
Abstract
Foul-smelling vaginal discharge in adolescents often stems from infectious origin, foreign body insertion, neoplasm, congenital anomaly, and sexual abuse. Diagnosing the causes of the discharge remains challenging, especially in cases where sexual and reproductive health awareness is relatively low in the population from marginalized ethnographies and socio-cultural backgrounds. Suspicion of sexual abuse must be explored carefully and sensitively. A history of sexual exposure might not be forthcoming in adolescents where premarital sex is frowned upon. The process of eliciting the causation may be a challenge to healthcare professionals, delaying the diagnosis and subsequent management. In rare circumstances, imaging studies may help confirm the origin of the infection, giving insight into the presentation’s aetiology. We describe a case of Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) Syndrome presented with foul-smelling vaginal discharge in a newly attained menarche girl in the North-East region of Peninsular Malaysia. We also discussed the theories and reasons behind the occurrence of such a presentation, along with the diagnostic dilemma in this current case.
Introduction
Foul-smelling vaginal discharge in adolescents is uncommon. It is associated with sexual-transmitted diseases, fungal infections, bacterial vaginosis, vulvar skin disease or vaginal neoplasm. The possibility of sexual abuse needs to be explored sensitively. A predilection of self-exploration or introduction by siblings or playmates should not be overlooked, though such findings are more commonly seen among children aged between three to 9 years old. 1 Furthermore, intra-vaginal foreign body insertion should also be considered specifically among individuals with age-appropriate curiosity.
However, a timely but thorough evaluation of such cases is usually not forthcoming. Of note, history-taking related to sexual and reproductive health issues is challenging among patients from South-East Asia, especially those from marginalized socio-demographic backgrounds. 2 Anxiety and embarrassment from a pubertal child may even contribute to the diagnostic challenge.
Consideration should also be given to sources stemming from congenital malformation. Herein, we present an atypical presentation of Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) Syndrome with foul-smelling vaginal discharge in a 12-year-old Muslim girl from Malaysia.
Case report
A 12-year-old girl presented to our centre with a history of foul-smelling vaginal discharge for 7 months. Her mother brought her. She attained menarche at the age of 11 years old. She claimed that her menses were regular but prolonged. Normal flow lasted about 5 days, followed by a scanty foul-smelling brownish discharge until the next menses. She denied any history of fever, dysmenorrhea, foreign body insertion, or any sexual exposure. There was no suspicion of sexual abuse. She denied any UTI symptoms. She was never on any treatment. The patient came from a single-mother family. Her mother was unable to support her financially. Following her father’s recent demise, she was patronized by an orphanage institution. She was avoidant towards group activities and isolated herself from the rest of the residents. She also suffered from low self-esteem and embarrassment because of her problem. She was born full-term through an uncomplicated spontaneous vaginal delivery. Other histories were insignificant.
At our centre, her vital signs were normal, and she was afebrile. She was quiet and shy and avoided eye contact during the consultation. Abdominal examination revealed a soft, non-tender abdomen with no palpable mass. Perineal examination showed normal external genitalia. Pus discharge was seen coming out from the introitus, and the hymen was intact. Per rectal examination revealed a bulge about 6 cm from the anal verge. A low vaginal swab revealed Streptococcus beta-hemolytic Group B organism isolated with numerous pus cells and epithelial cells of 10–15. Her blood investigations, including her renal function test, were normal.
A bedside ultrasound scan showed a homogenous mass of about 7 cm × 5 cm within the vagina. Subsequently, CT abdomen and pelvis revealed uterus didelphys, obstructed left hemivagina with fluid collection measuring 6.4 cm × 3.6 cm × 7.4 cm, and left renal agenesis (Figures 1–3). Coronal-reformatted, contrast-enhanced CT image demonstrates the normal appearance of the right kidney with an absence of the left kidney. A fluid collection (yellow arrow) with HU 7–10 was seen in the pelvic cavity. Coronal-reformatted, contrast-enhanced CT image demonstrates the presence of right (red arrowhead) and left (yellow arrowhead) uterine cavities. Sagittal-reformatted, contrast-enhanced CT image demonstrates the left uterine cavity (yellow arrowhead) communicating with the fluid collection (yellow arrow). Anteriorly the urinary bladder and posteriorly, the rectum are normal in morphology.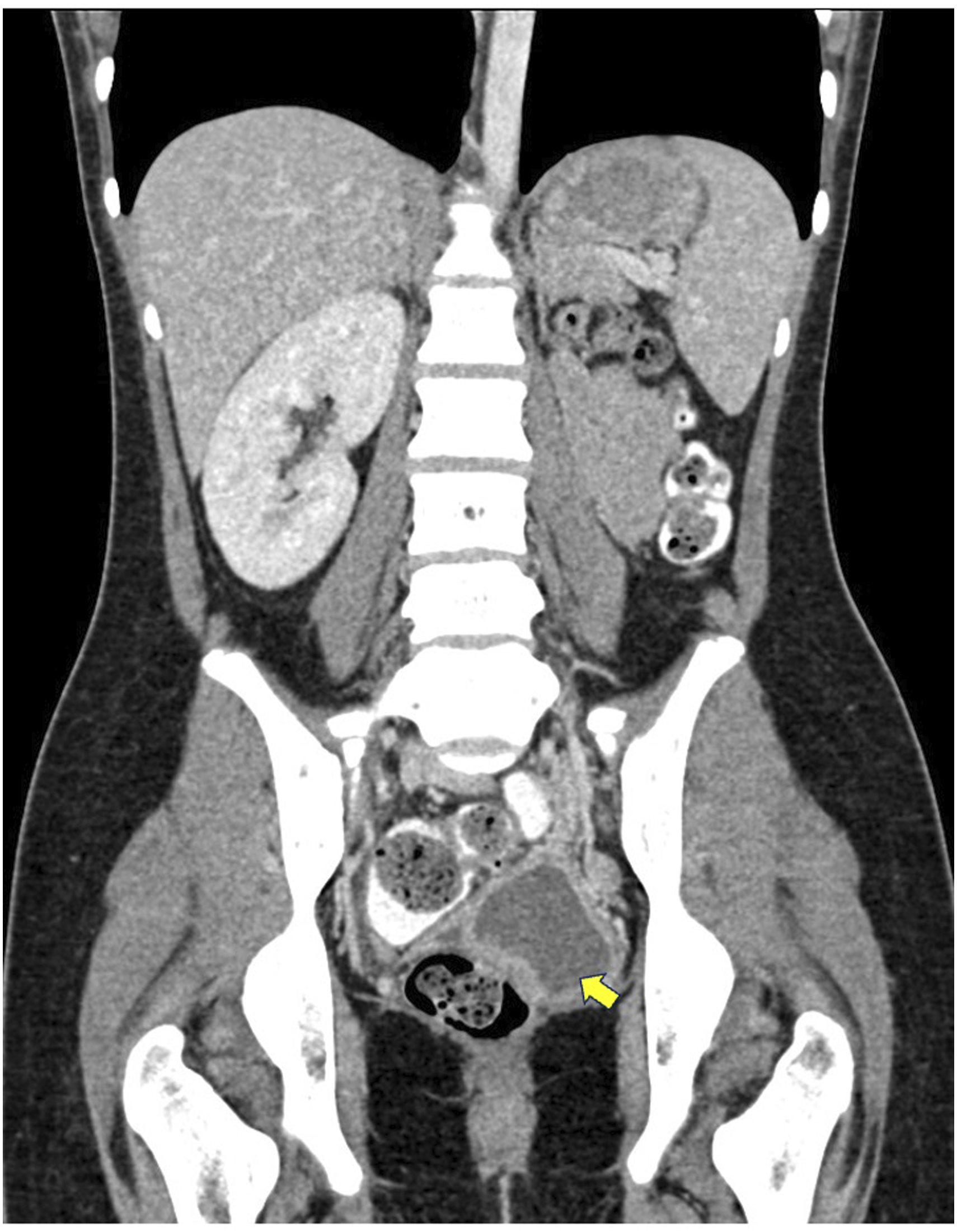


The risk of incomplete excision and the need for possible further surgery was explained prior to the operation. The case proceeded with septum removal vaginally. The septum was about 0.5 cm thickness situated at the upper 1/3 of the left vagina. There was a small punctum releasing yellowish foul-smelling pus seen at the bulge. She was discharged with a 2-weeks course of antibiotics.
She was satisfied with her health condition at 4 months post-septal removal follow-up. Her menses were regular, lasting for 5–7 days. She had mild dysmenorrhea on Day 1–2 menses, which did not require any analgesia. The possible long-term complications of endometriosis and subfertility were explained to both patient and her mother. She was advised in the future that, if she gets pregnant, she to come for an antenatal checkup in our centre.
Discussion
Herlyn-Werner-Wunderlich (HWW) syndrome is a rare urogenital-congenital anomaly. Named after its initial founders, Herlyn and Werner in 1971, as well as Wunderlich in 1976, who described an association of right renal aplasia with a bicornuate uterus and simple vagina in the presence of an isolated hematocolpos. The disease was further named Obstructed HemiVagina and Ipsilateral Renal Anomaly (OHVIRA) syndrome, representing the triad of uterus didelphys, obstructed hemivagina and ipsilateral renal agenesis.
Acien proposes the vagina is completely of the mesonephric origin, whereas the uterus and cervix may have derived from the fused-paired paramesonephric ducts (2nd part) and divergent distal paramesonephric ducts (3rd part). 3 The agenesis of the ureteric bud and, eventually the adjacent ureter and kidney are caused by the failure of the metanephric diverticulum development (around 5 weeks). The mesonephros plays a role in developing and to position the paramesonephric duct. The paramesonephric duct is position laterally to the mesonephric duct, before crossing it anteriorly and medially to it in a converging manner. Stemming from the malpositioning of the paired paramesonephric duct, the two hemiuteri and hemicervices fail to unite, resulting in uterus didelphys.
In the case of OHVIRA syndrome, the ipsilateral mesonephric duct developmental arrest causes a domino effect on the failed development of all three components (development of uterus didelphys, distal hemivagina obstruction, and ipsilateral renal agenesis.
The disorder poses an incident rate of 0.1–3.8%. It is often presented with severe dysmenorrhea and a palpable mass due to unilateral hematocolpos in early menarche. 4 Diagnosis of OHVIRA is usually made by exploring the cause of dysmenorrhea stemming from obstructive hemivagina and hematocolpos, which start shortly after menarche in adolescence. 5 In most cases, menses often flow normally from the patent hemivagina, contributing to its diagnostic dilemma and delayed management. 6
Typically, patients with OHVIRA Syndrome are often presented with dysmenorrhea, cyclical lower abdominal pain, and tender vaginal mass. 7 Additionally, the persistent buildup of blood products may cause urinary retention secondary to mass effect and further to accentuate urinary tract infections. 8 Also, retrograde expulsion due to uterine contraction may cause endometrial implantation into surrounding pelvic regions (endometriosis). 7 Echoing some published reports, we postulate that the formation of pyocolpos in our patient originated from blood collection in obstructed hemivagina, which became a nodus of infection made possible by the presence of fistula in the wall of the vaginal septum.5,8
Magnetic resonance imaging (MRI) remains the diagnostic gold standard for this syndrome due to its multiplanar and wide range of view. 9 MRI may help detect dilated pelvic structures due to fluid accumulation and adhesions, pelvic inflammation, and endometrioma.7,8 However, if such imaging modality is unavailable in most clinical settings, a bedside ultrasound by an experienced gynaecologist may suffice for an initial diagnostic view. Our case herein is supported by a CT scan imaging, which explains the causation and source of the foul-smelling vaginal discharge. Therefore, adolescents with persistent offensive vaginal discharge should be referred to a gynaecologist for further evaluation.
Early diagnosis is crucial to prevent complications such as infertility and endometriosis, as well as warranting a limited usage of nephrotoxic drugs among patients with OHVIRA. 6 Moreover, the psychological well-being of an OHVIRA patient should be emphasized. Often, they are misdiagnosed and partially treated for their symptoms. 10 Little care is given to the inner struggle coupled with the social stigma stemming from their cultural and religious background. Such was the case of our patient herein, who came from a low socioeconomic family and the discussion regarding menses is considered taboo in her culture.
In patients with OHVIRA, it is essential to drain the hematocolpos for symptomatic treatment. Hence, resection should be performed on the vaginal septum. Patients may experience vaginal restenosis during follow-up. Communication between the right and left vagina should be established to relieve obstruction and allow the accumulated menses to outflow. However, the rate of conceiving post-resection remains high (around 87%). 7
Conclusion
In short, adolescents with persistent offensive vaginal discharge at menarche require a comprehensive workup to exclude rare causes such as urogenital-congenital anomalies. A thorough history taking coupled with the help of diagnostic imaging may contribute to an early diagnosis of the disorder.
Footnotes
Author contributions
Concepts and design: ANR, TV wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.