
Abstract
Background
We have reported that age-specific incidence rates of breast cancer among Japanese women increased from 2005 to 2015 in a bimodal distribution pattern, with two peaks in the pre- and postmenopausal age groups.
Objectives
The present study aimed to assess the associations of the increasing age-specific breast cancer incidence or mortality with the prevalence of obesity and drinking and smoking habits, compared with those in uterine body, female and male colon and lung cancers.
Methods
Linear correlations of annual rates from 2005 to 2015 of the 10-year age-specific cancer incidence and mortality with the prevalence of obesity (body mass index, 25 and over) and drinking (alcohol, 20 g and over 3 times or more a week) and smoking habits were assessed by Pearson’s correlation coefficients during the same 10-year period (from 2005 to 2015) or the 10-year period 10 years before the cancer incidence and mortality were noted (from 1995 to 2005).
Results
Positive correlations (r>0.640) were found between the increasing breast cancer incidence and the drinking habit during the same period or the smoking habit during the period 10 years before. Similar but weaker correlations were found for the breast cancer mortality rate increasing with age. Positive correlations were found between the decreasing male lung cancer mortality rate and the smoking habit rate during the period 10 years before.
Conclusions
The present ecological study indicated that the breast cancer incidence was associated with the current drinking habits and the past smoking habits among Japanese women.
Introduction
We have reported that age-specific incidence rates of breast cancer among Japanese women increased from 2005 to 2015 in a bimodal distribution pattern, with two peaks in the age groups of 45–49 and 60–64 years (pre- and postmenopausal age groups). 1 Such a recent increase indicates some modifiable factors to develop breast cancer, which may be regarded as westernized lifestyle factors. The impact of westernized lifestyle was also demonstrated by a migration study from Japan to Hawaii between 1969 and 1997, being more obvious for colon cancer both in Japanese men and women. 2 The increase in colon cancer incidence has been stagnant since 2005. 1 Apart from genetic risk factors, modifiable environmental risk factors for estrogen-related breast cancer such as obesity, alcohol drinking and cigarette smoking, besides reproductive factors, have been evaluated in Japan. 3 The obesity prevalence was not correlated with the breast cancer incidence among Japanese women. 1
The present study aimed to assess associations of the recent increase in breast cancer incidence with the prevalence of obesity and drinking and smoking habits among age-stratified Japanese women, as an ecological study using the national data of Japan. The incidence and mortality rates of breast cancer were compared with those of colon cancer, uterine body cancer related to estrogen, 4 and lung cancer that is known to be obviously affected by cigarette smoking. 5
Methods
Age-specific incidence and mortality rates (per 100,000 population in each 5-year age group) of breast, uterine body, colon and lung cancers among Japanese women and those of colon and lung cancers among Japanese men in 2005 through 2015 were obtained from national data published by Cancer Information Services, National Cancer Center, Japan (http://gdb.ganjoho.jp/graph_db/). Age-specific rates (% in each 10-year age group) of obesity (body mass index, 25 and over), drinking habits (alcohol, 20 g and over 3 times or more a week), and smoking habits in 1995 through 2015 were obtained from national data published by National Institute of Health and Nutrition, Ministry of Health, Labour and Welfare, Japan (https://www.mhlw.go.jp/bunya/kenkou/kenkou_eiyou_chousa.html). The national survey on drinking habits in 2013 was not performed.
Age-specific incidence and mortality rates of breast, uterine body, colon and lung cancers were re-calculated from per 100,000 population in each 5-year age group to per 100,000 population in each 10-year age group, because data of age-specific rates for obesity prevalence, drinking habits and smoking habits were published in each 10-year age group. Linear correlations of the 10-year age specific incidence or mortality rates of each cancer in 2005 through 2015 with the 10-year age-specific rates of obesity prevalence, drinking habits and smoking habits were assessed during the same 10-year period or the 10-year period 10 years before the cancer incidence and mortality were noted.
Statistical analysis
The linear correlations between the age-specific cancer incidence or mortality rates and the age-specific rates of obesity prevalence, drinking habit or smoking habit in each 10-year age group were assessed by Pearson’s correlation coefficients, using 11 pair data (n = 11), except for the drinking habit rate in 2005 through 2015 (10 pair data, n = 10). All tests were two-tailed, and statistical significance was set at p < 0.05.
Results
Figure 1 shows the age-specific incidence and mortality rates of breast cancer and uterine body cancer in each 5-year age group in 2005, 2010 and 2015. The age-specific incidence rates of breast cancer clearly increased during the 10-year period in a bimodal distribution pattern with two peaks in the age groups of 45–49 and 60–64 years. The incidence rates of uterine body cancer were lower than those of breast cancer, but still increased during the same period in a bell-shaped pattern, with a single peak in the age group of 55–59 years. The mortality rates of both breast and uterine body cancers rather increased with age, and moderately increased from 2005 to 2015. The age-specific incidence and mortality rates of female and male colon cancers are shown in Figure 2, and those of lung cancers are shown in Figure 3. The incidence and mortality rates of both colon and lung cancers increased with age like common age-related cancers. The incidence rates of female and male colon cancers and female lung cancer slightly increased from 2005 to 2015. The mortality rates of female and male colon cancers and female lung cancer did not change from 2005 to 2015. The incidence and mortality rates of male lung cancer began to decrease during 2005 through 2015. Age-specific incidence and mortality rates of breast cancer and uterine body cancer in 2005, 2010 and 2015 in Japan. Age-specific incidence and mortality rates of female colon cancer and male colon cancer in 2005, 2010 and 2015 in Japan. Age-specific incidence and mortality rates of female lung cancer and male lung cancer in 2005, 2010 and 2015 in Japan.


Figure 4 shows annual changes from 1995 to 2015 in the age-specific rates of female and male obesity prevalence, drinking habits and smoking habits in each 10-year age group. Data on drinking habits in 2013 were lacking due to no survey. The obesity prevalence rates in all the age groups, but the age group of 20–29 years, tended to decrease during 1995 through 2015 in women, while those in all the age groups tended to increase during the same period in men. The obesity prevalence rates of the age groups of 20–29 and 30–39 years in women were as low as less than 16% throughout the period. The drinking and smoking habit rates in women were much less than those in males. The drinking habit rates in the age groups of 40–49 and 50–59 years in women tended to increase during 1995 through 2015, and those in the age groups of 20–29 and 30–39 in women tended to increase during 1995 through 2005. The smoking habit rates in the age groups of 20–29, 30 to 39, 40 to 49 and 50–59 years in women tended to increase during 1995 through 2005. The drinking and smoking habit rates in all the age groups in men continued to decrease during 1995 through 2015. Female and male age-specific obesity prevalence, drinking habit and smoking habit rates during 1995 through 2015 in Japan.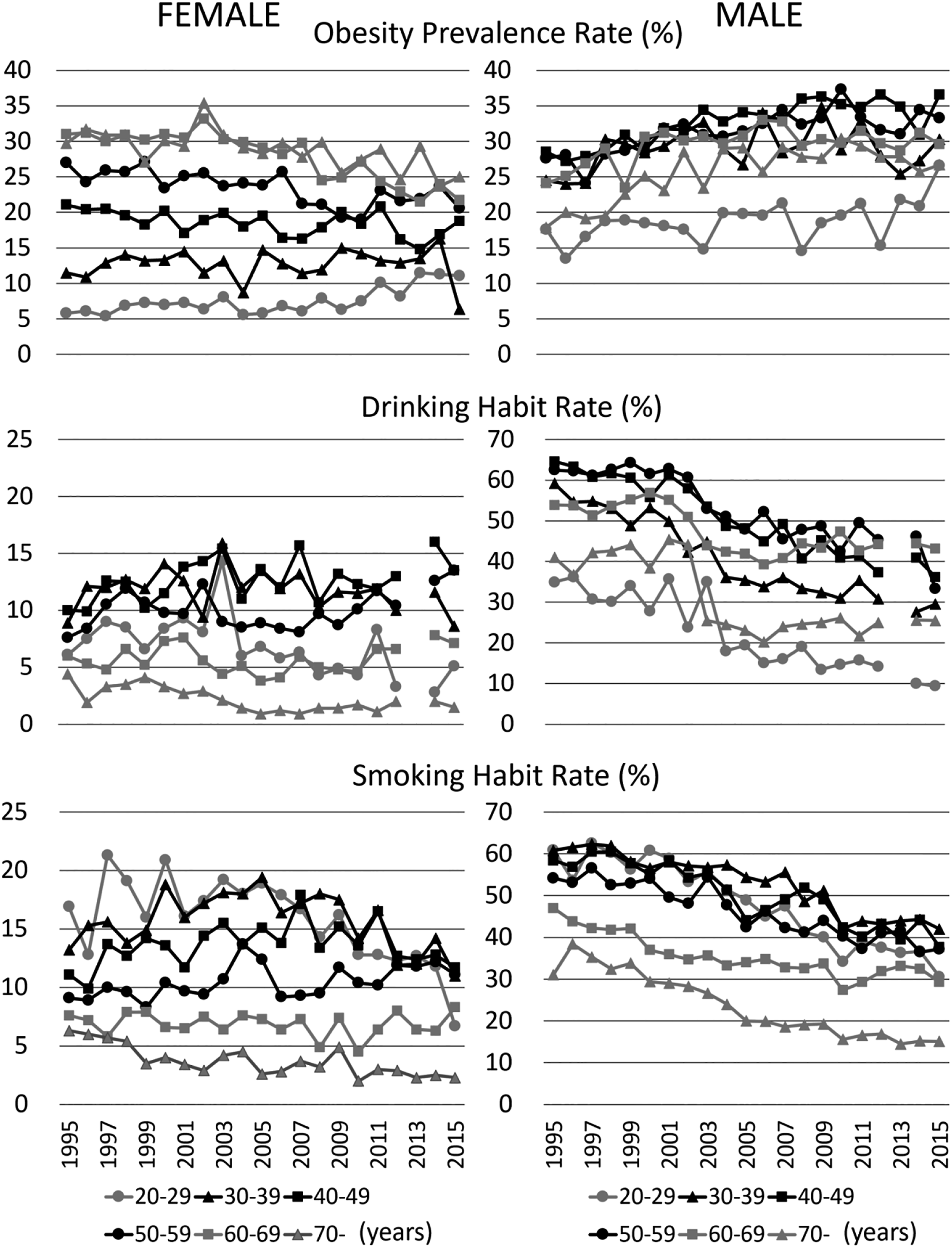
Correlation coefficients between the age-specific breast cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005–2015) or the period 10 years before (1995–2005).
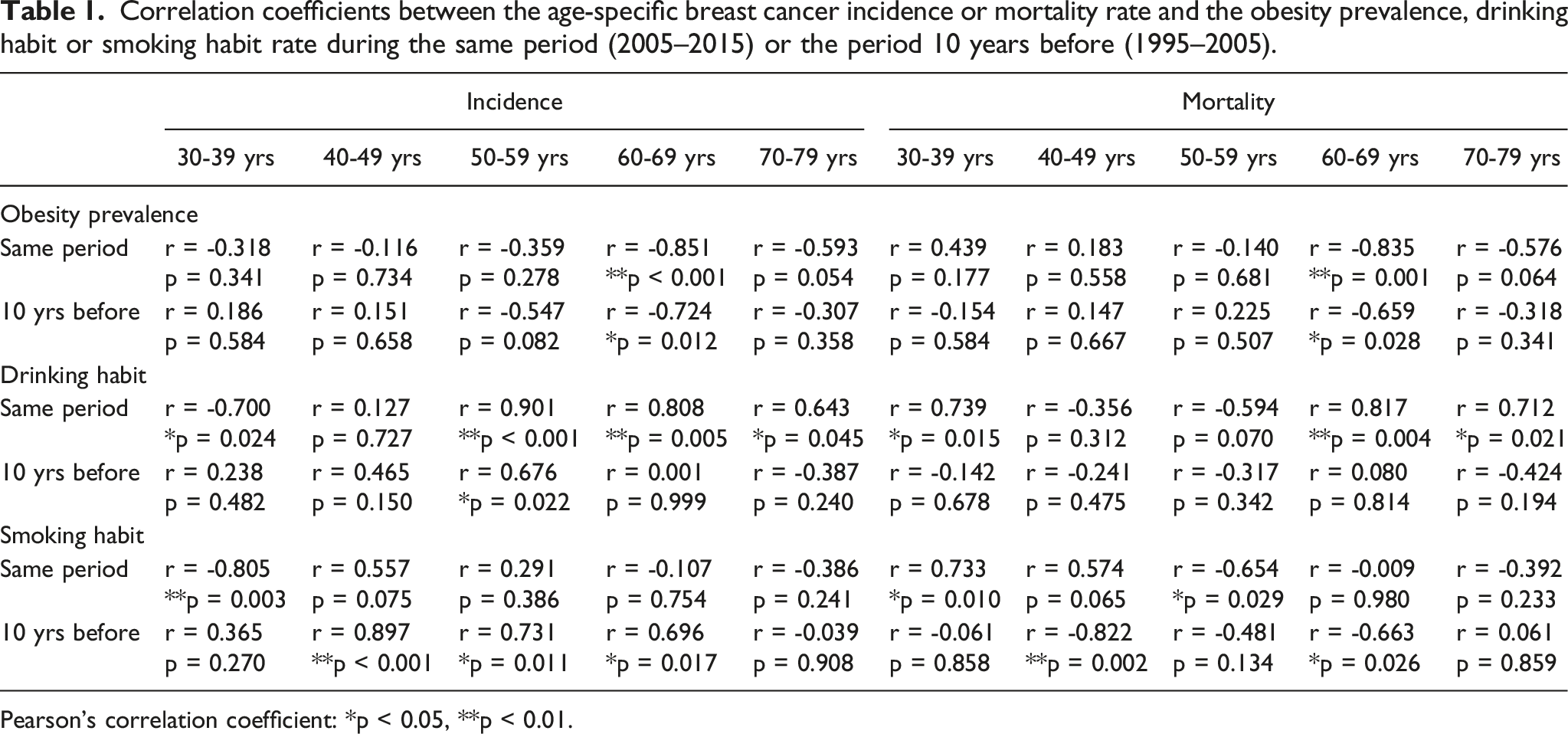
Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Correlation coefficients between the age-specific uterine body cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005 to 2015) or the period 10 years before (1995 to 2005).
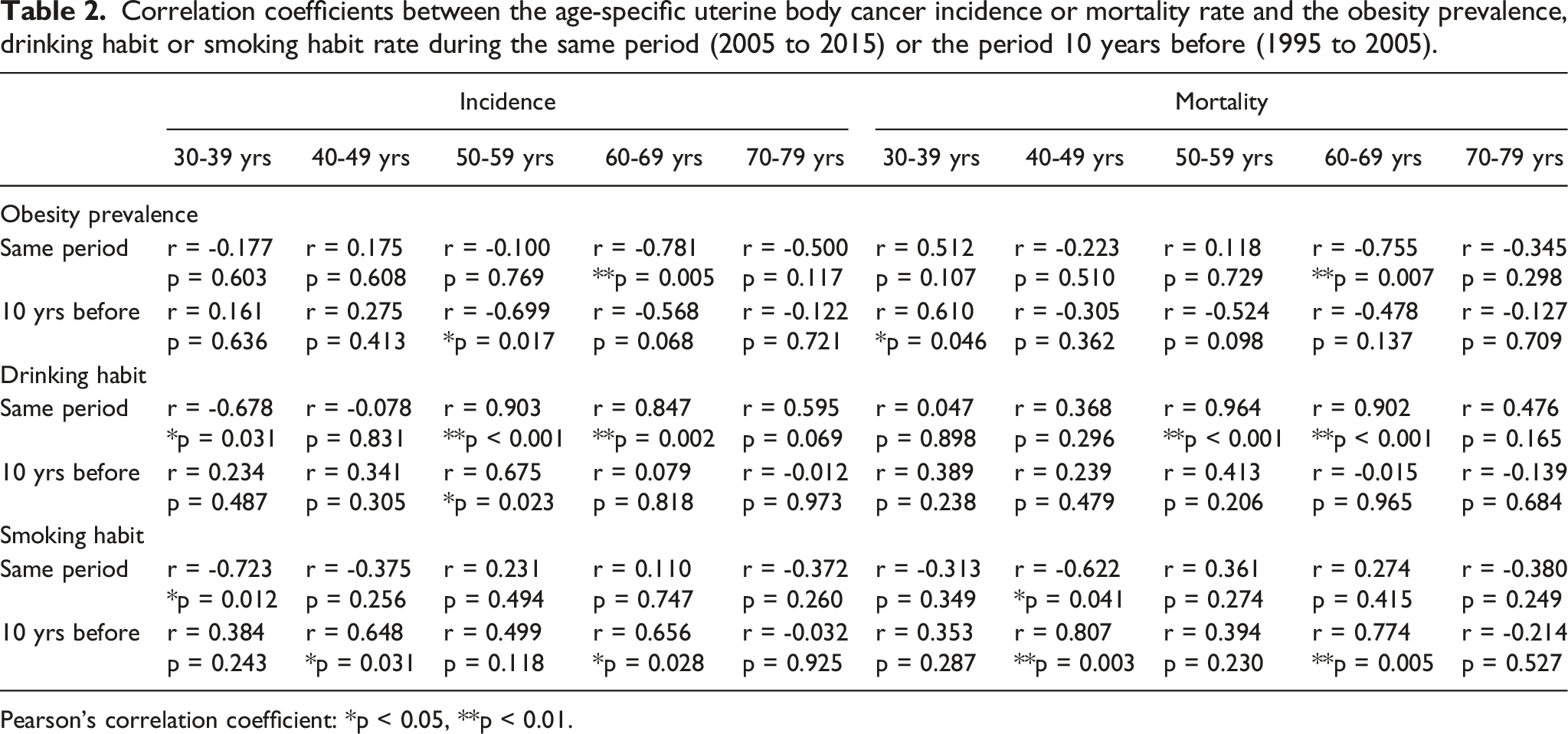
Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Correlation coefficients between the age-specific female colon cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005 to 2015) or the period 10 years before (1995 to 2005).

Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Correlation coefficients between the age-specific male colon cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005 to 2015) or the period 10 years before (1995 to 2005).

Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Correlation coefficients between the age-specific female lung cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005 to 2015) or the period 10 years before (1995 to 2005).

Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Correlation coefficients between the age-specific male lung cancer incidence or mortality rate and the obesity prevalence, drinking habit or smoking habit rate during the same period (2005 to 2015) or the period 10 years before (1995 to 2005).

Pearson’s correlation coefficient: *p < 0.05, **p < 0.01.
Since changes in the age-specific incidence rates of breast, uterine body, colon and lung cancers among women during 2005–2015 were relatively easy to observe as shown in Figures 1–3, correlations among annual changes (n = 11) in those incidence rates (10-year age groups) were assessed in addition. Positive correlations were found between the breast cancer incidence and the uterine body cancer incidence in the age groups of 30–39 (r = 0.923, p < 0.001), 40 to 49 (r = 0.873, p < 0.001), 50 to59 (r = 0.935, p < 0.001), 60 to 69 (r = 0.928, p < 0.001) and 70 to 79 (r = 0.905, p < 0.001); between the breast cancer incidence and the colon cancer incidence in the age groups of 30–39 (r = 0.695, p < 0.05) and 70 to 79 (r = 0.952, p < 0.001); and between the breast cancer incidence and the lung cancer incidence in the groups of 30–39 (r = 0.709, p < 0.05), 50 to 59 (r = 0.674, p < 0.05), 60 to 69 (r = 0.901, p < 0.001) and 70 to 79 (r = 0.924, p < 0.001). Also, there were positive correlations between the uterine body cancer incidence and the colon cancer incidence in the age groups of 30–39 (r = 0.625, p < 0.05), 40 to 49 (r = 0.639, p < 0.05) and 70 to 79 (r = 0.894, p < 0.001); between the uterine body cancer incidence and the lung cancer incidence in the age groups of 50–59 (r = 0.686, p < 0.05), 60 to 69 (r = 0.944, p < 0.001) and 70 to 79 (r = 0.943, p < 0.001); and between the colon cancer incidence and the lung cancer incidence in the age group of 70–79 (r = 0.902, p < 0.001).
Discussion
The present ecological study using the national data of Japan indicated that the age-specific breast cancer incidence rate correlated with the drinking habit rate during the same period from 2005 to 2015 and the smoking habit rate during the period 10 years before the breast cancer incidence was noted, that is, during the period from 1995 to 2005. These results would be interesting when mechanisms for the initiation, promotion, and progression of carcinogenesis in breast cancer are taken into consideration. Clinical and experimental studies have demonstrated that estrogen is involved in each phase of the carcinogenesis through complex mechanisms. 6 Concerning the modifiable cancer risk factors shown in the present study, blood estrogen levels can be elevated in postmenopausal women with obesity 7 and in pre- and postmenopausal women with drinking habits,8,9 but cannot be elevated in women with smoking habits. 10
The age-specific incidence and mortality rates of uterine body cancer, another estrogen-related cancer, also increased from 2005 to 2015, despite smaller rates compared with those of breast cancer. The age-specific incidence rate of uterine body cancer increased in a bell-shaped pattern, which was, interestingly, almost the same as that of breast cancer in 1980. 11 The mortality rates of breast cancer and uterine body cancer, which are thought to be affected by early cancer detection and advanced cancer treatments, 12 increased mainly among menopausal women. The colon cancer incidence rate has been presumed to be increased by westernized lifestyle factors,2,13 but such an increasing trend was stagnant during 2005 through 2015 among both women and men. The colon cancer mortality rates among both women and men remained stable after 2005. These changes contrasted to those of the breast cancer similarly affected by westernized lifestyle factors.1,2
During 2005 through 2015, the age-specific incidence rate of lung cancer among women slightly increased in a similar pattern to that of colon cancer. The lung cancer incidence and mortality rates among men and the mortality rate among women slightly decreased during 2005 through 2015, while the smoking habit rates among both women and men decreased during 1995 through 2015, except for the women during 1995 through 2005 in the age group of 20–59 years. Such decreases in lung cancer incidence are more obvious in the United States, where the incidence declined from 2009 to 2018 by almost 3% annually in men and 1% annually in women, according to smoking prevalence. 12 Cigarette smoke contains several thousand compounds, including at least 60 known carcinogens, which are highly correlated with the incidence of lung cancer. 14 The present study indicated that lung cancer incidence and mortality rates started to decrease with the continuing decrease in the smoking habit rate among Japanese men.
Regarding breast cancer, the present study demonstrated that the cancer incidence rate was associated with the current drinking habit rate among women in the age group of 50–79 years and the past smoking habit rate among women in the age group of 40–69 years. In the literature concerning the breast cancer incidence among Japanese women, a population-based prospective cohort study from 1990 to 2003 found that alcohol consumption had no overall effect on breast cancer risk. 15 A multicenter case-control study conducted from 2005 to 2016 found that even light to moderate alcohol consumption was associated with breast cancer risk in Japan. 16 A pooled analysis of eight large-scale population-based prospective cohort studies has revealed that both high frequency alcohol consumption and consumption of large amounts of alcohol were associated with increased breast cancer risk in premenopausal but not postmenopausal women. 17 The consumption of alcohol beverages has been classified as carcinogenic to humans, 18 and possible mechanisms include oxidative stress, cell proliferation, effects on steroid hormones, and effects on one-carbon metabolism. 19
In respect to the smoking habit and breast cancer incidence, a systematic review with three cohort studies and eight case–control studies identified by a MEDLINE search from 1966 to 2005 concludes that tobacco smoking possibly increases the risk of breast cancer in the Japanese population. 20 A population-based prospective study conducted from 1990 to 1999 found that both active and passive smoking increased the risk of breast cancer in premenopausal but not postmenopausal women. 21 Another population-based prospective study conducted from 1992 to 2008 found that passive but not active smoking was associated with the risk of breast cancer, and that the increased risk was pronounced among women who did not habitually consume alcohol. 22 It is thus indicated that both drinking and smoking habits have additive or interactive effects on breast cancer incidence. Smoking during adolescence or early adulthood is suggested to increase later risk of breast cancer, when the rapidly developing breast is particularly susceptible to carcinogenesis. 23
Conclusions
The present ecological study indicated that the breast cancer incidence was associated with the current drinking habit and the past smoking habit among Japanese women. This finding would be interesting when mechanisms for the initiation, promotion, and progression of carcinogenesis in breast cancer are taken into consideration. Counseling on lifestyle modification should be beneficial for high-risk or young women to reduce the risk of developing breast cancer.
Footnotes
Authors’ contributions
YA conceived the research and wrote the manuscript. All authors (YA, AN, HB, YN) assessed data and researched the relevant literature. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Age-specific incidence and mortality rates of breast, uterine body, colon and lung cancers among Japanese women and those of colon and lung cancers among Japanese men in 2005 through 2015 can be obtained from Cancer Information Services, National Cancer Center, Japan (http://gdb.ganjoho.jp/graph_db/). Age-specific rates of body mass index and drinking or smoking habits in 1995 through 2015 can be obtained from National Institute of Health and Nutrition, Ministry of H2ealth, Labour and Welfare, Japan (![]() ).
).