
Abstract
Background
The role of perioperative chemotherapy in localized soft tissue sarcomas (STS) remains controversial, particularly in older adult patients and those with considerable comorbidities who may not tolerate anthracycline-based regimens. Although eribulin has demonstrated efficacy and safety in advanced STS, its use as a postoperative adjuvant treatment has not been well documented.
Objective
To evaluate the feasibility, safety, and clinical outcomes of postoperative adjuvant eribulin administration in patients with localized STS, with a focus on older adults and patients with comorbidities.
Methods
We conducted a single-institution retrospective study of a case series of patients with localized STS who had undergone surgical resection with curative-intent, followed by postoperative adjuvant eribulin administration. Data on patient characteristics, treatment administration, adverse events, and oncological outcomes were obtained from the medical records. Adverse events were graded based on the Common Terminology Criteria for Adverse Events.
Results
Eight patients, most of whom were older adults or had substantial comorbidities, were included in the study. Postoperative eribulin therapy was initiated in all patients. Hematological toxicities, including neutropenia and leukopenia, were relatively common, but manageable with dose modification and supportive care. Non-hematological toxicities, such as peripheral neuropathy and dysgeusia, were generally mild to moderate. No treatment-related deaths or clinically significant cardiac adverse events were observed. Six patients remained continuously disease-free during follow-up, whereas two died of the disease.
Conclusions
Postoperative adjuvant eribulin therapy was feasible and well-tolerated in a high-risk population of patients with localized STS. Although its efficacy cannot be determined from this small case series, its favorable safety profile suggests that eribulin may be a viable treatment option for patients who are poor candidates for anthracycline-based perioperative chemotherapy. Further studies are warranted to clarify its role in perioperative treatment strategies for STS.
Keywords
Introduction
Soft tissue sarcoma (STS) consists of a heterogeneous group of rare, malignant tumors, and complete surgical resection remains the keystone of curative treatment for localized disease. However, patients with high-risk pathological features continue to have high recurrence rates and disease-related mortality. 1
However, the role of perioperative chemotherapy in localized STS remains controversial. Several randomized trials and meta-analyses have suggested the modest benefit of anthracycline-based regimens in selected high-risk patients; however, consistent survival advantages have not been demonstrated.2,3 Accordingly, perioperative chemotherapy is not universally recommended in current clinical practice guidelines, and its use is often individualized. 4
Older patients and those with considerable comorbidities are major clinical challenges. Anthracycline-based chemotherapy, which is commonly used in the perioperative setting, may be poorly tolerated in this population due to concerns regarding cardio- and treatment-related toxicities. 5 Consequently, perioperative systemic treatment options for these patients are limited, and evidence guiding clinical decision-making is scarce.
Eribulin mesylate is a microtubule dynamics inhibitor that has demonstrated efficacy in advanced and metastatic STS, and is generally considered to have a favorable cardiac safety profile. 6 Despite its established role in the metastatic setting, no data are available regarding the use of eribulin as a perioperative or adjuvant treatment for localized STS.4,7
Therefore, we conducted a retrospective case series study to evaluate the feasibility, safety, and clinical outcomes of postoperative adjuvant eribulin administration in patients with localized STS, with a focus on older adult patients and those with notable comorbidities. Furthermore, we discuss the potential implications of our findings for the development of perioperative treatment strategies in high-risk patients with STS.
Materials and methods
Study design and patients
In this single-institution, retrospective case series study, we reviewed the data of consecutive patients with localized STS who had undergone surgical resection with curative-intent followed by postoperative adjuvant chemotherapy with eribulin at Tochigi Cancer Center, Tochigi, Japan, between July 2018 and June 2024.
Patients who had received eribulin exclusively as a postoperative adjuvant treatment were eligible for inclusion. Those who had received eribulin for unresectable or metastatic disease at treatment initiation were excluded from the study. The decision to administer eribulin was made by a multidisciplinary sarcoma team, and was primarily based on the patient’s age, comorbidities, and their anticipated tolerability of anthracycline-based chemotherapy. Written informed consent for treatment was obtained from all patients as part of routine clinical practice. This study is reported as a case series and conforms to the CARE (CAse REport) guidelines. 8 A completed CARE checklist has been provided as Supplemental file 1.
Data collection
Clinical data were retrospectively collected from the electronic medical records. The collected variables included age, sex, comorbidities, tumor location, histological subtype, surgical margin status, use of postoperative radiotherapy, number of eribulin treatment cycles, eribulin dosing schedule, treatment modifications, oncological outcomes, follow-up duration (months), and adverse events.
Adverse events were assessed throughout eribulin treatment and graded based on the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. 9
Treatment protocol
Eribulin was administered intravenously according to institutional practice. The standard dosing schedule consisted of two consecutive weekly administrations, followed by a 1-week rest period (2-on/1-off schedule). Dose reductions, treatment delays, and supportive care, including the use of granulocyte colony-stimulating factors, were permitted at the discretion of the treating physician, based on the patient’s condition and treatment-related toxicity.
All patients were administered eribulin after surgical resection. Postoperative radiotherapy was also administered when clinically indicated, based on the tumor location, surgical margin status, and multidisciplinary discussion.
Outcome measures
The primary endpoints of this study were the feasibility and safety of postoperative adjuvant eribulin administration. Feasibility was evaluated based on treatment initiation, continuation, dose modification, and discontinuation due to adverse events.
The secondary endpoints included descriptively assessed oncological outcomes. Disease-free status, recurrence, and disease-related death were recorded based on clinical and radiological follow-up.
Statistical analysis
Given the small sample size and descriptive nature of this case series, no formal statistical comparisons were performed. Continuous variables are presented as medians and ranges, and categorical variables as counts. No formal sample size calculation was performed due to the descriptive and exploratory nature of this retrospective case series.
Ethics approval
This study was conducted at Tochigi Cancer Center, Tochigi, Japan. This retrospective case series was conducted using anonymized clinical data obtained from routine clinical practice. According to the institutional policy of Tochigi Cancer Center, retrospective studies using fully anonymized data are covered by the institutional comprehensive consent system and do not require individual Institutional Review Board approval. All patient data were fully de-identified prior to analysis. This study was conducted in accordance with the Declaration of Helsinki (as revised in 2024).
Results
Patient characteristics
Patient demographics and clinical characteristics.

Abbreviations are RT: Radiation therapy, Fr: fraction.
Myxofibrosarcoma was the most common histological subtype (n = 4) followed by pleomorphic liposarcoma (n = 2). One patient each had myxoid and dedifferentiated liposarcoma. Tumors arose at various anatomical sites, including retroperitoneal and intraperitoneal locations. Details regarding the surgical margins and the use of postoperative radiotherapy are summarized in Table 1.
Eribulin administration and feasibility
Patient comorbidities and details of eribulin administration.
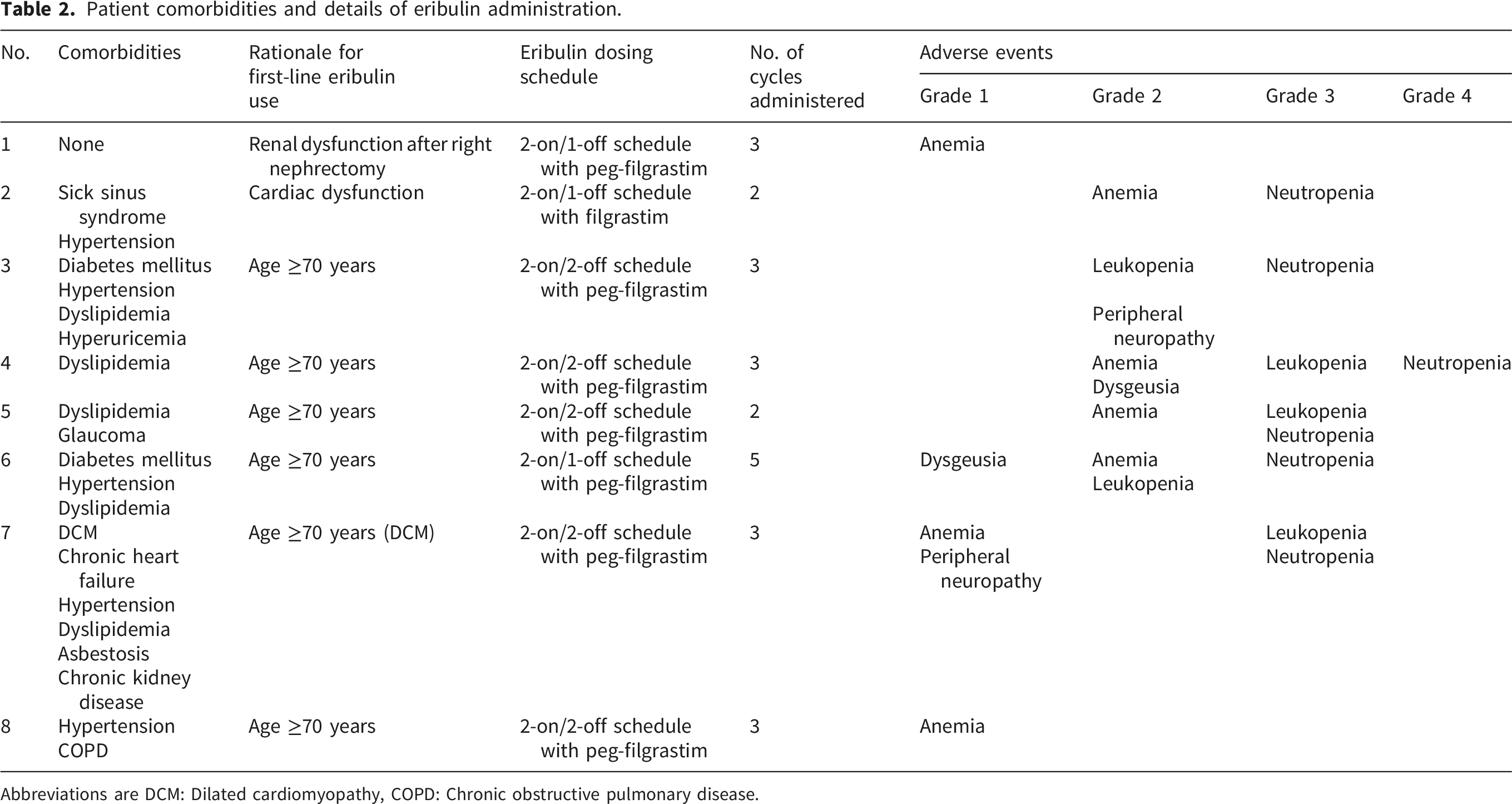
Abbreviations are DCM: Dilated cardiomyopathy, COPD: Chronic obstructive pulmonary disease.
Several patients required dose modifications or schedule adjustments during treatment, mainly because of hematological toxicity. Nevertheless, no patient permanently discontinued the eribulin treatment because of adverse events, and no treatment-related deaths were observed.
Safety and adverse events
The treatment-related adverse events are summarized in Table 2. Haematological toxicities, particularly neutropenia and leukopenia, were relatively common. These events were managed with dose adjustments, treatment delays, or supportive care, including the administration of granulocyte colony-stimulating factor, when appropriate.
The non-hematological toxicities included peripheral neuropathy and dysgeusia, which occurred in a subset of patients. These adverse events were generally mild to moderate in severity and were manageable with conservative measures. Importantly, no severe adverse cardiac events or clinically significant deterioration in cardiac function were observed during eribulin therapy.
Oncological outcomes and subsequent treatment
Eribulin treatment outcomes, subsequent treatment, and oncological outcomes.

Abbreviations are DOD: Died of disease, CDF: Continuous disease free.
The clinical courses of the two patients who experienced oncological events are summarized below. One patient with dedifferentiated liposarcoma of the retroperitoneum developed local recurrence 5 months after completion of eribulin therapy. The patient underwent two subsequent surgical resections; however, the third recurrence was deemed unresectable. Doxorubicin was administered at a reduced dose (80%), but treatment was discontinued after a single cycle due to grade 3 diarrhea. The patient was subsequently managed with best supportive care; however, she died of disease 23 months after eribulin therapy. Another patient with myxoid liposarcoma of the thigh developed multiple pulmonary metastases 67 months after eribulin therapy and was subsequently managed with best supportive care. The patient died of disease 73 months after eribulin therapy.
Discussion
In this retrospective study of a series of eight patients, we evaluated the feasibility, safety, and clinical outcomes of postoperative adjuvant eribulin administration in patients with localized STS, with a focus on older adults and those with notable comorbidities.
Anthracycline-based chemotherapy, with or without ifosfamide, has been the most extensively studied perioperative regimen for localized high-risk STS. However, its clinical benefits remain inconsistent, and treatment-related toxicity is a major concern, particularly in older adults and those with comorbidities. Large, randomized trials and meta-analyses have demonstrated the modest benefits of adjuvant anthracycline-based chemotherapy, while reporting substantial hematological and non-hematological toxicities that limit its feasibility in routine clinical practice.10,11
In the present series, although hematological toxicities such as neutropenia and leukopenia were relatively common, they were manageable with dose modification and supportive care. Importantly, no severe cardiac adverse events were observed, despite the inclusion of older adults and patients with pre-existing cardiovascular disease in this case series. Given that cardiotoxicity is a major limitation of anthracycline use in the perioperative setting, these findings suggest that eribulin may represent a safer alternative in selected patients.
Gemcitabine-based regimens, such as gemcitabine plus docetaxel, have also been explored as alternative perioperative treatments; however, their roles remain limited and their toxicity profiles vary across studies. 12 Although no direct comparisons can be made in this small retrospective series, the safety and feasibility observed in our cohort appear to be comparable to those reported for established perioperative chemotherapy regimens.
The clinical significance of our findings lies in demonstrating that postoperative adjuvant eribulin can be administered safely to patients who are considered poor candidates for anthracycline-based chemotherapy. Older adult patients and those with significant comorbidities are frequently encountered in clinical practice; however, evidence guiding perioperative systemic treatment in this population remains limited. Our results suggest that eribulin may serve as a feasible therapeutic option in this underrepresented group.
This interpretation is supported by previous clinical reports demonstrating that eribulin can be administered with manageable toxicity and a low incidence of clinically significant cardiac adverse events, even in patients with contraindications to doxorubicin.13,14 Furthermore, recent studies have explored its potential role beyond advanced disease. For example, a retrospective analysis demonstrated the feasibility of postoperative adjuvant eribulin administration in selected high-risk patients with liposarcoma who were not candidates for intensive chemotherapy. 15 In addition, preclinical studies have shown that eribulin exhibits antiproliferative activity comparable to that of anthracycline-based treatment in undifferentiated pleomorphic sarcoma models, providing a biological rationale for its potential use beyond liposarcoma. 16
Although eribulin has primarily been investigated in patients with advanced or metastatic liposarcoma and leiomyosarcoma, its clinical use varies by region. In the United States and Europe, its approval is limited to specific histological subtypes, whereas in Japan it is approved for soft tissue sarcoma regardless of histology and is used more broadly in routine practice. Therefore, the present study, which included multiple histological subtypes, reflects real-world clinical decision-making in Japan.
Furthermore, our previous real-world study of patients with advanced or metastatic STS demonstrated the favorable safety profile of eribulin, including in older adults and those with cardiovascular comorbidities. 17 Although that study focused on advanced disease, the present analysis extends these observations to the postoperative adjuvant setting, supporting the feasibility of eribulin use across different clinical contexts.
This study has several limitations. First, it was a retrospective case series conducted at a single institution with a small sample size. Therefore, the findings should be interpreted with caution, and no definitive conclusions regarding efficacy can be drawn. Second, the absence of a control group precludes direct comparison with other perioperative chemotherapy regimens, and selection bias is inherent, as eribulin was preferentially administered to patients considered unsuitable for anthracycline-based chemotherapy. Third, oncological outcomes were assessed descriptively without formal statistical analysis, and no sample size calculation was performed. Despite these limitations, this study provides clinically relevant real-world data on the feasibility and safety of postoperative adjuvant eribulin administration in a high-risk population that is often underrepresented in prospective trials.
Conclusion
Eribulin was feasible and well-tolerated as postoperative adjuvant chemotherapy in older adult patients and those with severe comorbidities with localized STS. Although the current case series was not designed to evaluate efficacy, the absence of severe treatment-related complications, including clinically significant adverse cardiac events, supports the potential role of eribulin as a therapeutic option for patients considered poor candidates for anthracycline-based perioperative chemotherapy. These findings, along with previous real-world safety data, suggest that eribulin may be a useful component in multimodal treatment strategies for carefully selected high-risk patients. Further studies with larger cohorts are warranted to clarify its role in the perioperative management of STS.
Supplemental material
Supplemental material - Postoperative adjuvant eribulin in high-risk patients with soft tissue sarcoma: A retrospective study of eight cases
Supplemental material for Postoperative adjuvant eribulin in high-risk patients with soft tissue sarcoma: A retrospective study of eight cases by Yudai Murayama, Hirokazu Ideta, Rumi Nakagawa, Yasutaka Sukawa, Masanobu Takahashi, Hiroyuki Kawashima, Kazutaka Kikuta in Rare Tumors
Footnotes
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki (as revised in 2024). According to the institutional policy of Tochigi Cancer Center, retrospective studies using fully anonymized clinical data are covered by the institutional comprehensive consent system and do not require individual Institutional Review Board approval. All patient data were fully de-identified prior to analysis.
Consent to participate
Informed consent for participation was waived due to the retrospective nature of the study and the use of anonymized data under the institutional comprehensive consent policy.
Consent for publication
Patient consent for publication was obtained as part of the institutional comprehensive consent process.
Author contributions
YM and KK contributed to the conception and design of the study. YM, HI, and RN collected the clinical data. YM analyzed and interpreted the data. YM drafted the manuscript. YS, MT, HK, and KK critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets presented in this study are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.