXa), which contributes to the conversion of Factor X to Factor Xa (FXa). FXa and Factor Va lead to formation of the prothrombinase complex (FVa/FXa), which cleaves Factor II (prothrombin) to generate Factor IIa (thrombin).20,21 In the propagation phase of the coagulation cascade, both the FVIIIa/FIXa and FVa/FXa complexes gather on the activated platelet surface and promote the burst in thrombin generation (Figure 2). Thrombin is a serine protease and has multifunctional properties in thrombus formation. Thrombin mediates the conversion of fibrinogen to fibrin, which is essential to form a thrombus. In particular, fibrin monomers polymerize to form a fibrin-rich clot and this clot is stabilized by crosslinking with Factor XIIIa. In addition, thrombin plays an essential role in platelet activation via binding to protease activator receptors (PARs)-1 on the platelet membrane.22,23

The cell surface-based coagulation process.
Rationale for anticoagulation therapy in ACS patients
Thrombin generation plays a key role in the pathophysiology of ACS. In particular, thrombin contributes to platelet activation, enhancing activation of the coagulation cascade, overall favoring thrombus formation and its associated complications. 22 Therefore, anticoagulant therapy is critical in the acute care of ACS patients. Currently, various parenteral anticoagulant agents are available for clinical use in the acute setting of ACS. These include heparin (unfractionated form and low molecular-weight heparin), bivalirudin (a direct thrombin inhibitor) and fondaparinux (a direct Factor Xa inhibitor). 24 However, these agents are used only for a short period of time, essentially for the in-hospital phase of care of ACS patients. Conversely, the use of oral anticoagulant drugs has not traditionally been part of the long-term management of ACS patients, particularly after the introduction of current regimens of standard DAPT.
The rationale for supporting the use of DAPT in patients experiencing an ACS is represented by the fact that thrombotic complications after an ACS have been primarily considered a platelet-mediated process.5,6 Currently, three oral P2Y12 receptor inhibitors – clopidogrel, prasugrel and ticagrelor – are approved for clinical use in ACS patients.7–9 Prasugrel and ticagrelor are characterized by enhanced potency over clopidogrel and better net clinical outcomes in ACS patients.7,8 Accordingly, guidelines support their preferential use in ACS settings.10–13 However, regardless of the use of optimal DAPT regimens including prasugrel and ticagrelor, recurrence rates of cardiovascular ischemic events still remain high. 1 This persistent risk may be in part attributed to the sustained generation of thrombin, which play a key role in thrombus formation. Several studies in fact support that thrombin generation is persistently high in ACS patients after an acute episode.25–27 Biomarkers of persistent activation of the coagulation system, such as prothrombin fragment 1 + 2, D-dimer have been shown to be associated with worse clinical outcomes. 28 These findings indicate that thrombotic complications may not be prevented by antiplatelet therapy alone and support the potential need for long-term oral anticoagulant therapy to inhibit thrombin generation. The use of anticoagulant therapy for long-term management of ACS patients, in particular VKA, has been largely abandoned with the use of DAPT. However, the recent introduction of NOACs, characterized by a better safety profile and ease of use compared with VKA, has led to a reappraisal of the need for using oral anticoagulant therapy for secondary prevention in ACS patients, as described below. 14
Vitamin K antagonists for the patients of ACS
In the 1940s, intravenous unfractionated heparin was used for the treatment of patients with myocardial infarction (MI). Then VKAs were used as oral anticoagulant therapy and had represented the only oral agents for several decades. 29 Warfarin, a representing drug of the VKA class, inhibits multiple enzyme in the coagulation cascade, including Factor II (prothrombin), Factor VII, Factor IX, Factor X, protein C and protein S. However, warfarin has several limitations including drug–drug and food–drug interactions, need for frequent monitoring, delayed onset and offset of action (due to indirect action and long half-life), and genetic variability in liver enzyme metabolism. 30 Although warfarin has been the cornerstone of oral anticoagulation therapy for the prevention of stroke in patients with AF for several decades, its role in the treatment of atherosclerotic events such as ACS is not clear.31–33 The AFTER (aspirin and anticoagulation following thrombolysis with eminase in recurrent infarction) study did not show any benefit of warfarin monotherapy compared with aspirin 150 mg monotherapy in post-MI patients. 34 Thereafter, warfarin monotherapy without aspirin in post-MI patients was largely abandoned. 35 There were several large-scale randomized clinical trials comparing aspirin monotherapy with dual therapy of aspirin plus warfarin. Among these, the CARS (the Coumadin aspirin reinfarction study) and CHAMP (the combination hemotherapy and mortality prevention) studies were conducted in a relatively large number of participants. The CARS study evaluated the role of warfarin among 8803 patients with recent MI (3–21 days after index MI). Patients were randomly assigned to three groups: 160 mg of aspirin monotherapy, 80 mg of aspirin and 1 mg of warfarin, 80 mg of aspirin and 3 mg of warfarin. 31 After a median of 14 months, the addition of warfarin to aspirin did not provide any benefit in the reduction of rates of cardiovascular events beyond that achieved from 160 mg of aspirin monotherapy (one year estimated event rate, 8.6% in 160 mg of aspirin monotherapy, 8.8% in 80 mg of aspirin + 1 mg of warfarin, and 8.4% in 80 mg of aspirin + 3 mg of warfarin) and showed increased rates of major bleeding. The CHAMP study also compared a combination therapy of warfarin and aspirin (81 mg) to aspirin monotherapy (162 mg) in 5059 patients with a recent MI for a median follow up of 2.7 years. 32 Combination therapy did not demonstrate a reduction of cardiovascular events compared to aspirin monotherapy and the addition of warfarin was significantly associated with an increased risk of bleeding (1.28 versus 0.72 events, per 100 person years, p < 0.001). In a meta-analysis including 14 studies enrolling 25,307 MI patients, as compared with aspirin monotherapy, combination of warfarin and aspirin was associated with a 27% relative risk reduction in the rates of all-cause death, non-fatal MI or stroke only when INR targets were between 2.0 and 3.0; however, this occurred at the expense of increased major bleeding. 36
Overall, the addition of warfarin to aspirin monotherapy does not provide the clinical benefits desired for the prevention of secondary events in ACS patients, largely due to the increased risk of bleeding complications. There are no available data of combined therapy with warfarin and clopidogrel as well as with newer-generation P2Y12 receptor inhibitors such as ticagrelor and prasugrel. There is also limited evidence on the use of ‘triple therapy’ (combination of warfarin with DAPT), which, however, has shown to be associated with a high risk of major bleeding in registry data and thus is not recommended for secondary prevention of ACS. 35
Non-vitamin K antagonist oral anticoagulants
Since VKAs inhibit the synthesis of coagulation factors which are dependent on vitamin K, VKAs are called indirect oral anticoagulants. On the other hand, NOACs act directly on their target (i.e. FXa or thrombin) and are thus called direct oral anticoagulants. 37 Because of these properties, their anticoagulation effect is more prompt and they also have more rapid offset of action compared with warfarin. Direct thrombin inhibitors directly bind to thrombin and prevent conversion of fibrinogen into fibrin. 38 Ximelagatran and dabigatran etexilate were tested in clinical trials, and currently dabigatran etexilate is the only oral direct thrombin inhibitor used in clinical practice for prevention of stoke in AF patients, as well as treatment and prevention of venous thromboembolism (VTE). 39 The other group of NOACs is represented by the direct FXa inhibitors. FXa is upstream to prothrombin and its inhibition contributes to the down-regulation of thrombin generation. The role of FXa inhibition in ACS patients is supported by the result from parenteral use of the indirect FXa inhibitor fondaparinux in two large studies in the acute care setting.40,41 Contrary to indirect agents, cofactors, like antithrombin III, are not required for the action of the direct FXa inhibitors which directly target FXa activity. 21 The oral direct FXa inhibitors, including apixaban, rivaroxaban and edoxaban, are currently used for the prevention of stoke in AF patients and prevention/treatment of VTE. 39 Other oral FXa inhibitors including darexaban, letaxaban and betrixaban have been investigated in phase II clinical trials. However, of all the clinically available NOACs, only rivaroxaban has successfully completed phase III investigation meeting its primary endpoint in ACS patients and has received approval for clinical use for this indication. The individual results of clinical trials for anticoagulation in CAD are be described in detail below (Table 1).
Phase II dose-escalation, clinical trials for the safety and efficacy of NOAC in ACS patients.
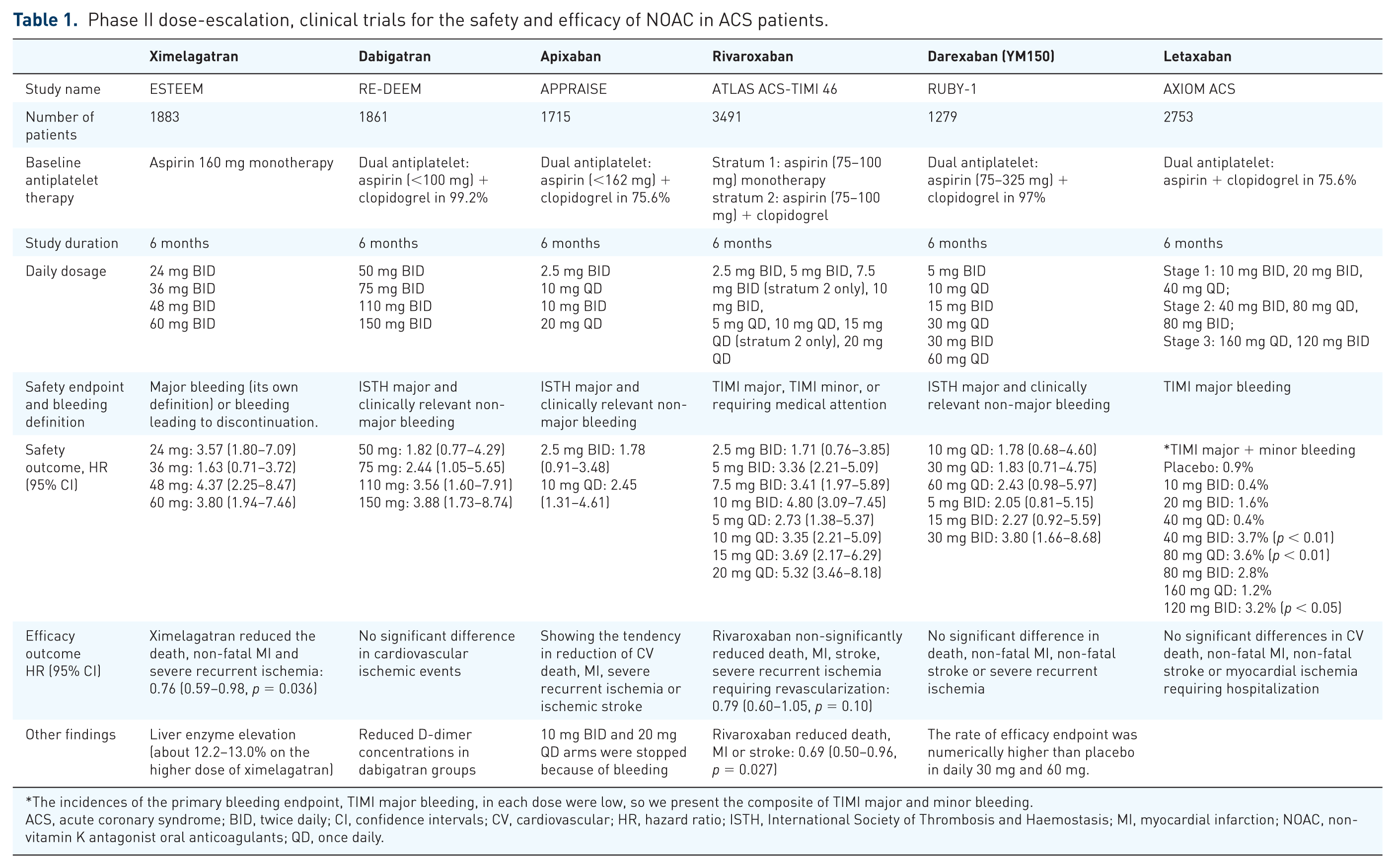
The incidences of the primary bleeding endpoint, TIMI major bleeding, in each dose were low, so we present the composite of TIMI major and minor bleeding.
ACS, acute coronary syndrome; BID, twice daily; CI, confidence intervals; CV, cardiovascular; HR, hazard ratio; ISTH, International Society of Thrombosis and Haemostasis; MI, myocardial infarction; NOAC, non-vitamin K antagonist oral anticoagulants; QD, once daily.
Ximelagatran
Ximelagatran, an oral direct thrombin inhibitor, is the first NOAC that has been studied for the reduction of ischemic recurrences in ACS patients. After oral administration, ximelagatran is rapidly converted to its active form, melagatran. 42 The ESTEEM trial (The efficacy and safety of the oral direct thrombin inhibitor ximelagatran in patients with recent myocardial damage trial) explored the safety and efficacy of ximelagatran in ACS patients. 43 A total of 1883 ACS patients (within 14 days of the index event) were randomly assigned to ximelagatran [at twice daily doses (BID) of 24 mg, 36 mg, 48 mg or 60 mg] or placebo. Approximately, two-thirds of the total study population were STEMI and about half of these were treated with thrombolytic therapy. Almost all patients received 160 mg of aspirin. However, this study does not reflect current practice. For example, percutaneous coronary intervention (PCI) performed in the past four months or planned within two months of randomization were excluded. Patients needing adjunctive oral antiplatelet therapy, including P2Y12 receptor inhibitors, and anticoagulants were excluded. In the trial, the combination of ximelagatran and aspirin significantly reduced the primary endpoint (defined by composite all-cause death, non-fatal MI and severe recurrent ischemia) compared with aspirin alone (HR 0.76, 95% CI 0.59–0.98, p = 0.036) with a 3.6% absolute risk reduction of the primary endpoint (12.7%, ximelagatran versus 16.3%, placebo). The frequency of major bleeding was numerically higher in the ximelagatran group (1.8% versus 0.9%, HR 1.97, 95% CI 0.80–4.84). However, elevation in liver enzymes occurred with ximelagatran (about 12.2–13.0% on the higher dose of ximelagatran). Because of liver toxicity, ximelagatran was withdrawn from commercialization.
Dabigatran
Dabigatran is the only oral direct thrombin inhibitor available for clinical use. 39 After oral administration of the pro-drug of dabigatran etexilate, the serum esterase rapidly converts dabigatran etexilate into dabigatran. The efficacy and safety of dabigatran in ACS patients was investigated in the phase II, dose-ranging RE-DEEM (randomized dabigatran etexilate dose finding study in patients with acute coronary syndromes post index event with additional risk factors for cardiovascular complications also receiving aspirin and clopidogrel) trial. 44 A total of 1861 patients with recent STEMI or NSTEMI were randomly assigned to different doses of dabigatran (dabigatran 50 mg BID, 75 mg BID, 110 mg BID, 150 mg BID) or placebo. At the time of randomization, 99.2% of patients were already on DAPT with aspirin plus clopidogrel and 83.8% of patients continued DAPT until the end of the study. The primary endpoint of this study was the rate of major and clinically relevant minor bleeding. The assessment of major bleeding was based on the International Society of Thrombosis and Haemostasis (ISTH) definition. There was a dose-dependent increase in the rate of the primary endpoint compared to placebo (2.2% in placebo group, 3.5% in 50 mg BID group, 4.3% in 75 mg BID, 7.9% in 110 mg BID and 7.8% in 150 mg BID). Dabigatran was not associated with any ischemic benefit. It significantly reduced coagulation activity, such as D-dimer concentration. 44 Further investigations, including phase III, of dabigatran in ACS patients have not been conducted after the RE-DEEM trial.
Apixaban
Apixaban is a selective direct-acting FXa inhibitor which affects both free and prothrombinase-bound FXa. 39 The half-life of apixaban is approximately 12 h and it is eliminated through multiple pathways, including hepatic metabolism, renal clearance and biliary secretion. 39 The safety and efficacy of apixaban in ACS patients were explored in the phase II, dose-ranging APPRAISE trial. 45 APPRAISE enrolled 1715 patients with recent STEMI or NSTE-ACS. Aspirin was used in almost all patients and clopidogrel was used in 76% of cases. Patients were randomly allocated to receive apixaban [one of four different doses; 2.5 mg BID, 10 mg QD (once daily), 10 mg BID, 20 mg QD] or placebo. The primary outcome was major bleeding (by ISTH definition) and clinically relevant non-major bleeding during 6-month clinical follow up. Apixaban 2.5 mg BID demonstrated a non-significant increase in the primary outcome compared to placebo (HR 1.78, 95% CI 0.91–3.48, p = 0.09) and the 10 mg QD dose resulted in a significant increase in the primary outcome (HR 2.45, 95% CI 1.31–4.61, p = 0.005). Both the 10 mg BID and 20 mg QD arms were stopped due to excess bleeding. Although apixaban showed dose-dependent increased bleeding, a trend in reducing ischemic events was also demonstrated. Overall, the addition of apixaban to ACS patients treated with DAPT was associated with dose-related increase in bleeding events, with modest benefit in the reduction of ischemic events (rate of ischemic event; 7.6% in 2.5 mg BID, 6.0% in 10 mg QD, 8.7% in placebo).
Based on the result of the APPRAISE trial, a 5 mg BID dose of apixaban was investigated in addition to DAPT after an ACS event in the large-scale, phase III APPRAISE-2 trial. 46 Among the baseline characteristics of study participants, 59% of patients were ⩾65 years old, 47.8% of patients had diabetes mellitus, 10.0% of patients had a prior stroke and 28.9% of patients had impaired renal function. With a median follow up of approximately 8 months, TIMI major bleeding (primary safety outcome) occurred in 1.3% and 0.5% of patients in the apixaban and placebo groups, respectively (HR 2.59, 95% CI 1.50–4.46, p = 0.001). In addition, apixaban was associated with an increase in fatal bleeding events and intracranial bleeding (ICH) compared to placebo. There was no reduction in ischemic events with the primary efficacy outcome, defined as a composite of cardiovascular death, MI or ischemic stroke, occurring in 7.5% and 7.9% in the apixaban and placebo groups, respectively. After recruitment of 7392 participants, the APPRAISE-2 trial terminated prematurely because of increased bleeding without clinical benefits.
Rivaroxaban
Rivaroxaban is a highly selective, direct FXa inhibitor. 39 Similarly to apixaban, it inhibits both free FXa activity and prothrombinase-bound FXa activity. Rivaroxaban has a half-life of 5–9 h, and is eliminated through the renal (66%) and fecal/biliary systems (28%). The safety and efficacy of rivaroxaban in ACS patients (1–7 days after the index event) was explored in the phase II, dose-escalation ATLAS ACS-TIMI 46 trial. 47 This trial had two strata based on the antiplatelet treatment regimen used (stratum I: monotherapy of aspirin 75–100 mg; stratum II: dual therapy of aspirin 75–100 mg and clopidogrel). Patients (n = 3491) were randomized to placebo or different doses (5–20 mg) of rivaroxaban (2.5 mg BID, 5 mg BID, 7.5 mg BID, 10 mg BID, 5 mg QD, 10 mg QD, 15 mg QD, 20 mg QD). During the 6-month follow-up period, rivaroxaban showed a dose-dependent increase in clinically significant bleeding with a non-significant reduction in the primary efficacy endpoint (death, MI, stroke or severe recurrent ischemia requiring revascularization). However, the secondary efficacy endpoints (death, MI or stroke) was significantly decreased with rivaroxaban (HR 0.69, 95% CI 0.50–0.96, p = 0.027). A dose of 2.5 mg BID was the only regimen that did not show a statistically significant increase in bleeding risk (HR 1.71, 95% CI 0.76–3.85), while this was significantly increased with all other doses.
The findings from the ATLAS ACS-TIMI 46 trial identified the most suitable dosing regimens of rivaroxaban to be used in combination with DAPT, which were applied in the phase III, ATLAS ACS 2-TIMI 51 study. 48 In this trial, 15,526 patients with a recent ACS were randomized to either rivaroxaban (2.5 mg BID or 5 mg BID) or placebo. 46 Among the baseline characteristics of study participants, 36.5% of patients were ⩾65 years old, 32.0% had diabetes mellitus and 50.3% of patients were STEMI. Patients with a prior stroke were excluded. The median time from the index event to randomization was 4.7 days. Thienopyridines (clopidogrel or ticlopidine) were used as a background antiplatelet therapy in 93% of the patients. The trial showed a significant reduction in the primary efficacy endpoint (a composite of cardiovascular death, MI or stroke) with rivaroxaban compared with placebo after mean treatment duration of 13.1 months (8.9%, rivaroxaban versus 10.7%, placebo; HR 0.84, 95% CI 0.74–0.96, p = 0.008). In particular, both dosing regimens showed a significant reduction in the primary efficacy endpoint (8.8% in 5 mg BID and 10.7% in placebo, p = 0.03; 9.1% in 2.5 mg BID dose and 10.7% in placebo, p = 0.02). Most importantly, a survival benefit was achieved with the 2.5 mg BID regimen; in particular, there was a significant reduction in cardiovascular death (2.7% in 2.5 mg BID and 4.1% in placebo, p = 0.002) and death from any cause (2.9% in 2.5 mg BID dose and 4.5% in placebo, p = 0.002) (Figure 3). However, no survival benefit compared to placebo was demonstrated with the 5 mg BID regimen. Rivaroxaban was associated with a significant increase in non-coronary artery bypass grafting (CABG)-related major bleeding (2.1% in rivaroxaban and 0.6% in placebo, p < 0.001) and ICH (0.6% in rivaroxaban and 0.2% in placebo, p = 0.009). The rate of TIMI bleeding requiring medical attention was also increased with rivaroxaban (14.5% versus 7.5%, p < 0.001). Overall, the 5 mg BID dose was associated with more bleeding, including fatal bleeding (5 mg BID: 0.4% versus 2.5 mg BID: 0.1%, p = 0.004) compared with the 2.5 mg BID dose. The lower rate of fatal bleeding with the 2.5 mg BID dose may indeed have contributed to its survival benefit. Overall, the ATLAS ACS 2 trial demonstrated that the addition of low-dose rivaroxaban (2.5 mg BID regimen) to DAPT with aspirin and clopidogrel reduced recurrent cardiovascular events, including mortality, in patients with a recent ACS at the expense of three-fold increased major bleeding, but with no increase in fatal bleeding. To date, the only reported subgroup analysis of the ATLAS ACS 2 trial is that on patients with STEMI (n = 7817). In this analysis, rivaroxaban reduced the incidence of the primary efficacy endpoint consistently with the overall trial results (8.7% with 2.5 mg BID, 8.2% with 5 mg BID and 10.6% with placebo). 49 Rivaroxaban was also associated with an increase of major bleeding rate, but there was no significant increase in fatal bleeding in the STEMI subgroup.

The survival benefit of rivaroxaban 2.5 mg BID from the ATLAS ACS2 TIMI 51 trial.
The result of the two phase III trials, ATLAS ACS 2 and APPRAISE-2, which investigated the long-term use of NOACs in post-ACS patients are discordant. One probable reason for the conflicting results may be attributed to the characteristics of the study population. The study participants of APPRAISE-2 were older and had more comorbidities, including more diabetes and renal dysfunction. Importantly, patients with prior stroke who were excluded in ATLAS ACS 2 were enrolled in the APPRAISE-2 trial. The higher risk profile of patients enrolled in the APPRAISE-2 trial is also supported by the higher ischemic event rate. The second possible reason is the level of anticoagulant effects achieved in the two studies. The APPRAISE-2 trial tested 5 mg BID of apixaban, which is the same dose used for stroke prevention in AF patients. On the contrary, in ATLAS ACS 2 there was a survival benefit with the 2.5 mg BID daily dose, which is one-quarter of the total daily dose of rivaroxaban used in AF. 14 Therefore, the high levels of anticoagulant effect when added to DAPT in ACS patients may not provide benefits due to the high risk of bleeding complications.
Given the survival benefit presented in the ATLAS ACS 2 trial, the 2.5 mg BID regimen of rivaroxaban with aspirin alone or with DAPT obtained regulatory approval from the European Medicines Agency (EMA) for secondary prevention in ACS patients with elevated cardiac biomarkers. 50 However, rivaroxaban has not been approved by the Food and Drug Administration (FDA) for the ACS indication due to concerns regarding missing data in the pivotal trial. The addition of low-dose rivaroxaban (2.5 mg BID for one year) is now considered within the European Society of Cardiology guidelines on NSTE-ACS and STEMI.11,12 In particular, in NSTEMI patients without history of prior stroke/TIA and at high ischemic risk as well as low bleeding risk receiving aspirin and clopidogrel, low-dose rivaroxaban (2.5 mg BID) may be considered after discontinuation of parenteral anticoagulation (Class IIb, level of evidence B); 12 in selected STEMI patients who receive aspirin and clopidogrel, low-dose rivaroxaban (2.5 mg BID) may be considered if the patient is at low bleeding risk (Class IIb, level of evidence B). 11
The observations from the ATLAS ACS 2 trial have led to questions on how to enhance the safety profile of rivaroxaban while maintaining efficacy. Recently, there has been emerging interest in exploring whether withdrawing aspirin from novel antithrombotic treatment regimens could be a potential approach to reaching this goal.51,52 The rationale behind this is that in the presence of other antithrombotic agents, aspirin may not provide further ischemic benefit, but simply enhance the risk of bleeding complications, in particular gastrointestinal. The bleeding risk of low-dose rivaroxaban (in addition to a P2Y12 receptor inhibitor) without aspirin was evaluated in the phase II, GEMINI-ACS-1 (A study to compare the safety of rivaroxaban versus acetylsalicylic acid in addition to either clopidogrel or ticagrelor therapy in participants with acute coronary syndrome-1) trial. 53 A total of 3037 ACS patients were randomly assigned to 2.5 mg BID rivaroxaban versus 100 mg aspirin (1:1 ratio) in addition to a P2Y12 receptor inhibitor in a double-blind fashion. The choice of the P2Y12 receptor inhibitor (ticagrelor or clopidogrel) was not randomized, and was left at the discretion of the investigator. TIMI non-CABG-related clinically significant bleeding, the primary endpoint of this trial, was similar in both groups at 12-month follow up (rivaroxaban: 5% versus aspirin: 5%, p = 0.584). The rates of TIMI major bleeding and ICH were very low and not significantly different between groups (TIMI major bleeding, rivaroxaban 1% versus aspirin 1%; ICH, rivaroxaban <1% versus aspirin 0%). The rate of the primary endpoint was similar between the two groups both in the ticagrelor stratum (rivaroxaban 7% versus aspirin 6%) and in the clopidogrel stratum (rivaroxaban 3% versus aspirin 3%). There was a significant increase in bleeding with ticagrelor compared to clopidogrel (p = 0.0006). The exploratory ischemic endpoint (CV death, MI, stroke or definite stent thrombosis) was also similar between groups (rivaroxaban 5% versus aspirin 5%, p = 0.73). Overall, the findings from the GEMINI-ACS-1 trial suggest that the use of low-dose rivaroxaban with ticagrelor without aspirin was associated with an acceptable safety profile compared with DAPT with aspirin and ticagrelor.
Darexaban (YM150)
The tolerability and safety of darexaban (YM150), another direct FXa inhibitor, in ACS patients was tested in the phase II, RUBY-1 [A randomized, double-blind, placebo controlled trial of the safety and tolerability of the novel oral Factor Xa inhibitor darexaban (YM150) following ACS] trial. 54 In this trial, a total of 1279 patients with recent NSTEMI or STEMI were enrolled and randomly assigned to different doses of darexaban (5 mg BID, 10 mg QD, 15 mg BID, 30 mg QD, 30 mg BID, 60 mg QD) or placebo. There were higher rates of major (by ISTH definition) and clinically relevant non-major bleeding in a dose-dependent manner with all dosing regimens of darexaban compared to placebo without any improvement in efficacy endpoints (the composite of death, MI, stroke, systemic thromboembolism and severe recurrent ischemia). After the RUBY-1 trial, the development of darexaban for ACS patients was halted.
Letaxaban (TAK-442)
The safety and tolerability of letaxaban were tested in the AXIOM ACS (Safety and efficacy of TAK-442 in subjects with acute coronary syndromes) trial. 55 The AXIOM ACS trial was a dose-ranging, phase II trial that enrolled 2753 ACS patients. This trial explored a wide range of letaxaban doses (from 10 mg BID to 120 mg BID). The rate of TIMI major bleeding, the primary endpoint of this study, was not significantly different between groups (0.9% in letaxaban versus 0.5% in placebo, p = 0.47). However, the composite rate of TIMI major and minor bleeding was more frequent with letaxaban (2.1% versus 0.9%, p = 0.025). The efficacy endpoint was similar between letaxaban and placebo. There has not been further testing for ACS patients with letaxaban.
Edoxaban
Edoxaban is a direct oral Factor Xa inhibitor used for the prevention of ischemic stroke in AF patients as well as for the prevention/treatment of VTE. 39 However, there have not been any studies assessing edoxaban in ACS patients.
Clinical trial update
Large randomized trials have either been recently completed or are completing enrollment which are assessing the safety and efficacy of oral anticoagulant therapy, in particular rivaroxaban, in patients with atherosclerotic disease manifestations, albeit not selectively in patients with an ACS. The COMPASS trial [Cardiovascular outcomes for people using anticoagulation strategies trial (ClinicalTrials.gov identifier: NCT01776424)] was designed to evaluate the efficacy and safety of low-dose rivaroxaban plus aspirin compared to aspirin monotherapy for the prevention of ischemic events in patients with CAD or peripheral artery disease (PAD). Patients were randomly assigned to one of three groups (rivaroxaban 2.5 mg BID plus aspirin 100 mg; rivaroxaban 5 mg BID alone; or aspirin 100 mg alone). The trial was stopped one year ahead of its scheduled completion date after enrollment of 27,402 patients because rivaroxaban was shown to meet its efficacy endpoint. In particular, rivaroxaban plus aspirin showed better cardiovascular outcomes, including reduced mortality, than with aspirin alone, with consistent findings in the CAD and PAD populations. Although the combination group showed more major bleeding than aspirin alone, there was no significant difference in rate of ICH or fatal bleeding between these two groups. Rivaroxaban monotherapy (5 mg BID) did not result in better cardiovascular outcomes than aspirin alone and showed more major bleeding events. 56 It is important to note that only 62% of patients enrolled in COMPASS had a prior ACS, and the mean time from this event to randomization was 7.1 years. Therefore, the observations from the COMPASS trial suggest that there may be a role for adjunctive use of a very low dose of rivaroxaban for secondary prevention of ischemic events in the patients with stable atherosclerotic disease, and should not be considered as a post-ACS management strategy until further information is available. The VOYAGER PAD trial [Efficacy and safety of rivaroxaban in reducing the risk of major thrombotic vascular events in subjects with symptomatic peripheral artery disease undergoing peripheral revascularization procedures of the lower extremities trial (ClinicalTrials.gov identifier: NCT02504216)] is investigating the role of rivaroxaban in addition to the standard care of PAD. This ongoing trial will enroll 6500 participants undergoing successful revascularization procedure for symptomatic PAD, and randomized to rivaroxaban 2.5 mg BID or placebo. The use of clopidogrel is kept to the minimum necessary in accordance with international practice guidelines. The primary endpoint is a first occurrence of MI, ischemic stroke, CV death, acute limb ischemia and major amputation for 2 years; results are anticipated in 2019.
Future perspectives
Despite the use of standard of care DAPT with aspirin and a P2Y12 receptor antagonist, the risk of ischemic recurrences in ACS patients remains high. The persistence of thrombin generation after an ACS event may contribute to these observations, prompting investigators to reappraise the role of long-term oral anticoagulant therapy in these patients. Indeed, the introduction of the NOACs, which have a more favorable safety profile and ease of use compared with VKA, have stimulated interest in this field of investigation. A multitude of NOACs have been tested in the context of ACS settings. However, only rivaroxaban successfully completed phase III clinical investigation meeting its primary endpoint and has received approval for clinical use in most parts of the world (not in the United States) for patients with ACS. However, despite the survival benefit observed with rivaroxaban when used at a 2.5 mg BID regimen, in addition to standard of care therapy including DAPT, the uptake of the drug for the ACS indication has been very limited. Indeed, the increased bleeding risk as well as the need to consider a third antithrombotic agent contribute to the lack of enthusiasm of physicians and patients embracing this approach in clinical practice. Encouraging data from recent trial results suggest that withdrawal of aspirin therapy may be a safe approach in patients treated with low-dose rivaroxaban plus ticagrelor. These investigations have been prompted based on studies that have suggested that there is limited antithrombotic efficacy associated with aspirin therapy in the presence of potent P2Y12 blockade, which has been associated with modulation of other key platelet signaling pathways, including thromboxane generation.57–59 Indeed larger investigations are warranted to support the efficacy of this strategy. Moreover, a better understanding is needed to define the interplay between NOACs and antiplatelet agents. In fact, to date there is very limited data on this topic and it is also unclear how NOACs with different targets (anti-FII versus anti-FX) impact the effects of different classes of antiplatelet agents (COX-1 versus P2Y12 inhibitors).60,61 These studies will indeed provide important insights on the safety and efficacy findings from clinical trial data associated with their combined use. Ultimately, how to bridge from acute to long-term care with oral anticoagulant therapy among patients who experienced an ACS is also needed. Indeed, the results from patients with a more recent ACS who were enrolled in the COMPASS trial will provide further insights on this topic.
Conclusions
Over recent years there has been a reappraisal of the use of oral anticoagulant therapy for secondary prevention of ischemic recurrences in ACS patients. This has been indeed facilitated by the introduction of the NOACs, which have a favorable safety profile and ease of use compared with VKAs, which were tested in the same context a few decades ago, leading to disappointing outcomes due to the high risk of bleeding. Of the clinically available NOACs, only rivaroxaban when used at a 2.5 mg BID regimen, which is substantially lower than that used for stroke prevention in AF patients, has shown to be associated with an ischemic benefit, including a reduction in mortality and has received regulatory approval for clinical use in most countries across the globe. However, risks of bleeding complications still remain high when this regimen is added to standard DAPT, underscoring the need to define antithrombotic treatment regimens that maintain efficacy but minimize bleeding complications. A current wave of investigations is evaluating whether withdrawing aspirin therapy may represent a potential option to reach this goal. Indeed, a number of ongoing pharmacodynamic and clinical investigations will provide more insights on the role of using long-term oral anticoagulant therapy for secondary prevention in patients with cardiovascular disease manifestations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
Dr. Angiolillo reports receiving payments as an individual for: (a) consulting fee or honorarium from Amgen, Aralez, AstraZeneca, Bayer, Biosensors, Bristol-Myers Squibb, Chiesi, Daiichi-Sankyo, Eli Lilly, Janssen, Merck, PLx Pharma, Pfizer, Sanofi, and The Medicines Company; (b) participation in review activities from CeloNova and St. Jude Medical. Institutional payments for grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi-Sankyo, Eisai, Eli-Lilly, Gilead, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, Osprey Medical, and Renal Guard Solutions; in addition, Dr. Angiolillo is recipient of a funding from the Scott R. MacKenzie Foundation and the NIH/NCATS Clinical and Translational Science Award to the University of Florida UL1 TR000064 and NIH/NHGRI U01 HG007269, outside the submitted work.