
Abstract
Multiple primary malignant tumors of lung and colorectal incidence were extremely rare and in most cases, diagnosed incidentally. Due to its rarity, most physicians consider pulmonary lesions found in patients with a history of colorectal cancer as lung metastasis. To avoid misdiagnosis and treatment delays, it is critical to properly screen and explore for possible metastasis or the occurrence of a second primary tumor after a primary cancer has been diagnosed. We describe a 72-year-old woman who presented with rectal bleeding associated with altered bowel movement. Rectal biopsy revealed colon adenocarcinoma and subsequent CT scan showed sigmoid colon mass and right lower lobe lung mass with multiple mediastinal lymphadenopathies. Biopsies of the mediastinal lymph nodes also showed adenocarcinoma. PET/CT scans showed different SUVmax of lesions in the sigmoid colon and right lower lobe, which raised the possibility of separate colonic and lung primary tumors as opposed to colonic primary with lung metastasis. Further immunohistology studies confirmed separate primary lung tumor. These diagnoses facilitate the clinical approach and define treatment options for the patient.
Introduction
Multiple primary malignant tumors of lung and colorectal incidence were extremely rare 1 and in most cases, diagnosed incidentally. 2 Due to its rarity, most physicians consider pulmonary lesions found in patients with a history of colorectal cancer as lung metastasis. To avoid misdiagnosis, it is important to consider the possibility of a second primary tumor instead of a metastasis.
Case report
A 72-year-old woman presented with rectal bleeding associated with altered bowel movement. She also complained of anemic symptoms, lethargy and fatigue. Her past medical history include ischemic heart disease, diabetes mellitus, hypertension and dyslipidemia. Vitals were within normal limit and a suprapubic mass was felt on abdominal examination. Initial blood test showed hemoglobin count of 7.7 g/dL with microcytic hypochromic anemia picture. She received blood transfusion and subsequent colonoscopy revealed a sigmoid colon mass with contact bleeding 15 cm from the anal verge (Figure 1). Biopsies from this site revealed colon adenocarcinoma. Colonoscopic findings showed rectal mass with contact bleeding.
Subsequent CT staging showed a circumferential enhancing mass at the sigmoid colon with near total obliteration and splenic lesion suggestive of metastasis. In addition, there was a heterogeneously enhancing right lower lobe lung mass with multiple enhancing necrotic mediastinal lymphadenopathy suspicious of a concurrent primary lung mass with mediastinal metastases (Figure 2). Bronchoscopy examination revealed no endobronchial lesion and transbronchial needle aspiration (TBNA) guided by endoscopic ultrasound was performed on the mediastinal lymph nodes. The TBNA samples were examined via rapid on-site examination by pathologist to confirm the yield of the biopsied samples, of which showed malignant cells. CT scan findings; (A) Coronal view of thorax-abdomen-pelvis CT showed an enhancing lesion in the sigmoid colon measuring approximately 8 cm in length associated with surrounding fat streakiness (red arrow). (B) Axial view on lung window showed heterogenous lung mass seen at the medial basal segment of the right lower lobe. It measures approximately 4.3 × 2.8 × 6.0 cm (red arrow). The mass is seen in close proximity to the right lower lobe subsegmental bronchioles. (C) Axial view on mediastinal window at carina level showed multiple enhancing mediastinal lymphadenopathy at right and left paratracheal (red arrows). These lymph nodes enhanced with central hypodensity.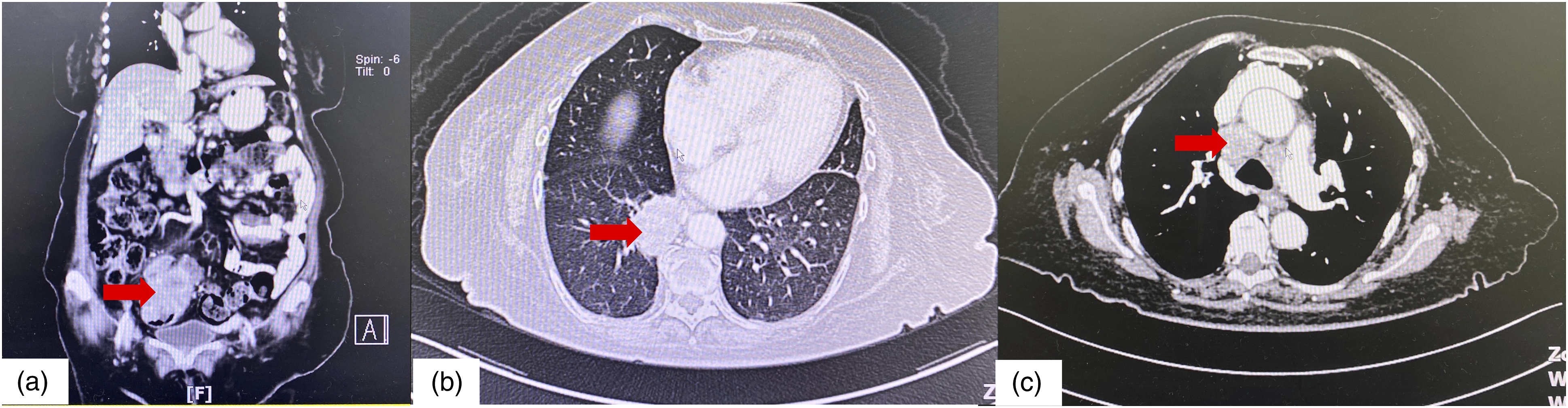
Full histology report of mediastinal lymph nodes showed primary lung adenocarcinoma with immunohistochemistry positive for CK7, TTF-1 and Napsin-A, and negative for CK20, CDX2, CK5/6, p40 and MUC2. Exon 18 G719X. Additional lung cancer panel analysis showed EGFR mutation (Exon 18 G719X) was detected. Rectal biopsy samples were re-examined and showed colon adenocarcinoma with tumor cells positive for CDX2, but negative for CK7 and TTF-1. These findings were consistent with a synchronous adenocarcinoma of lung and colon (Figure 3). (A) Cytology feature of the malignant cells seen in EBUS, with the large plemorphic malignant cells (*) and areas of necrosis (
A positron emission tomography (PET) scan showed hypermetabolic circumferential sigmoid colon mass measuring 8.1 × 7.0 × 6.7 cm (AP × W × CC) with SUVmax 29.6 and mesenteric nodal metastases largest measuring 1.9 × 1.5 cm with SUVmax 8.6, hypermetabolic lung mass at the medial basal segment of right lower lobe measuring 4.5 × 2.8 × 3.2 cm with SUVmax 6.8 and multiple hypermetabolic mediastinal, right hilar, and supraclavicular nodal metastases largest measuring 3.3 × 2.2 cm with SUVmax 6.1 (Figure 4). PET/CT scan findings. (A) Coronal view of PET-FDG showed a circumferential enhancing sigmoid colon mass measuring 8.1 × 7.0 × 6.7 cm (AP × W × CC) with SUVmax 29.6. (red arrow). (B) Axial view of PET-FDG showed hypermetabolic, heterogeneously enhancing lung lesion at the medial basal segment of right lower lobe measuring 4.5 × 2.8 × 3.2 cm (AP x W x CC) with SUVmax 6.8. (C) Axial view of PET-FDG showed multiple mediastinal lymph nodes with various uptake of SUVmax range 3.3 to 6.2 (red arrow).
Based on PET/CT scan and histology findings, diagnosis of a synchronous adenocarcinoma lung and colon was concluded in a multidisciplinary team consisting of respiratory, colorectal, pathology, and radiology teams. The final diagnosis was stage 3b lung cancer; right lower lobe mass with largest diameter 4.5 cm, supraclavicular nodal involvement and no distant metastasis (T2N3M0) and stage 2 colon cancer; involvement of serosa and absence of abdominal lymphadenopathy (T3N0M0). She was readmitted for recurrent rectal bleeding and subacute intestinal obstruction and was planned for colectomy. She developed hospital acquired pneumonia during the pre-operative admission for optimization for surgery and subsequently succumbed to her illness.
Discussion
Multiple primary malignant tumors (MPMTs) are defined as cancers arising from a different primary tumor which fulfil the following criteria: 3 (i) each tumor must be malignant, (ii) both tumors must have different histology, and (iii) metastasis must be ruled out. MPMT could be divided into synchronous or metachronous based on time intervals. The Surveillance Epidemiology and End Results (SEER) database recommended using a 2-month interval to distinguish between synchronous and metachronous multiple primaries, 4 whilst a 6-month interval was recommended by International Agency for Research on Cancer (IARC). 5 Based on these criteria, the present case was diagnosed as synchronous MPMTs of lung and colorectal.
MPMTs of lung and colorectal incidence were extremely rare (0.6%). 1 Furthermore the incidence of synchronous lung and colorectal cancer were much lower and in most cases, diagnosed incidentally , 2 as seen in the present case with the absence of any respiratory symptoms. Due to its rarity, most physicians consider pulmonary lesions that were found in patients with a history of colorectal cancer as lung metastases as it commonly develop in 10%–20% of patients with colorectal cancer. 6 Therefore, it is important to rule out synchronous tumors in suspicious lesions that could be metastasis, as failure to do so may lead to misdiagnosis and delay in treatment.
Demographically, synchronous MPMTs lung and colorectal cancer were commonly observed among elderly patients (range age 60–86 years) and those who smoke >30-pack-year. 2 Radiologically in computed tomography (CT) findings, single solitary lung nodule and presence of mediastinal lymph node enlargement in the setting of elderly patients or patient with a history of smoking were more likely to be primary lung cancer. 7 These findings concurred with our patient; suspicious CT findings of lung mass with multiple lymphadenopathies despite the absence of smoking history. In addition, FDG-PET/CT was shown to be superior to conventional work-up that include CT findings in the detection of synchronous tumors during primary staging. 8 Standardized uptake values (SUVs) on FDG-PET images can be used to distinguish between a metastatic lesion and a primary tumor. On an FDG-PET images, a metastatic lesion will have SUVs that are identical to the primary tumor. Therefore large differences in SUVs on FDG-PET images between two tumors of the same organ origin or tumors of a different organ could suggest the presence of a second primary tumour. 9 In the present case; a sigmoid colon mass with SUVmax 29.6 which was higher compared to a right lower lobe mass with SUVmax 6.8, was indicative of possible separate primaries.
To confirm this diagnosis, a histological examination is required. Furthermore, in cases with synchronous tumors with the same histology; which in this case adenocarcinoma subtypes in both colon and lung samples, immunohistochemical staining testing is useful which include CK7, CK20, TTF-1 and Napsin-A to confirm and exclude primary lung cancer. Primary lung cancer shows a CK7(+)/CK20(−) 10 pattern, positive TTF-1 11 and Napsin-A, 12 while a metastatic adenocarcinoma shows a CK7(−)/CK20(+) pattern, negative TTF-1 and Napsin-A. In addition, the biopsied samples in this case were examined and compared by the same pathologist with extensive immunohistochemical staining testing; mediastinal lymph node biopsies were positive for CK7, TTF-1 and Napsin-A, and negative for CK20, CDX2, CK5/6, p40 and MUC2, whereas rectal biopsies were positive for CDX2, but negative for CK7 and TTF-1. These findings confirmed a synchronous MPMTs of lung and colon adenocarcinoma.
A possibility of metastasis from the lung (mucinous type) to the colon is also considered despite the lack of mucinous features in the cytology of the primary lung tumor as well as the immunohistochemistry panels (Napsin-A and TTF-1). GIT metastasis of primary lung carcinoma is rare 13 and involvement of the colon have been reported but none specify a primary mucinous type. HNF4α expression in a tissue microarray have been used to specify primary mucinous lung cancer but no data of usage in secondary to GIT cases.
Treatment options for patients with synchronous colorectal and lung cancer is different from that of colorectal cancer patients with pulmonary metastasis. The former patients would benefit from synchronous curative resection of the two lesions as the first choice if the condition of the patient permits. For the latter, the first choice of treatment is chemotherapy or other palliative therapy. For our patient, she was diagnosed with advanced tumors; stage 3b lung cancer and stage 2 colon cancer. Therefore, any intervention at this juncture would be directed to colon cancer as patient was symptomatic from this tumor. She was planned for surgical resection to alleviate bowel obstruction with possibility of adjunct palliative chemotherapy. A combination of a 3-week/cycle regimen with paclitaxel (175 mg/m2) and oxaliplatin (100 mg/m2) on day 1 with a total of six cycles was used in synchronous adenocarcinoma lung and colorectal cancer. 14 Unfortunately, our patient succumbed prior to the intended treatments.
Conclusion
The chances of having a synchronous tumor with the same histological background are extremely rare. To avoid misdiagnosis and treatment delays, it is critical to properly screen and explore for possible metastasis or the occurrence of a second primary tumor after a primary cancer has been diagnosed. This will aid in the development of a good clinical approach for the patient and definite treatment options.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.