
Abstract
Introduction
With an increasing burden of cardiovascular disease, there has been rising demands for outpatient cardiology services. In this study, we reviewed the cardiology referral patterns from primary care to a tertiary cardiac centre, and evaluated their longer term clinical outcomes based on referral symptomatology as well as risk stratification.
Methods
Consecutive outpatients referred from primary care to a national cardiac centre between March 2015 to December 2020 were included. Patients with known coronary artery disease (CAD) were excluded. Chest pain patients were stratified by pre-test probability (PTP) of obstructive CAD using chest pain risk scores and the rest by age and sex. Outcomes studied included mortality and major adverse cardiovascular events (MACE).
Results
A total of 33,244 patients (11,865 chest pain, 3427 palpitations, 2844 dyspnoea) were included. In patients with chest pain, the 3-year mortality and MACE rates were 1.25% and 3.19% respectively. Patients with higher PTP of CAD demonstrated significantly higher rates of adverse events. In patients with palpitations, the 3-year mortality and MACE rates were 0.86% and 1.55% respectively. Males aged >65years had significantly higher risk of 3-year mortality (p < .00.5). In patients with dyspnoea, the 3-year mortality and MACE rates were 3.34 and 4.44% respectively. Subsets of younger age and/or female sex had lower rates of adverse events.
Conclusions
While long term adverse clinical outcomes were generally low in this stable outpatient cohort, risk stratification allowed for identification of an even lower risk subset of patients for whom additional testing may potentially not yield incremental clinical benefit.
Introduction
With a rapidly aging population, both the global and local burden of cardiovascular disease have increased over time, with cardiovascular disease being a leading cause of mortality and a major contributor to disability.1,2 In tandem, healthcare needs including the demand for both outpatient and inpatient cardiology services have multiplied. The rising demand for outpatient cardiology services necessitates more efficient utilisation of healthcare resources. This may involve amongst others having efficient referral protocols between primary and tertiary care providers, accurate risk stratification and reduction of unnecessary testing. In this study, we reviewed the cardiology referral patterns from primary care to a tertiary cardiac centre, and evaluated their longer term clinical outcomes based on referral symptomatology as well as risk stratification.
Methods
Study population
Consecutive patients referred from public primary care polyclinics to the outpatient cardiology clinic at a local tertiary centre between March 2015 to December 2020 were included. This local cardiology tertiary centre receives approximately half of all public outpatient cardiology referrals from primary care. Patients with known CAD were excluded. Data collected during the initial visit include demographics, cardiovascular risk factors and indications for referral. Cardiovascular risk factors include smoking status, hypertension, hyperlipidaemia, and diabetes mellitus. Indications for referral was based on the information in the referral letter and the patient’s presenting complaint and categorised into four main groups: chest pain, palpitations, dyspnoea, and others. Patients with multiple symptoms were grouped under ‘others’. As this study involved the analysis of de-identified patient data only, waiver of ethics review was accorded by the institution ethics review board.
Risk stratification
Chest pain patients were risk stratified according to their pretest probability (PTP) of obstructive CAD using CAD consortium score (CCS) – clinical. The CCS is a validated tool that uses demographic and clinical risk factors (including age, sex, history of diabetes, hypertension, hyperlipidaemia and smoking) as well as chest pain type, to estimate the PTP of CAD. 3 In patients who presented with palpitations and dyspnoea, these were stratified according to their age and sex.
Clinical outcomes
The primary outcome studied was all-cause mortality. Secondary outcomes studied included major adverse cardiovascular events (MACE) defined as cardiovascular (CV) death, non-fatal myocardial infarction (MI) and/or non-fatal stroke, and its individual components. All outcomes were obtained from national databases. 1-year and 3-year outcomes were studied. Mortality and MACE outcomes were available till December 2021 and December 2019 respectively. For all-cause mortality and CV death, patients enrolled by Dec 2020 and Dec 2018 were included for 1-year and 3-year outcomes respectively. For AMI, stroke, and MACE, patients enrolled by December 2018 and December 2016 were included for 1-year and 3-year outcomes respectively.
Statistical analysis
Continuous variables were expressed as mean values with their associated standard deviations and categorical variables were expressed as proportions. Proportional hazards models were used to estimate the hazard ratios (HR) with 95% confidence intervals (CI) for the various clinical outcomes. Chest pain patients were stratified by CCS PTP, while patients with palpitations and dyspnoea were stratified by age and sex. All analyses were performed using Stata version 16 (StataCorp, College Station, Texas, United States of America) and a p value of <0.05 was taken to be significant.
Results
Between March 2015 till December 2020, 35 028 patients were referred from government polyclinics to the tertiary centre’s outpatient Cardiology clinic. Of the 35 028 patients, 1784 patients with a known history of CAD were excluded. Of the remaining 33 244 patients, 11 865 were referred for chest pain, 3427 for palpitations, 2844 for dyspnoea, and 15 108 for other reasons (Figure 1). Indications for outpatient cardiology referrals from primary care. CAD; coronary artery disease.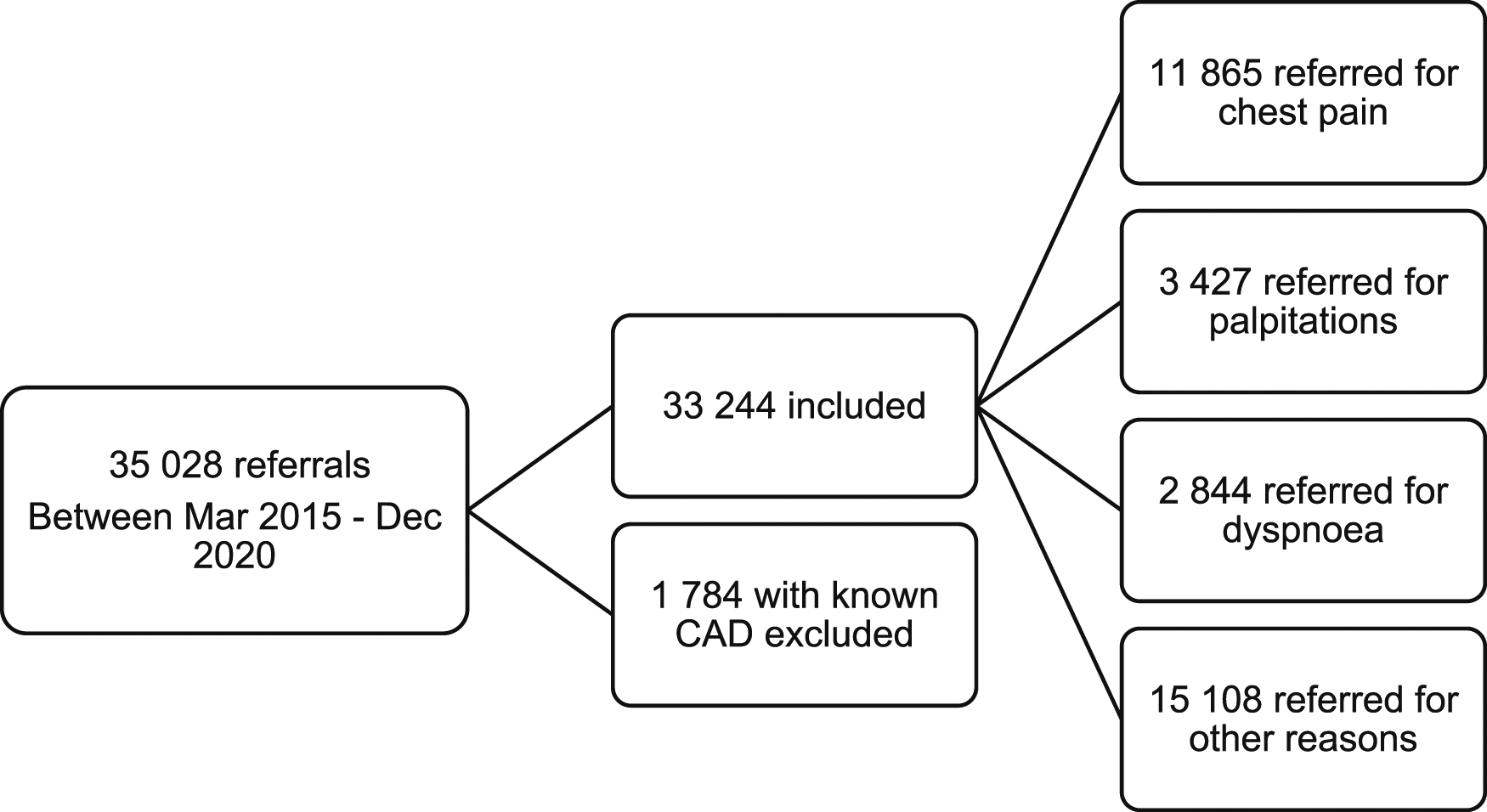
Baseline clinical characteristics of study population.

1-year and 3-year clinical outcomes of patients with chest pain, across the different pre-test probabilities (PTP) of obstructive coronary artery disease calculated using the CAD consortium score – clinical.


HR; hazard ratio. CI; confidence interval. CV; cardiovascular. MACE; major adverse cardiovascular events. MI; myocardial infarction.
1-year and 3-year clinical outcomes of patients with palpitations, stratified by age and sex.
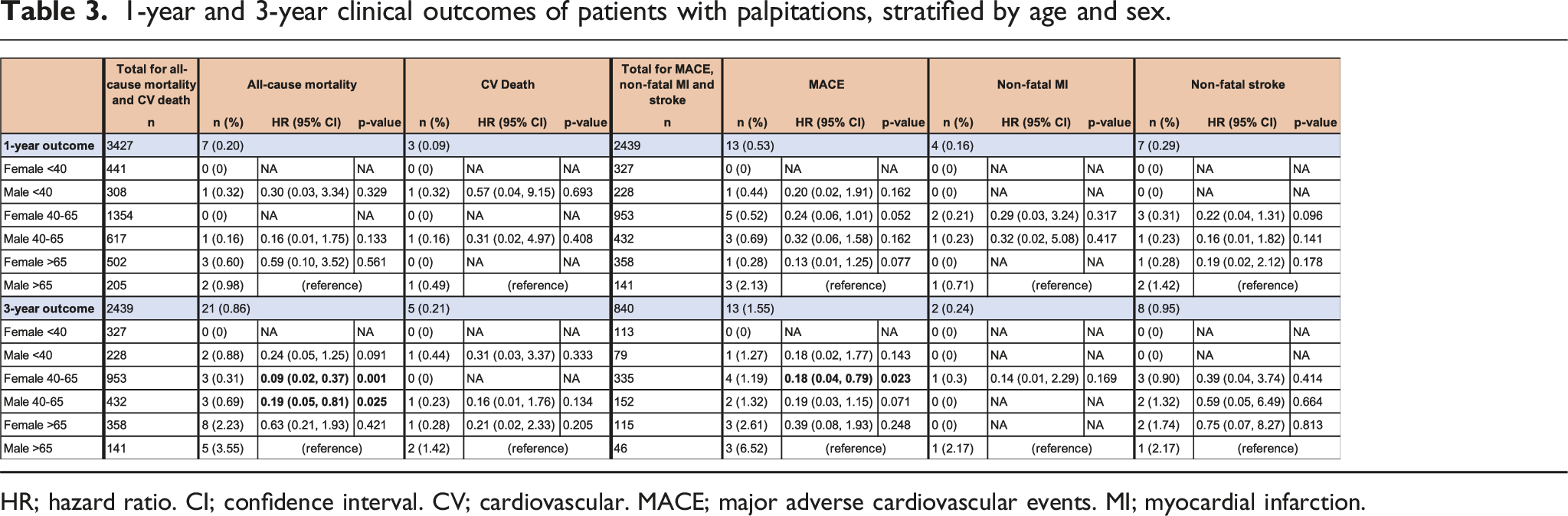

HR; hazard ratio. CI; confidence interval. CV; cardiovascular. MACE; major adverse cardiovascular events. MI; myocardial infarction.
1-year and 3-year clinical outcomes of patients with dyspnoea, stratified according to age and sex.


HR; hazard ratio. CI; confidence interval. CV; cardiovascular. MACE; major adverse cardiovascular events. MI; myocardial infarction.
Discussion
In this study, several important findings are emphasised: a) Chest pain, palpitations, and dyspnoea form a significant proportion of outpatient cardiology referrals, of which chest pain predominates; b) In chest pain patients, while the overall longer term adverse event rate is low, risk stratification aids in further identifying patients who are at even lower risk; c) Similarly, for patients presenting with palpitations or dyspnoea, the overall longer term adverse event rate is low, with the younger and/or female patient at lower risk of adverse events. These highlight a subset of patients for whom additional testing may potentially not yield incremental benefit.
Our study found that the top reasons for primary care to refer patients to the cardiology clinic were for chest pain (35.7%), followed by palpitations (10.3%), and then dyspnoea (8.6%). In a previous older local study, chest pain, breathlessness and palpitations accounted for 47.7%, 13.2% and 10.8% of the referrals from primary care and the emergency department to the cardiology outpatient clinic. 4 A study by Lenderink et al observed that in the Netherlands, chest pain, palpitations, and dyspnoea account were the top three reasons for outpatient cardiology referral, and represented 49%, 12% and 11% of all referrals respectively. 5 Our study reported fewer referrals for chest pain, possibly because patients with multiple complaints including chest pain were grouped under ‘others’ and this study did not include referrals from the emergency department.
In the chest pain cohort, the overall rate of adverse events was low with the rates of all-cause mortality and MACE at 3-year were 1.25% and 3.19% respectively. The PTP of obstructive CAD correlates well with adverse outcomes at 1-year and 3-year follow-up. In the very low risk group with PTP <5% which also made up about half the chest pain cohort, the 3y mortality rate was 0.81%. This suggests that risk scoring of PTP of obstructive CAD is useful as a risk stratification tool to identify patients who are at lower risk of longer-term adverse outcomes. Various studies have validated the use of PTP risk scores in predicting obstructive coronary artery disease,6,7 and MACE.6,8,9 In another local study, similar findings of have also been found with the rates of adverse events at 1 year in an outpatient chest pain cohort correlating in tandem with the PTP of CAD. 10
In this study, patients presenting with palpitations and dyspnoea also had overall low rates of adverse events. Prior studies have also demonstrated a low mortality rates amongst patients with palpitations presenting to primary care,11,12 the emergency department, 13 as well as the outpatient cardiology setting, 14 though the relationship between age, sex and risk of adverse events was not established. In the palpitations and dyspnoea cohort, risk stratification by age and sex generally correlated well with rates of adverse outcomes, with the younger and/or female subsets having the lowest event rate. In both the palpitations and dyspnoea cohort, the 3-year mortality and MACE rate in females <40 years old was 0%.
The rate of adverse events in the dyspnoea cohort was the highest as compared to the chest pain and palpitations cohorts. In another study looking at outcomes of patients referred from primary care to the cardiology outpatient clinic, the 24-month mortality of patients with dyspnoea was 4.9% and 2.1% in men and women respectively, higher than in patients with palpitations and chest pain. 14 In our study, the higher rate of adverse events in the dyspnoea cohort may be related to the fact that the dyspnoea cohort was generally older, with a mean age of 63.4 years compared to 53.8 years in the chest pain cohort and 52.3 years in the palpitations cohort.
Overall, this study highlights that in a stable outpatient cohort, the cardiovascular event rate is generally low up to 3 years follow up. Further risk stratification either by PTP of CAD for chest pain patients or age/sex for palpitations/dyspnoea patients identified a subset of even lower risk patients. This potentially opens up the opportunity to explore detailed protocols to either safely defer referrals or reduce additional testing in especially the very low risk subset. For patients with chest pain, the consideration to defer testing in low-risk patients is in line with recommendations from the European Society of Cardiology and the American Heart Association guidelines.15,16 A prospective observational cohort study at a chest pain unit found that patients with low PTP of obstructive CAD were at very low risk of acute coronary syndrome or a true-positive stress test, and also supports that in this group of patients, stress testing may be safely deferred. 8 Another study randomised symptomatic patients with suspected CAD and low PTP to deferred testing versus usual testing found that demonstrated that the strategy of deferred testing was safe with no observed adverse outcome events, fewer catheterisations without obstructive CAD, and similar symptom relief compared with usual testing. 17 Reductions in unnecessary referrals and testing in the low-risk population may help reduce the burden on our healthcare system and allow better utilisation of our limited healthcare resources, given that not a small proportion of patients fall into the low-risk group. For patients, these may reduce their financial burden and also avoid the potential anxiety and morbidity that may arise from unnecessary testing and false positive results. A study in the United States found that nearly a third of cardiac imaging stress tests were inappropriate and was associated with a cost of $494 million annually. 18
The key strengths of the paper are the large patient numbers and comprehensive longer term clinical outcomes obtained from national databases. However, there are several limitations. Whether testing or the treatment initiated could have potentially improved clinical outcomes was not possible to ascertain as these data was not readily available. In a previous older local study by Kwok et al. in 2008 which studied referrals from primary care and the emergency department to the outpatient cardiology clinic, 79.2% of the patients referred underwent additional cardiac testing, and with the yield for cardiac abnormalities with testing being generally low. 4 Second, missing data precluded the assessment of risk scores for a number of patients with chest pain and this may have introduced bias. In addition, beyond the prevalence of traditional cardiovascular risk factors of diabetes mellitus, hypertension, hyperlipidaemia, data on other risk factors (eg. obesity, lung disease, etc) were not available.
While these limitations did not impact on the reporting of hard clinical outcomes in each subset of patients, each patient’s unique characteristics and comorbidities would need to be considered when risk stratifying patients and deciding on subsequent investigations and treatment.
In conclusion, chest pain, palpitations, and dyspnoea are common reasons for outpatient cardiology referral from primary care. While long term adverse clinical outcomes were generally low in this stable outpatient cohort, risk stratification allowed for identification of an even lower risk subset of patients for whom additional testing may potentially not yield incremental clinical benefit.
Footnotes
Acknowledgements
The authors would like to express our heartfelt thanks to nurses from the Heart Care Unit at the National Heart Centre Singapore and Mr Lau Yee How from the Singapore Cardiac Data Bank at the National Heart Centre Singapore for their invaluable help in this project.
Author contributions
All authors were involved in conceptualisation the study and data acquisition. YYC, YJ, and JY were involved in the analysis and interpretation of data. YYC and JY drafted the initial manuscript. All authors reviewed and contributed to the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof. Jonathan Yap has received speaker’s honorarium from Abbott, Biosensors, Biotronik, Boston Scientific, Edwards, GE healthcare, J&J, Kaneka, Medtronic and Terumo. Prof. Yeo Khung Keong has received research funding from Amgen, Astra Zeneca, Abbott Vascular, Bayer, Boston Scientific, Shockwave Medical, Novartis (via institution); Consulting fees from Abbott Vascular, Medtronic, Novartis, Peijia Medical; Speaker fees from Shockwave Medical, Abbott Vascular, Boston Scientific, Medtronic, Alvimedica, Biotronik, Orbus Neich, Shockwave Medical, Amgen, Novartis, Astra Zeneca, Microport, Terumo, Omnicare. Prof. Yeo is also co-founder and owns equity in Trisail for which Orbus Neich is an investor.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.