
Abstract
Hepatic veno-occlusive disease (VOD), also known as sinusoidal obstruction syndrome, is a potentially life-threatening complication of chemotherapeutic conditioning used in preparation for hematopoietic stem-cell transplantation (SCT). VOD may occur in up to 62% of patients undergoing SCT, with onset generally within the first month after SCT. In severe cases, 100-day mortality is in excess of 80%. Current management consists of best supportive care, with no agents to date approved for treatment in the USA or the EU. Defibrotide, a polydisperse oligonucleotide, has been shown in phase II and III trials to improve complete response and survival in patients undergoing SCT with severe VOD. This article reviews our current understanding of VOD, and examines recent clinical findings on defibrotide for the treatment and prophylaxis of VOD.
Introduction
Hepatic veno-occlusive disease (VOD) is a serious condition that usually arises within the first 30 days after hematopoietic stem-cell transplantation (SCT), and is believed to be the result of endothelial cell damage and hepatocellular injury from high-dose conditioning regimens prior to SCT [Bearman, 1995; Kumar et al. 2003]. VOD is characterized by rapid weight gain, painful hepatomegaly, hyperbilirubinemia/jaundice, and ascites/fluid retention, without other identifiable causes for liver disease; VOD is fatal in 20–50% of patients [Bearman, 1995; Kumar et al. 2003]. Clinical criteria for the diagnosis of VOD have been developed; Seattle criteria stipulate that at least two or more clinical features including jaundice, painful hepatomegaly or ascites, and/or unexplained weight gain must be evident within 30 days of transplantation [Bearman, 1995; McDonald et al. 1984]; Baltimore criteria specify an elevated bilirubin level of at least 2.0 mg/dl and two or more of the following characteristics: hepatomegaly, ascites, or at least 5% weight gain by day 21 post-SCT [Bearman, 1995; Jones et al. 1987]. Although not included in the formal diagnostic criteria in the past, it has also been found that rapid and unexpected elevations in the blood levels of specific anti-graft-versus- host-disease (GvHD) drugs (such as sirolimus and tacrolimus) in association with a rise in creatinine as well as fluid avidity and weight gain (but prior to liver function abnormalities emerging) can be a valuable hint that VOD and sinusoidal obstruction may be evolving [Cutler et al. 2010].
In this article, we review the incidence and pathogenesis of VOD, and evaluate approaches to the treatment of the disease. In particular, we focus on the safety and efficacy of the investigational drug, defibrotide, a polydisperse mixture of porcine-derived single-stranded oligonucleotides [Bianchi et al. 1993], and its potential for the treatment and prophylaxis of VOD in patients undergoing SCT.
Prevalence of veno-occlusive disease
A recent analysis of retrospective data, prospective cohort studies and clinical trials published between 1979 and 2007 detailed the prevalence and severity of VOD [Coppell et al. 2010]. This comprehensive analysis found that VOD was reported in up to 62% (with a mean of 13.7%) of patients undergoing SCT following myeloablative conditioning. Prevalence varied according to the conditioning regimen, the type of transplantation, and the diagnostic criteria used [Coppell et al. 2010] (Table 1). Similarly, in an important recent retrospective study of 845 patients who received an allogeneic SCT over the past 24 years, the cumulative incidence of VOD was found to be 13.8% using Seattle criteria and 8.8% using Baltimore criteria [Carreras et al. 2011]. The incidence of VOD in children undergoing SCT also varies, ranging from 11% to 20% [Cesaro et al. 2005; Lee et al. 2010]. VOD ranges from mild, reversible disease to severe illness with multiple organ failure (MOF) and death [Kumar et al. 2003]. In the Carreras retrospective study, approximately two-thirds of patients had mild or moderate VOD and one-third had severe VOD according to Seattle criteria; this was closer to 50% when Baltimore criteria were used [Carreras et al. 2011]. In the Coppell analysis, up to 77% of all cases of VOD proved severe, with severe disease in turn associated with a mortality rate in excess of 80% [Coppell et al. 2010]. For severe VOD, the death rate in a large single-centre study (from Seattle) was reported as 98% [McDonald et al. 1993]. Many alternative conditions that adversely affect the liver after transplantation can mimic the signs and symptoms of VOD; diagnosis of VOD, especially in its early stages, is therefore a clinical challenge [Kumar et al. 2003]. In addition to the emergence of MOF, the risk for developing severe VOD can also be estimated using the Bearman prognostic model, which is based on height of bilirubin elevation, percentage weight gain, and time from transplant (up to day +16), although this model has only been validated for certain regimens [including cyclophosophamide (CY) plus total body irradiation (TBI), busulfan (BU) plus CY, and CY, carmustine plus etoposide] [Bearman et al. 1993a].
Variables that can influence incidence of veno-occlusive disease.

BU, busulfan; CY, cyclophosphamide; SCT, stem-cell transplantation; VOD, veno-occlusive disease.
Pathogenesis of veno-occlusive disease
Sinusoidal endothelial cell and hepatocyte injury, usually within zone 3 of the hepatic acinus, triggered by intensive chemotherapy conditioning are thought to be pivotal in the development of VOD [Coppell et al. 2010; Kumar et al. 2003]. Endothelial damage and hepatocellular necrosis with subendothelial edema and microthrombosis are seen (reviewed in [Richardson and Guinan, 1999; Carreras, 2000]). Fibrin-related aggregates and cellular debris occlude the small pores that perforate the endothelial lining, causing obstruction of the venous outflow. This results in intrahepatic portal hypertension, which is responsible for the main clinical manifestations of VOD (reviewed in [Carreras, 2000]). As a consequence of the endothelial cell damage, sinusoidal obstruction is often prominent on microscopy, leading to the alternative terminology sinusoidal obstruction syndrome [Kumar et al. 2003]. Cytokines, such as interleukin-1, interleukin-2 and tumor necrosis factor α, may be elevated due to tissue injury caused by both chemotherapy and allogeneic injury, with their procoagulant effects on endothelial cell surfaces further contributing to the pathogenesis of VOD, with endothelial damage leading to further cytokine release and serine protease activation (e.g. tissue factor) [Baars et al. 1992; Carreras, 2000; Holler et al. 1990; Nawroth et al. 1986]. Conditioning-related injury may be potentiated by agents used for GvHD prophylaxis, for example sirolimus (or a combination of sirolimus and tacrolimus), because sirolimus may accelerate the senescence of hepatic endothelial cells after conditioning-related injury [Cutler et al. 2010]. Sirolimus may also reduce endothelial growth factor levels, hindering the healing process [Cutler et al. 2010]. Elevated levels of several markers of endothelial injury have been described, including a key inhibitor of fibrinolysis, plasminogen activator inhibitor type-1 (PAI-1), and plasma thrombomodulin [Nurnberger et al. 1998; Salat et al. 1994]. PAI-1 inhibits fibrinolysis, may contribute to microthrombosis and can exacerbate subsequent organ failure [Reilly et al. 1994]; as a result, PAI-1 has become recognized as both a diagnostic and prognostic biomarker for VOD [Lee et al. 2002]. PAI-1 production is stimulated by transforming growth factor β (TGF-β); TGF-β released from activated platelets further contributes to hemostatic imbalance at the level of the sinusoidal endothelial surface in patients with VOD via an increase in endothelial cell PAI-1 production [Pihusch et al. 2005]. TGF-β has been implicated in the pathogenesis of fibrosis [Czaja et al. 1989], and elevated levels of TGF-β strongly correlate with an increased risk of the disease following SCT [Anscher et al. 1993]. Also a reduction in hepatic nitric oxide (NO) levels has been shown to contribute to the development of VOD via disruption in sinusoidal integrity and subsequent disturbance of sinusoidal perfusion [DeLeve et al. 2003]. Conversely, NO has been found to play a role in reducing hepatocyte damage and increasing hepatic microcirculation in rats, suggesting a potential role for NO in the prevention of ischemia-reperfusion injuries [Kuroki et al. 2004].
Risk factors for veno-occlusive disease
A number of risk factors, both pre and post SCT, can predispose patients to developing VOD. Pretransplant risk factors include patient-related factors, such as older patient age, female gender, pre-existent liver injury (especially cirrhosis) and advanced malignancy (reviewed in [Ho et al. 2008]). Allogeneic SCT is associated with a markedly increased risk of development of VOD compared with autologous SCT (Table 1); this could be due to the use of cyclosporin or methotrexate for the prophylaxis of GvHD, or may indicate an allogeneic immunological element in the development of VOD [Carreras, 2000] via cytokine dysfunction and inflammation [Richardson and Guinan, 1999].
As mentioned above, specific transplant conditioning regimens, including CY followed by TBI [McDonald et al. 2003] and BU followed by CY [McCune et al. 2007], are associated with the development of VOD, although inter-patient variability can confound correlations [McCune et al. 2007].
In an in vitro study, BU has been shown to deplete hepatic glutathione and, at high concentrations, induce oxidative stress resulting in BU toxicity [DeLeve and Wang, 2000]. Another in vitro study revealed that sinusoidal cells are highly sensitive to CY metabolites; CY metabolites deplete glutathione by more than 95% and profound depletion of glutathione precedes the onset of toxicity [DeLeve, 1996]. Patients undergoing SCT with a short interval from administration of gemtuzumab ozogamicin, a monoclonal antibody against CD33 used in the treatment of acute myeloid leukemia (AML), have a significantly increased risk of VOD development [Wadleigh et al. 2003], possibly due to targeting of CD33+ cells in the sinusoids of the liver, activation of stellate cells, damage to sinusoidal endothelial cells, sinusoidal vasoconstriction and ischemic hepatocyte necrosis [McDonald, 2002]. Prior abdominal irradiation has also been found to increase the risk of VOD compared with patients with no prior abdominal irradiation (13% versus 5%, respectively; p = 0.009) [Carreras et al. 1998].
Approaches to the prevention of veno-occlusive disease
Modification of conditioning and GvHD prophylaxis regimens may reduce the risk of developing VOD. In patients conditioned with BU plus CY, intravenous BU has been found to significantly decrease the incidence of VOD after allogeneic SCT compared with orally administered BU (Table 1) [Lee et al. 2005]. Since CY metabolites are implicated as important contributors to endothelial injury in VOD, substitution of high-dose CY in the conditioning regimen may also ameliorate VOD risk. Indeed, a recent retrospective study comparing oral BU plus CY with targeted intravenous BU plus fludarabine (BU/Flu) as conditioning therapy in patients with AML demonstrated that high-dose BU/Flu was associated with less early toxicity, including VOD [Pidala et al. 2010]. In addition, caution has been advised against intensive treatment with gemtuzumab ozogamicin, especially within 3 months of SCT, to reduce the risk of VOD [McKoy et al. 2007; Ho et al. 2004]. Gemtuzumab ozogamicin (Mylotarg, Wyeth Pharmaceuticals, Philadelphia, PA, USA) was withdrawn from the US market in 2010 following reports of increased incidence of VOD in patients with AML in the absence of SCT as well as during the early post-transplantation period in patients who had been previously treated with the agent.
VOD risk may also be reduced by careful consideration of choice of GvHD prophylaxis in patients undergoing allogeneic SCT. For example, use of ex vivo T-cell depletion as GvHD prophylaxis has been associated with a lower risk of VOD [Moscardó et al. 2001]. Conversely, if pharmacological GvHD prophylaxis is employed, the combination of tacrolimus, sirolimus, and methotrexate is associated with a higher risk of VOD compared with tacrolimus and methotrextate [Cutler et al. 2008]. Further, the use of sirolimus as GvHD prophylaxis after high-dose BU/CY conditioning appears to further escalate the risk of severe VOD [Cutler et al. 2008].
Pharmacological prevention
As VOD is associated with aberrant fibrin deposition leading to sinusoidal and/or central vein occlusion, antithrombotic or fibrolytic agents have been investigated as prophylaxis for VOD. In an animal model, antithrombin III has been shown to exert anti-inflammatory properties [Okada et al. 1999] and potentially reverse procoagulant stress at the level of the endothelium [Richardson and Guinan, 2001; Richardson et al. 2010b]. However, antithrombin III as prophylaxis has not been found to decrease VOD incidence [Haussmann et al. 2006]. Separately, a recent study in 374 children undergoing SCT suggests that prostaglandin E1 may have a protective effect against the development of VOD and may therefore be suitable for prophylaxis, although tolerability proved to be an issue [Lee et al. 2010]. Similarly, an earlier study found that significant toxicity occurred with prostaglandin E1 prophylaxis in patients undergoing SCT [Bearman et al. 1993b], and its ability to prevent severe VOD therefore remains unproven. Heparin prophylaxis, including combination therapy, has shown some potential to reduce the incidence of VOD [Batsis et al. 2006; Forrest et al. 2003; Lakshminarayanan et al. 2010]. Randomized clinical trials are required to clarify the otherwise mixed data observed to date. Ursodiol (ursodeoxycholic acid) as prophylaxis following allogeneic SCT has been associated with a reduced incidence of VOD [Essell et al. 1998; Ohashi et al. 2000]. However, a multicenter randomized trial from the Nordic Bone Marrow Transplantation Group comparing patients with or without ursodiol treatment prior to and after allogeneic SCT did not show any benefit in terms of VOD, although improved overall survival and reduced hepatic complications were observed in the ursodiol arm [Ruutu et al. 2002].
Management of veno-occlusive disease
Current standard management of VOD focuses on best supportive care, which includes avoidance of hepatorenal toxic agents, management of fluid overload with diuresis, paracentesis for large volume ascites, ventilator support and hemodialysis as clinically indicated [DeLeve et al. 2009]. In rare cases, liver transplantation may be considered [DeLeve et al. 2009].
There are currently no standard approved pharmacological agents for the treatment of VOD in the USA or the EU. Systemic anticoagulants or thrombolytics such as tissue plasminogen activator (tPA) have been investigated as treatment options for established VOD, but they have been associated with significant bleeding complications, including fatal events, thus limiting their utility and with no survival benefit observed (reviewed in [Ho et al. 2008]).
Defibrotide
Defibrotide is a promising candidate for the treatment of VOD due to its pleiotropic effects at the endothelial surface, and the relatively low risk of significant systemic bleeding associated with its use [Richardson and Guinan, 1999, 2001]; exciting new data on defibrotide are now available in this setting.
Mechanisms of action
Defibrotide is a polydisperse mixture of porcine-derived single-stranded oligonucleotides, which was initially identified as an adenosine receptor agonist [Bianchi et al. 1993]. However, subsequent preclinical studies have shown defibrotide to have multiple actions in the micro- and macrovasculature, and have confirmed defibrotide as an attractive candidate agent for the treatment of VOD [Echart et al. 2009; Falanga et al. 2003].
Studies have revealed that defibrotide confers antithrombotic properties by increasing levels of the fibrinolytic protein plasmin, through increase in tPA, which activates plasminogen to plasmin [Falanga et al. 2003], by increasing activity of plasmin itself [Echart et al. 2009], and by reducing PAI-1 levels [Falanga et al. 2003]. In addition, defibrotide reduces the amount of a key endothelial cell surface procoagulant tissue factor (TF), through blocking TF deposition in the extracellular matrix [Palomo et al. 2011] and stimulating release of TF pathway inhibitor [Benimetskaya et al. 2008] as well as other vascular mediators, such as NO [Richardson and Guinan, 2001]. Thus, defibrotide may limit the organ dysfunction and thrombotic microangiopathies associated with fibrin deposition [Falanga et al. 2003]. In addition, defibrotide has been shown to protect endothelial cells against apoptosis induced by certain cytotoxic drugs [Eissner et al. 2002] and to prevent allogeneic responses of CD8 cells against endothelial targets.
Defibrotide has also been shown to confer anti-inflammatory properties. Preclinical studies have found that the proinflammatory p38 mitogen-activated protein kinase and Akt cell signaling pathways are upregulated in endothelial cells that have been incubated in sera from patients after autologous SCT [Palomo et al. 2011]. These signaling pathways were inactivated by defibrotide [Palomo et al. 2011]. Moreover, the same group observed that elevated levels of intercellular adhesion molecule-1 (ICAM-1), which are associated with blood vessel inflammation [Lawson and Wolf, 2009], were blocked by defibrotide [Palomo et al. 2011]. Previous exposure and continuous incubation of cultured endothelial cells with defibrotide prevented the signs of activation and damage induced by sera from patients following autologous SCT, indicating that defibrotide has protective anti-inflammatory and antithrombotic effects in this setting [Palomo et al. 2011].
Furthermore, defibrotide may provide a stimulus to the sinusoidal endothelium of a damaged liver and aid in revascularization. In vitro, defibrotide was found to promote endothelial cell proliferation and angiogenesis, in addition to stimulating tubular morphogenesis [Benimetskaya et al. 2008].
Defibrotide may also have a protective effect against acute GvHD. Elevated expression of the heparanase gene was identified as a risk factor for acute GvHD following SCT [Ostrovsky et al. 2010], and defibrotide has been shown to suppress heparanase expression [Mitsiades et al. 2009]. Activation of adenosine receptors has been found to inhibit T-cell function with the potential for prevention and treatment of acute GvHD [Lappas et al. 2010; Saldanha-Araujo et al. 2011].
Clinical assessment of defibrotide
Defibrotide does not interfere with chemotherapeutics in vitro, and it has been shown to reduce resistance to chemotherapy in vitro and in animal models, although defibrotide has no antitumor properties of its own [Mitsiades et al. 2009]. Defibrotide is well tolerated and can be administered intravenously, intramuscularly, or orally (reviewed by [Palmer and Goa, 1993]).
The first study to evaluate defibrotide for the treatment of severe VOD was performed in the USA and analyzed 19 patients with severe VOD after SCT (defined as bilirubin >2 mg/dl, and two or more of the following clinical features: hepatomegaly and right upper quadrant pain, ascites, or >5% weight gain above admission weight), with patients treated on a compassionate-use basis [Richardson et al. 1998]. Resolution of VOD (<2 mg/dl bilirubin and improvement in other symptoms) was observed in eight patients (42%), six of whom survived for longer than 100 days, and no significant bleeding was seen. Although this was a retrospective study and of limited sample size, the encouraging findings prompted a European multicenter compassionate-use study, which assessed defibrotide in 40 patients with VOD post SCT (according to either the Baltimore or Seattle criteria) [Chopra et al. 2000]. This study reported a complete response (CR) in 22 patients (55%) and 17 patients (43%) were still alive after 100 days [Chopra et al. 2000], again with no significant toxicity described. However, the data were based on a retrospective review of eligibility and outcome forms at individual treating centers. Thus, these results must be interpreted with some caution.
The encouraging findings of the initial US experience led to the enrollment of an additional 69 patients with severe VOD into a larger multi-institutional study, to provide a total of 88 patients as part of an emergency use dose escalation protocol. The study reported CR in 36% of patients, with a 100-day survival rate of 35% [Richardson et al. 2002]. A decrease in PAI-1 levels during defibrotide treatment was associated with better outcome. In line with the VOD risk factors discussed above, patients who had received autologous SCT responded better than those who had received allogeneic SCT, and improved survival was observed in patients who had not previously received BU-based conditioning compared with those who had [Richardson et al. 2002]. Since this study, several case series have reported similar CR rates and improved survival with defibrotide in patients with severe VOD [Bairey et al. 2002; Palladino et al. 2008; Shah et al. 2009].
In a recent, rigorously conducted, prospective phase II, multicenter, randomized, dose-finding trial, adult and pediatric patients with severe VOD were randomized to receive one of two doses of defibrotide (25 mg/kg/day or 40 mg/kg/day) [Richardson et al. 2010b]. Patients were eligible if they had at least a 30% chance of developing severe VOD by the Bearman prognostic model [Bearman et al. 1993a], or had MOF. Overall, 46% of 141 evaluable patients achieved CR, and the 100-day survival rate was 42% in 149 treated patients, with no significant difference in response between the two dose regimens. Defibrotide was generally well tolerated, with treatment-related adverse events reported in only 8% of patients, although a trend toward more toxicity was seen with the 40 mg/kg/day defibrotide dose compared with the 25 mg/kg/day dose, particularly among the pediatric patients. Based on these results, 25 mg/kg/day was the dose selected for further study.
A pivotal phase III, historically-controlled clinical trial of defibrotide in patients with severe VOD has been recently completed [Richardson et al. 2009]. The trial comprised 102 patients with VOD (according to the Baltimore criteria) within 21 days of SCT and with MOF (renal and/or lung dysfunction) by day 28 post transplant. Patients received intravenous defibrotide 6.25 mg/kg every 6 h (total 25 mg/kg/day) for at least 21 days. Due to the life-threatening nature of severe VOD and the absence of any other effective treatment as a comparator, the placebo arm of this phase III study was composed of a matched historical control (HC). Medical charts at each center were reviewed by an independent Medical Review Committee (MRC) to provide 32 suitable HC patients. The MRC was blinded to outcome data from both the defibrotide and HC arms. The primary endpoint of this trial was CR (bilirubin <2 mg/dl and resolution of MOF) by 100 days post SCT; the secondary endpoint was 100-day mortality. The 100-day CR rate was significantly higher in the defibrotide arm compared with the HC arm (24% versus 9%, respectively; adjusted p = 0.015). There was a substantial decrease in the 100-day mortality rate with defibrotide compared with HC (62% versus 75%, respectively; adjusted p = 0.051). A strong correlation was observed between CR and survival for both patients receiving defibrotide (p < 0.0001) and those in the HC group (p = 0.0016). Subgroup analysis revealed that in patients receiving defibrotide compared with those in the HC group, autologous transplantation, age 16 years and younger, and dialysis independence were associated with a significantly higher CR (p =0.005, 0.04 and p = 0.027, respectively). A similar number of patients in both groups experienced hemorrhage: 65% of patients receiving defibrotide and 69% of patients in the HC group, with treatment discontinued in 18% of patients who received defibrotide due to possible drug-related adverse events. Whilst these results are encouraging, it should be noted that this phase lll study was not a prospectively randomized study, and matched HCs were used as the comparator. Although using a HC methodology is not ideal, the absence of any other effective treatment as a comparator in patients with severe disease limits the options available for ethically evaluating the efficacy of defibrotide, and so this approach constituted the most reasonable strategy in this setting.
A meta-analysis combining results from the above phase II and III trials has since been conducted [Richardson et al. 2010c]. Of the total 133 patients treated with defibrotide 25 mg/kg/day, 29% achieved a CR by day 100 compared with 9% in the HC group (p = 0.0021). The mortality rate at day 100 was 60% in the defibrotide cohort versus 75% in the HC cohort (p = 0.0408). Hemorrhage and GvHD incidence were lower in patients treated with defibrotide compared with those in the HC group (61% versus 72%, respectively, for hemorrhage; 6% versus 25% for GvHD). The observations of reduced GvHD seen in both treatment and prophylactic studies of defibrotide are intriguing and imply that endothelial injury is also important in the development of acute GvHD, so warranting further evaluation [Cooke et al. 2008].
Due to the recognition of VOD with MOF as a life-threatening condition, defibrotide became available in the USA through an investigational new drug (IND) treatment protocol in December 2007. An interim analysis of 104 patients enrolled on this protocol from multiple centers found that 36 patients (35%) achieved a CR at day 100 post transplant, and the 100-day overall survival was 39% [Richardson et al. 2010a]. From this protocol, 69 patients met the eligibility criteria of the pivotal phase III trial, and when compared with HC counterparts in the phase lll trial, they achieved a significantly higher CR rate (p = 0.0007). Although comparison with matched HCs has limitations, as discussed previously, this is a promising finding and may reflect the fact that this population were marginally less sick in terms of degree of MOF, an observation also seen in other studies of defibrotide therapy where earlier intervention has been associated with better outcome [Corbacioglu et al. 2004; Richardson et al. 2010b]; Table 2 summarizes comparable data from these larger pivotal studies.
Summary of clinical response and overall survival with defibrotide for the treatment of severe hepatic veno-occlusive disease.
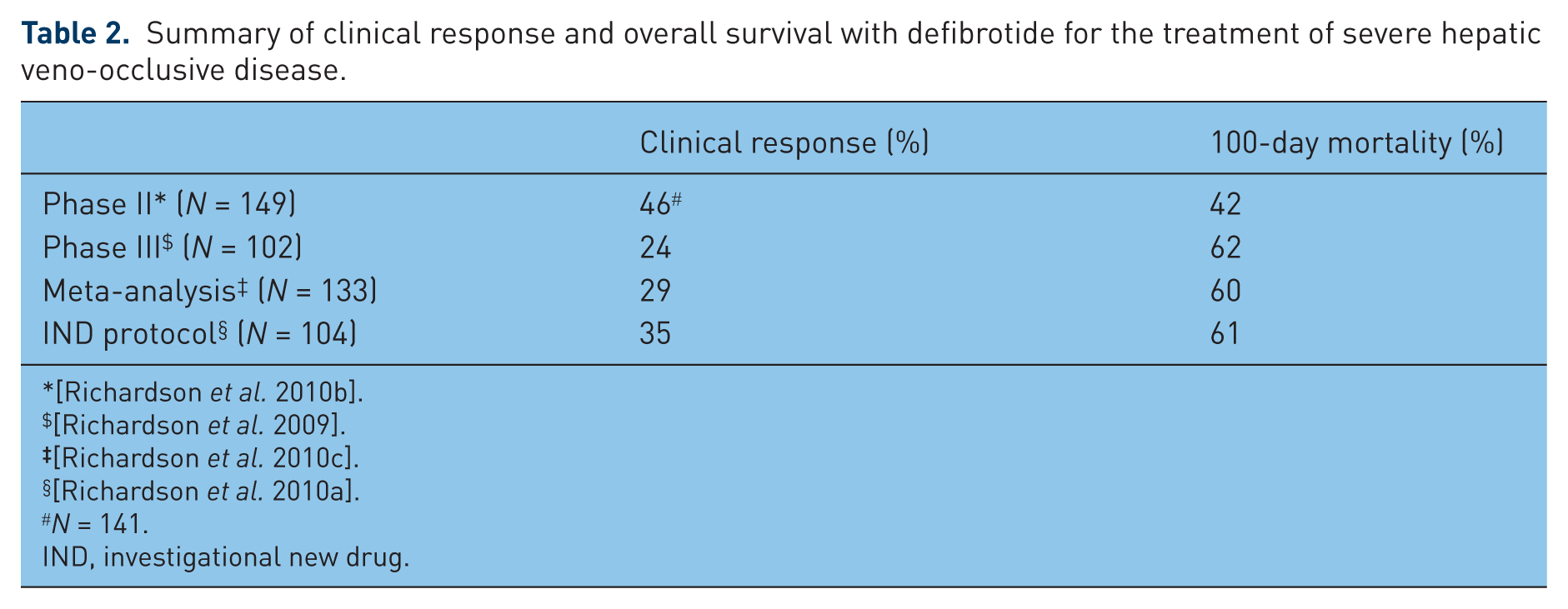
N = 141.
IND, investigational new drug.
In a recent retrospective analysis of 845 consecutive cases of allogeneic SCT performed in a single center during the last 24 years, the mortality rate due to VOD was 36% before 1997 compared with 14% since 1997, the only relevant change in the management of these patients being the introduction of defibrotide [Carreras et al. 2011]. Whilst other changes in the management of patients with VOD have also been associated with improved outcomes, and these include the increasing use of reduced-intensity conditioning regimens [Ramasamy et al. 2006], use of high-resolution human leukocyte antigen typing [Petersdorf, 2004], improvement of patient support measures, plus the increasing use of peripheral blood stem cells, this observation was considered compelling [Carreras et al. 2011]. Switching administration from oral to intravenous BU and using targeted dose-adjusted BU also decreases the incidence of VOD and may improve outcomes for patients with VOD, although the impact of this change on survival has been at best very modest in patients with established disease [Clopes et al. 2006; Kashyap et al. 2002].
Defibrotide as prophylaxis
The promising results observed in the treatment trials described above provided a good rationale for further investigation of defibrotide as prophylaxis against VOD following SCT. Although no prospective randomized studies in adult SCT have been published to date, there have been a number of prospective historically controlled trials suggesting that defibrotide is safe and effective in the setting of VOD prevention. One study compared 52 patients receiving defibrotide prophylaxis in addition to heparin with a HC group of 52 patients [Chalandon et al. 2004]. The investigators reported that no patients receiving defibrotide and heparin prophylaxis developed VOD compared with 19% of patients in the HC group (p = 0.001). There was also a trend towards improved 100-day survival with defibrotide and heparin compared with the HC group (p = 0.07). A more recent study evaluated 58 consecutive patients receiving protocol-directed defibrotide prophylaxis without concurrent heparin following allogeneic SCT [Dignan et al. 2007]. No patients developed VOD (according to the Baltimore criteria) and no patients died within 100 days of SCT, which was significantly better than expected based upon prior incidence rates at that center (namely, the Royal Marsden Hospital, UK).
The role of defibrotide to prevent VOD in children has been recently evaluated in a prospective multicenter phase II/III study [Corbacioglu et al. 2010]. This study randomized 360 children (<18 years) undergoing myeloablative SCT (69% allogeneic, 31% autologous) to either receive prophylactic defibrotide from conditioning to 30 days post SCT or no prophylaxis (control group). In the intent-to-treat analysis (n = 356) 12% of patients in the defibrotide arm versus 20% in the control group developed VOD by day 30 after SCT (p = 0.051). In the per protocol analysis (n = 360) VOD incidence was 11% in the defibrotide arm versus 20% in the control group (p = 0.023). The composite score for morbidity and mortality was significantly lower with defibrotide compared with the control (p = 0.034), and renal failure was observed in 1% of patients in the defibrotide arm versus 6% in the control group (p = 0.017). Excluding patients with autologous SCT, the incidence (45% versus 63%; p = 0.004) and severity (p = 0.003) of acute GvHD by day 100 was significantly reduced in the patients in the defibrotide arm compared with the control arm, suggesting that endothelial injury is also important in the pathogenesis of GvHD. Results from this prospective randomized trial confirm results from previously reported studies showing an advantage of defibrotide prophylaxis in children at a high risk of developing VOD [Cappelli et al. 2009; Corbacioglu et al. 2006; Qureshi et al. 2008; Versluys et al. 2004]. Importantly, defibrotide has been demonstrated to have favorable effects on thrombotic microangiopathy and renal failure [Bonomini et al. 1984, 1985; Vangelista et al. 1986]; preliminary studies in the SCT population have been favorable, with a positive effect on renal outcome also seen in this large pediatric prevention trial [Corbacioglu et al. 2010].
Future directions
Defibrotide is currently available via an ongoing treatment IND study in the USA and elsewhere via named patient use programmes, with regulatory approval for both treatment and prophylaxis of hepatic VOD being actively sought in the EU and the USA. Additional studies in prophylaxis are planned in adult populations and specific high-risk settings.
With improved understanding of the mechanism of action of defibrotide and pathogenesis of VOD, it may become possible to rationally design treatment and preventative strategies for VOD based on patient and transplant-specific profiles. As an example, subgroup analysis of the defibrotide phase III clinical study has already identified patients at increased risk of VOD, and those most likely to respond to defibrotide [Richardson et al. 2009], suggesting that a more personalized approach could further improve treatment and prevention outcomes. Though clinical trials with defibrotide have provided the most promising results as effective therapy for VOD to date, 100-day mortality from severe VOD remains unacceptably high at over 50%. Other therapies, such as antithrombin III, novel plasminogen activator inhibitors, N-acetyl cysteine and other novel antithrombotics may warrant further investigation in combination with defibrotide [Ho et al. 2008; Ringden et al. 2000]. If these agents complement defibrotide therapy without increasing the risk of bleeding or other toxicity, superior outcomes and survival may yet be realized.
Importantly, recent observations have found the outcome of early intervention with defibrotide to be superior to delayed treatment [Richardson et al. 2010a]. Elevations of von Willebrand factor, thrombomodulin, E-selectin, and soluble ICAM-1 before and early after allogeneic transplantation may be useful in predicting VOD in patients receiving sirolimus [Cutler et al. 2010] and could lead to pre-emptive trials based on biomarkers, leading to improved treatment strategies to reverse VOD pathophysiology earlier in specific high-risk groups [Platzbecker et al. 2009].
Footnotes
Acknowledgements
The authors acknowledge Kate Silverthorne and Abigail Marmont for their assistance in writing this manuscript, and the administrative assistance of Katie Redman and Michelle Maglio of the Dana-Farber Cancer Institute.
Funding
Funding for writing and administrative assistance was provided by Gentium S.p.A and the Rick Corman Multiple Myeloma Research Fund, respectively.
Conflict of interest statement
V.T. Ho, S. Giralt, S. Arai, S. Mineishi, J.H. Antin and N. Stavitzski have no conflicts of interest to declare. P.G. Richardson is on the advisory board for Gentium S.p.A. C. Cutler is consultant for Sigma Tau and has equity in Gentium S.p.A. D. Niederwieser is a consultant for the speakers bureau, Gentium S.p.A. E. Holler has received honoraria and research grants from Gentium S.p.A. E. Carreras and R. Soiffer have received honoraria from Gentium S.p.A.