
Abstract
Background
Impostor phenomenon, characterised by self-perceived incompetence and inadequacy, has adverse effects on career progression and psychological wellbeing. While it is prevalent in various medical specialties, its prevalence in neurology is unknown.
Methods
Anonymous surveys were conducted among neurology trainees and junior neurologists over two windows across two major campuses in Singapore. The first window recruited incoming neurology residents (R0). The second window recruited neurology residents enrolled in any year of training (R1, R2, and R3) and junior neurologists (specialists practising within the first 2 years of accreditation). The second window included the same respondents from the first window. The Leary Impostorism Scale (LIS) was used, with a score of 15 indicating moderate or severe impostorism.
Results
The first window recorded five out of a possible five responses. The second window recorded 14 out of a possible 23 responses. The median LIS score started at 21 (interquartile range, IQR 15-25) among R0 residents, peaked at 28 (IQR 22-28) among R1 neurology residents, before declining to 15.5 (IQR 14-16.3) among R2 residents and 11 (IQR 10-16) among junior neurologists. No responses were received from R3 residents. There was a significant difference between the median LIS scores of each level of training (Kruskal-Wallis H = 10.398, p = 0.015). 10 out of 14 respondents (71.4%) had moderate or severe impostorism.
Conclusions
Impostor phenomenon is pervasive among neurology trainees and junior neurologists. Further studies are needed to investigate the impact of impostor phenomenon on neurology trainees and to identify means of mitigating it.
Introduction
Impostor phenomenon (IP), also known as impostorism, is a behavioural health phenomenon characterised by a self-perception of incompetence and inadequacy, leading to pervasive feelings of self-doubt, anxiety, depression, and a fear of being exposed as a fraud in their work. 1 It was originally described in high achieving women, but is now known to affect men as well.2,3 Importantly, IP is also common among junior healthcare professionals; A previous review reported a 33%–44% prevalence of clinically significant IP among resident trainees. 4 The prevalence of IP is likely to vary geographically and between different medical specialties. For example, one study reported that 94% of young neurosurgeons in Europe exhibited signs of IP. 5 IP has important consequences for career progression and psychological wellness. 6 In addition, it is associated with burnout in the medical profession. 7
Despite its potentially far-reaching consequences, IP remains poorly understood. If the literature on IP among healthcare practitioners has been scarce, it is virtually non-existent for neurologists. The psychological welfare of neurology trainees in Asia is of particular concern, since Asia has a disproportionately low neurologist-to-population ratio which heightens the impact of attrition and burnout. 8
Methods
We conducted a cross-sectional cohort study by anonymously surveying incoming and enrolled neurology residents, as well as junior neurologists from two major tertiary hospitals in Singapore.
In the Singaporean context, the completion of post-graduate year 1 (PGY1) followed by a 3-year internal medicine residency is a pre-requisite for joining the 3-year neurology residency programme. The 3-year internal medicine programme includes a solitary and continuous 3-month rotation in neurology, to be completed in the first or second year of the programme. Upon graduation from neurology residency, one will be certified as a specialist in neurology. In this study, a junior neurologist (JN) was defined as a neurologist practising within the first 2 years of specialist accreditation.
To assess for the presence of signs of IP, the Leary Impostorism Scale (LIS) was used; this is a seven-item English survey scale that has been validated as a measure of IP with high internal reliability, significant positive correlation with the longer Clance Impostor Phenomenon Scale (CIPS), and a low respondent burden.9–11 The range of possible scores is 7-35, with any score above 7 suggesting some degree of IP, and with a higher score indicating stronger IP features in the respondent. A score of 15 or more was taken to indicate the presence of moderate or severe impostorism, since a respondent finding the majority (at least four) of the seven items on the LIS to be ‘moderately characteristic’ for him/her-self would score at least 15 points.
The survey was administered digitally via an encrypted virtual platform created by a Singaporean government agency. The survey was advertised, by means of text message broadcasts, as a brief and optional one-minute survey. To maintain anonymity, the survey collected only the respondent’s year of training in neurology in addition to the LIS, omitting their names, sex, and ethnicities. The year of training in neurology was defined by the grade of residency seniority of the resident (R1, R2, or R3) rather than the number of years spent in training. An optional free-text field was available for the respondent to provide narrative comments on IP in neurology.
The surveys were administered over two windows. The first window recruited incoming neurology residents (R0) in June 2024, the month before they commenced neurology residency. The second window recruited enrolled neurology residents in any year of training (R1, R2, and R3) and JN from July 2024 to Oct 2024, including the respondents from the first window who had now assumed their appointments as neurology residents.
Data from the collected responses were analysed using SPSS software (version 26.0, Chicago, IL, USA). The Kruskal-Wallis test was used to study independent variables in groups of two or more.
Results
In the first window, responses were solicited from five R0 residents and five responses were received, with the median LIS score being 21 (interquartile range, IQR 15-25).
In the second window, responses were sought from a total of 23 prospective respondents (comprising five R1 residents, eight R2 residents, three R3 residents, and seven JN physicians), and 14 responses were received. The median LIS scores for R1, R2, and JN were 28 (IQR 22-28), 15.5 (IQR 14-16.3), and 11 (10-16) respectively. No responses were received from R3 residents.
Mean and median Leary Impostorism Scale scores for each year of training. IQR, interquartile range; JN, junior neurologist (a specialist in neurology in the first two years of specialist accreditation); LIS, Leary Impostorism Scale; R0, incoming neurology resident; R1, first-year neurology resident; R2, second-year neurology resident; R3, third-year neurology resident.

There was a significant difference between the median LIS scores of each level of training (Kruskal-Wallis H = 10.398, p = 0.015). Figure 1 shows the boxplot of median LIS scores and their IQR. Boxplot of Leary Impostorism Scale scores, showing the median, interquartile range, and range of scores at each stage of neurology training. LIS, Leary Impostorism Scale; JN, junior neurologist (a specialist in neurology in the first 2 years of specialist accreditation); R0, incoming neurology resident; R1, first-year neurology resident; R2, second-year neurology resident.
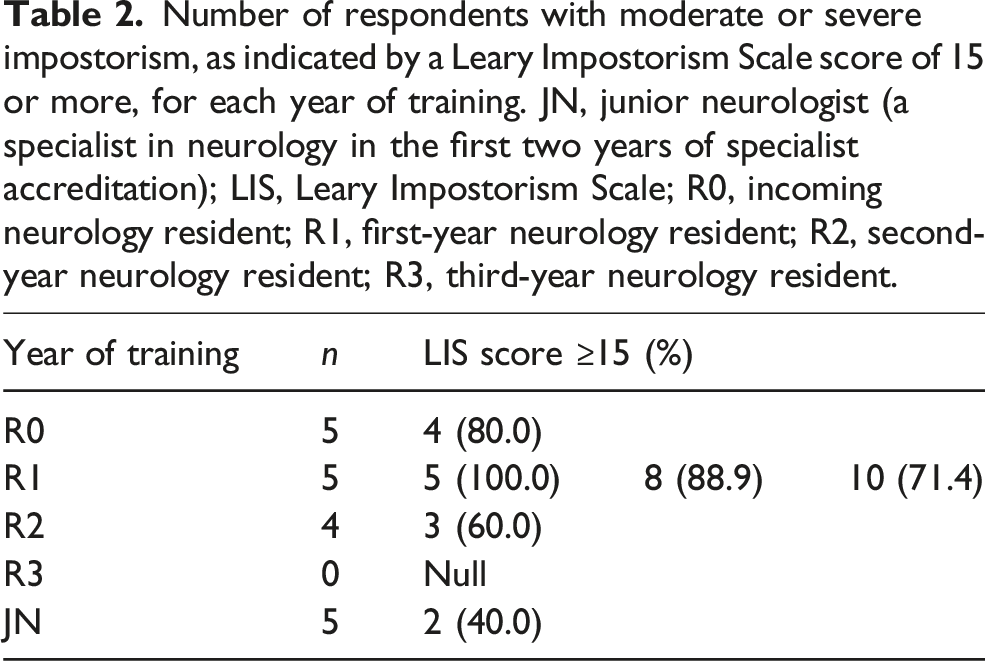
Number of respondents with moderate or severe impostorism, as indicated by a Leary Impostorism Scale score of 15 or more, for each year of training. JN, junior neurologist (a specialist in neurology in the first two years of specialist accreditation); LIS, Leary Impostorism Scale; R0, incoming neurology resident; R1, first-year neurology resident; R2, second-year neurology resident; R3, third-year neurology resident.
Only two respondents provided narrative comments. One R2 resident expressed gratitude for the “nice and forgiving” culture in the neurology department, which alleviated feelings of inadequacy. Another R2 resident opined that the transition from internal medicine resident to neurology resident required the navigation of a “steep learning curve”, which was compounded by the “long gap” between their neurology rotation in internal medicine residency and the commencement of neurology residency.
Discussion
Our study provides important insights into IP in neurology trainees and in junior neurologists.
First, IP was more pervasive among first-year neurology residents (R1) than among incoming neurology residents (R0). Since the five R0 and five R1 respondents in our study were the same respondents answering the same survey questions separated by a brief interval of only one to 3 months, it is likely that the start of neurology residency exacerbated IP.
A plausible explanation for the above observation is that increased exposure to neurology expands a resident’s metacognitive ability to recognise his/her own deficits and knowledge gaps. Daily exposure to neurology would likely help new R1 residents identify blind spots in their knowledge, transferring knowledge gaps from things they did not know existed, to things they know exist but which they do not yet comprehend. As suggested by the Dunning-Kruger effect, this would likely narrow the gap between self-perceived ability and actual ability, but the resulting correction of self-perceived ability is likely to intensify feelings of inadequacy and hence IP. 12
The narrative comments recorded also suggested additional explanations for the aggravation of IP during the transition from R0 to R1, which may be specific to the local structure of residency programmes. The promotion from internal medicine resident (also known as a ‘junior resident’ in the local context) to neurology resident (‘senior resident’) carries an increased weight of expectations and a wider scope of responsibilities. Beginner’s uncertainty about one’s capacity to fulfil these expectations and responsibilities may deepen IP. We also acknowledge that the long latency between a resident’s earlier neurology rotation during internal medicine residency and the subsequent commencement of neurology residency may aggravate IP. A previous study showed that the current level of neurology teachings in a Singaporean internal medicine programme is already inadequate to instill confidence in managing neurological conditions. 13 An internal medicine resident’s period away from neurology, which can last for one to two consecutive years before the commencement of neurology residency, may further weaken a resident’s recollection of any teachings received, hence further eroding confidence.
The narrative comment about a “nice and forgiving” culture alleviating IP symptoms may have suggested that institutional and departmental cultures can significantly influence the prevalence of IP among neurology trainees, and that the effect of such cultures can be perceived by individuals. Previous studies have shown that high performance pressure predicted more intense impostorism across different professions. 14 Furthermore, a competitive work culture exacerbates IP by encouraging a self-threatening form of social comparison with high-performing colleagues, internally highlighting contrast between oneself and one’s colleagues instead of fostering assimilation in the workplace. 15 Although the narrative feedback we collected was limited in quantity, it may encourage improvement of modifiable work cultures, in order to ameliorate culture-imposed performance pressure and strengthen workplace collaboration over competition. For example, the normalizing of experiences through peer-support groups and availing of mentor support are examples of interventions that have been proposed as organisational means of mitigating IP. 16
Another insight gleaned from our study was that IP abated with increasing grades of residency seniority. This was an expected finding, given that progression within the residency programme is dependent on documentation of the necessary levels of competence, and greater competence instills greater confidence in one’s own ability. It is likely that among more senior physicians, symptoms of IP would be less prevalent. For perspective, one study of family medicine residency programme directors found only 20% scoring 15 or more on the LIS. 17 In contrast, 71.4% of our cohort, who were considerably more junior physicians, scored 15 or more, though it is uncertain how much of the difference may be accounted for by differences in the practice of family medicine and neurology.
Finally, our study suggests that IP is pervasive among neurology trainees and junior neurologists in Singapore. The high prevalence of IP among neurology trainees and junior neurologists should be of particular concern in Asia because of the low neurologist-to-population ratio in Asia, which contains only 20% of the world’s neurologists despite constituting 60% of the world’s population. 8 IP predisposes sufferers to multiple risk factors for burnout, and thus can potentially exacerbate manpower shortages. Individuals with IP are at greater risk of employing avoidant coping strategies (such as giving up, denial, or even substance abuse) as opposed to active coping strategies (such as seeking emotional support). 16 This puts them at greater risk of emotional exhaustion because avoidant coping strategies tend to only provide temporary relief. 16 In addition, persons with IP tend to attribute negative events to internal causes, and hence expend more emotional resources toward improving their performance, further compounding the problem of emotional exhaustion. 18 Emotional exhaustion is a prominent dimension of burnout which, among physicians, is associated with absence from work, changing to part-time work, an aversion to call duty, early retirement, and leaving the practice of medicine. 19
Our study had several limitations. Our ethical commitment to keeping the survey anonymous, to avoid the risk of workplace stigma and prejudice against the residents who responded, meant that we could not collect more granular data from the small pool of potential respondents, such as age, sex, and the number of years spent in training. This limited our ability to conduct deeper analyses. For instance, while we found that IP waned with increasing grades of residency seniority, we were unable to investigate the relationship between IP and the total time spent in neurology. This is a point of interest, since an inverse relationship may suggest that longer rotations in neurology prior to the commencement of neurology residency can help alleviate IP in R1 residents.
As our survey was optional, our response rate of 61% (14 out of 23 potential respondents) in the second window exacerbated the problem of a small sample size. This may have created selection bias in our results. It is possible that the extremes of the IP spectrum (from either end) prevail within the non-respondents, potentially causing their disinterest and hence non-response. For instance, we received no responses from final year (R3) residents. This may have simply been an artefact of the small number of potential R3 respondents at the time of the survey (there were only three of them to invite). However, it is also possible that R3 residents, being at the cusp of completing their training, may have had a heightened awareness of their knowledge gaps, greater concerns about disclosing psychological vulnerabilities, and a smaller appetite for reputational risk (especially given the small R3 cohort size which can increase the risk of identification despite our efforts at anonymisation).
While lengthier questionnaires have been employed to diagnose different dimensions of IP, the dimensionality of IP remains unclear. 20 Since it has also been suggested that IP may be a unidimensional construct, we utilised the LIS and its brevity as a means of identifying IP with minimal respondent burden. 21 However, unlike the more widely used CIPS, the LIS does not have any suggested cut-off score for the diagnosis of clinically significant IP. 22 We attempted to mitigate this problem by defining moderate impostorism using an LIS score of 15 or more, as explained in our Methods section.
We have provided important insights into a hitherto unexplored area of neurology trainee wellbeing in Asia. Future research should focus on detailing the impact of IP on neurology trainees. Furthermore, studies are needed to design and validate interventions aimed at mitigating IP in first-year neurology residents, who are the worst afflicted. Based on our study findings and hypotheses, the following interventions may be explored: (1) Courses and workshops to equip incoming neurology residents with the skills needed to cope with the scope of responsibilities fulfilled by a ‘senior resident’, (2) scheduling neurology teachings or rotations closer to the start of neurology residency, and (3) mitigating competition between trainees by setting up peer-support groups and availing mentorship support.
Conclusions
This study suggests that impostor phenomenon is pervasive among neurology trainees, and peaks at the commencement of neurology residency. More research is needed to delineate its impact, and to find means of mitigating impostorism.
Supplemental Material
Supplemental Material - Impostor phenomenon in neurology trainees peaks at commencement of residency
Supplemental Material for Impostor phenomenon in neurology trainees peaks at commencement of residency by Zhibin Tan, Wai Dic Foong, Nara Tiara Sugianto, Yi Rong Chiew, You Jiang Tan, Shih Hui Lim in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
We would like to acknowledge the respondents who participated in this study for contributing to our understanding of impostor phenomenon among junior neurologists.
Ethical considerations
Ethical approval for this study was waived by the SingHealth Centralised Institutional Review Board because this study involves only educational tests, surveys, interviews or observation of public behaviour (CIRB Ref 2024-3604). This study was conducted in accordance with the principles set out by the Declaration of Helsinki.
Consent to participate
Informed consent was not sought for the present study because the need for written consent were waived by the SingHealth Centralised Institutional Review Board. In accordance with the study protocol submitted for exemption, all participants were informed that the survey was optional, and that responding to the survey was taken to be an implied agreement to publish their anonymised data in scientific journals.
Author contributions
TZB conceptualised and designed the study and was involved in the acquisition and analysis of data, interpretation of results, and drafting and editing of the manuscript. FWD, NTS, and CYR were involved in the acquisition and analysis of data, interpretation of results, and editing of the manuscript. TYJ and LSH supervised the project, and were involved in the analysis of data, interpretation of the results, as well as editing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset generated and analysed during the current study is included in its supplementary material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.