
Abstract
Objective
To describe the functional outcomes of post COVID-19 patients after inpatient rehabilitation and determine if patients who underwent adjunct daily robotic therapy with Andago had better functional outcomes than those who did not and if patients who were frail had worse functional outcomes than those who were pre-frail or not frail.
Design
Retrospective study of COVID-19 patients transferred for acute inpatient rehabilitation from 1 November 2021 to 31 December 2021.
Results
Post COVID-19 patients who underwent inpatient rehabilitation had an improvement in the Functional Independence Measure (FIM) (median 109 vs 82), Functional Ambulation Category(FAC) (median 3 vs 2), distance walked with physiotherapist (mean 143.5 vs 18.7 m), and the Hospital Anxiety and Depression Scale(HADS) (mean 4.5 vs 7.8) from baseline. Robotic therapy may be associated with a shorter rehabilitation medicine length of stay (median 13 vs 19.5 days) and a higher FIM efficiency (mean 2.3 vs 1.2). Patients with a higher frailty score may have a slower 10 Meter Walk Test (10MWT) speed at discharge (Spearman’s rho −0.542).
Conclusion
Post COVID-19 patients benefit from inpatient rehabilitation with a comprehensive rehabilitation program, and adjunct robotic therapy may be offered to further improve functional outcomes. Frailty may also be considered when establishing rehabilitation goals, as meaningful functional gains can still be achieved.
Introduction
Coronavirus disease 2019 (COVID-19) has become a global pandemic, with over 500 million confirmed cases globally in May 2022. 1 Singapore was not spared and confirmed its first imported case in January 2020. 2 The setting up of a multi-ministry task force and tight social restrictions were able to keep numbers low initially; 3 however, subsequent outbreaks resulted in a surge in local cases, mainly in migrant worker dormitories, from April to June 2020. 4 The affected population was relatively young, and most of them did not have severe disease. The healthcare system was stretched once again when the Delta variant cases peaked in October 2021 5 with more patients having severe disease requiring critical care and post COVID-19 sequelae impacting their mobility and function. As of May 2022, Singapore has reported over 1.2 million cases. 6
Studies have suggested that patients with COVID-19 can benefit from rehabilitation.7,8 The identification of areas of need includes pulmonary rehabilitation, neuromuscular rehabilitation, and strategies to cope with psychological distress. 9 In the first year of the COVID-19 outbreak, our acute inpatient rehabilitation unit had the opportunity to trial a robotic device for pulmonary rehabilitation of a post-ICU COVID-19 patient. 10 During the delta wave, we extended the use of the robotic device to include more patients. To our knowledge, there is limited data on the benefits of robotic therapy for the rehabilitation of COVID-19 patients. 11
Studies have also been published on the effects of frailty on outcomes, particularly mortality,12,13 disease severity, and length of stay; 14 however, there is no published data on the impact of frailty on functional outcomes in COVID-19 patients.
In this study, we describe the functional outcomes of COVID-19 patients after inpatient rehabilitation. We aimed to determine whether patients who underwent robotic therapy with Andago had better functional outcomes than those who did not and if patients who were frail had worse functional outcomes than those who were pre-frail or not frail.
Methods
This was a retrospective medical record review of COVID-19 patients transferred for acute inpatient rehabilitation from 1 November 2021 to 31 December 2021. Ethics deliberation was exempted as this study utilized de-identified patient data. CIRB 2022/2075. The inclusion criteria were a diagnosis of COVID-19 based on a positive PCR test and the presence of impairments as a direct result of COVID-19 or its complications.
Patients with COVID-19 as an incidental finding on screening were excluded.
The data collected included demographics, such as age, sex, and premorbid function. Clinical information included the Charlson comorbidity index, frailty score 15 on transfer, admission to the ICU or high-dependency unit, method of oxygenation ICU/HDU, oxygen requirement on transfer to the rehabilitation unit, mental health scores, and discharge destination. The functional data collected included the Functional Independence Measure (FIM) score, Functional Ambulation Category (FAC) score, Hospital Anxiety and Depression Scale (HADS), 10 Meter Walk Test (10 MWT), number of physiotherapy sessions, distance ambulated with a physiotherapist, rehabilitation, and total length of stay.
The Functional Independence Measure (FIM) is a widely used general measure of disability consisting of 18 items with scores ranging from one (total dependence) to seven (total independence) for each item. It measures motor function, cognition, and self-care ability. The derivatives of FIM scores include FIM gain and FIM efficiency. FIM gain is the difference between the discharge and admission FIM and measures the absolute functional gain. FIM efficiency is the FIM gain divided by the length of stay in rehabilitation, and it measures the rate of functional improvement.
Functional Ambulation Categories (FAC) is a 6-point functional walking test that evaluates ambulation ability, determining how much human support the patient requires when walking, regardless of whether they use a personal assistive device. The Hospital Anxiety and Depression Scale (HADS) includes 14 questions (seven for anxiety and seven for depression) on a scale of 0–3 for each question, with higher values indicating a greater likelihood of anxiety or depression.
Fried’s frailty phenotype was used to assess frailty after transfer. The following five physical features were assessed: unintentional weight loss, weakness(low grip strength), exhaustion, slow walking speed, and low physical activity. Frailty is present when three of these features are present and pre-frail when 1–2 features are present. 16
Patients were screened for suitability for robotic therapy on transfer to the rehabilitation unit. Andago is a robotic device with a partial body-weight-supported suspension system that allows over-the-ground walking at a patient-selected speed. Robotic therapy was administered daily, including on weekends, as an adjunct to conventional pulmonary rehabilitation. The patients were supplemented with weight support of 2.5–5 kg bilaterally with a minimum weight support of 2.5 kg. Each robotic session lasted 30 min, during which the patient underwent gait training and was allowed to ambulate as much as possible if vital signs such as blood pressure and oxygen saturation were within the limits of safety. This is in addition to the standard therapy available 5 days a week.
Patients who had COVID-19 and were transferred to the inpatient rehabilitation unit were already deisolated from the COVID-19 ward. The criteria for the suitability of robotic therapy were as follows: 1. No episodes of desaturation within 48 hours or stable resting oxygen requirements 2. Agreement from the primary team for ambulation 3. No history of osteoporosis 4. Ability to weight-bear 5. No active joint or muscle pain 6. Manual Muscle testing (MMT) of ≥4 for ambulation 7. Ability to stand supported for 30–45 s for the security harness to be put on. 8. Does not need isolation or contact precautions
All post COVID-19 patients underwent daily physiotherapy, occupational therapy, and speech therapy on a 5 days a week basis. Pulmonary rehabilitation was conducted in 30–45 min sessions 1–2 times a day, depending on the patients’ tolerance so as to reduce dyspneic symptoms, increase muscle utilization, and teach techniques to cope with activities of daily living. Depending on the severity of symptoms, chest physiotherapy may be in the form of deep breathing exercises with or without the use of an incentive spirometer, inspiratory muscle training with recruitment of abdominal muscles, and active cycles of breathing techniques. Muscle strengthening exercises were implemented for deconditioned patients with notable muscle wasting to improve their efficiency and utilization. Oxygen saturation and cardiovascular parameters were monitored continuously during therapy, and oxygen via nasal prongs may be supplemented depending on tachycardia, desaturation, or patient symptoms during exertion with the intent to wean during the course of the rehabilitation stay. Nutrition was optimized with dietitian consultation to ensure adequate caloric and protein intake. Patients were also monitored for mood and anxiety symptoms and referred to a mental health therapist for emotional support if deemed appropriate by the primary team.
Statistical analysis
Descriptive statistics of demographic, clinical, and functional outcome variables are reported as numbers and percentages for categorical data, mean ± standard deviation (SD) for continuous or quasi-interval data, and median and interquartile range (IQR) for discrete data.
To assess whether functional outcomes improved after rehabilitation, we used the paired samples t-test for continuous or quasi-interval outcomes and the Wilcoxon signed-rank test for discrete outcomes. To assess whether there was a relationship between robotic therapy and baseline characteristics/functional outcomes, we used Welch’s t-test for continuous or quasi-interval outcomes, the Mann-Whitney U test for discrete outcomes, and Fisher’s exact test for categorical outcomes. The relationship between the frailty score and functional outcomes was assessed using Spearman’s rho. Because this was an exploratory study with a small sample size, we did not adjust for multiple comparisons. A p-value below the two-sided significance level of 0.05 was taken to suggest the possibility of an association.
All statistical analyses were conducted using Stata 15.0 (College Station, TX, StataCorp LLC).
Ethics clearance
This study was exempt from review by the Institutional Research Review Board, as it is a retrospective review involving de-identified data (CIRB 2022/2075).
Results
The total number of patients screened was 14. One patient did not qualify for the study as he sustained a spinal cord injury after a fall while at a community isolation facility. Thirteen patients qualified for robotic therapy. Nine patients underwent robotic therapy, while four did not. Among the four patients, two declined, one required contact precautions (nursed in a separate cubicle in the ward and segregated from other patients during therapy), and one patient was in a separate rehabilitation ward without access to Andago, as the patients and staff were segregated based on location at the height of the pandemic. The average number of sessions of robotic therapy that was applied was 10.4.
Characteristics of patients.

†4 patients had missing oxygenation data. A&E = Accident and Emergency. H-score = Highest score. HDU = High Dependency Unit. HFNC = High Flow Nasal Cannula. ICU = Intensive Care Unit. RHM = Rehabilitation Medicine. RPE = Borg Rating of Perceived Exertion. SACH = St. Andrew’s Community Hospital.
aMann-Whitney U test was used for discrete outcomes, and Fisher’s exact test for categorical outcomes.
Functional outcomes of patients at discharge vs. at admission
Change in functional outcomes of patients at discharge compared to admission.

aThe paired t-test was used for continuous or quasi-interval outcomes, while the Wilcoxon signed-rank test was used for discrete outcomes. †5 patients were unable to perform the 10MWT at admission. Change in 10MWT speed was estimated using available data from eight patients. 10MWT = 10 Meter Walk Test. FAC = Functional Ambulation Category. FIM = Functional Independence Measure. HADS = Hospital Anxiety Depression Scale. RHM = Rehabilitation Medicine.
Functional outcomes of patients with vs. without robotic therapy
Functional outcomes of patients with and without robotic therapy.
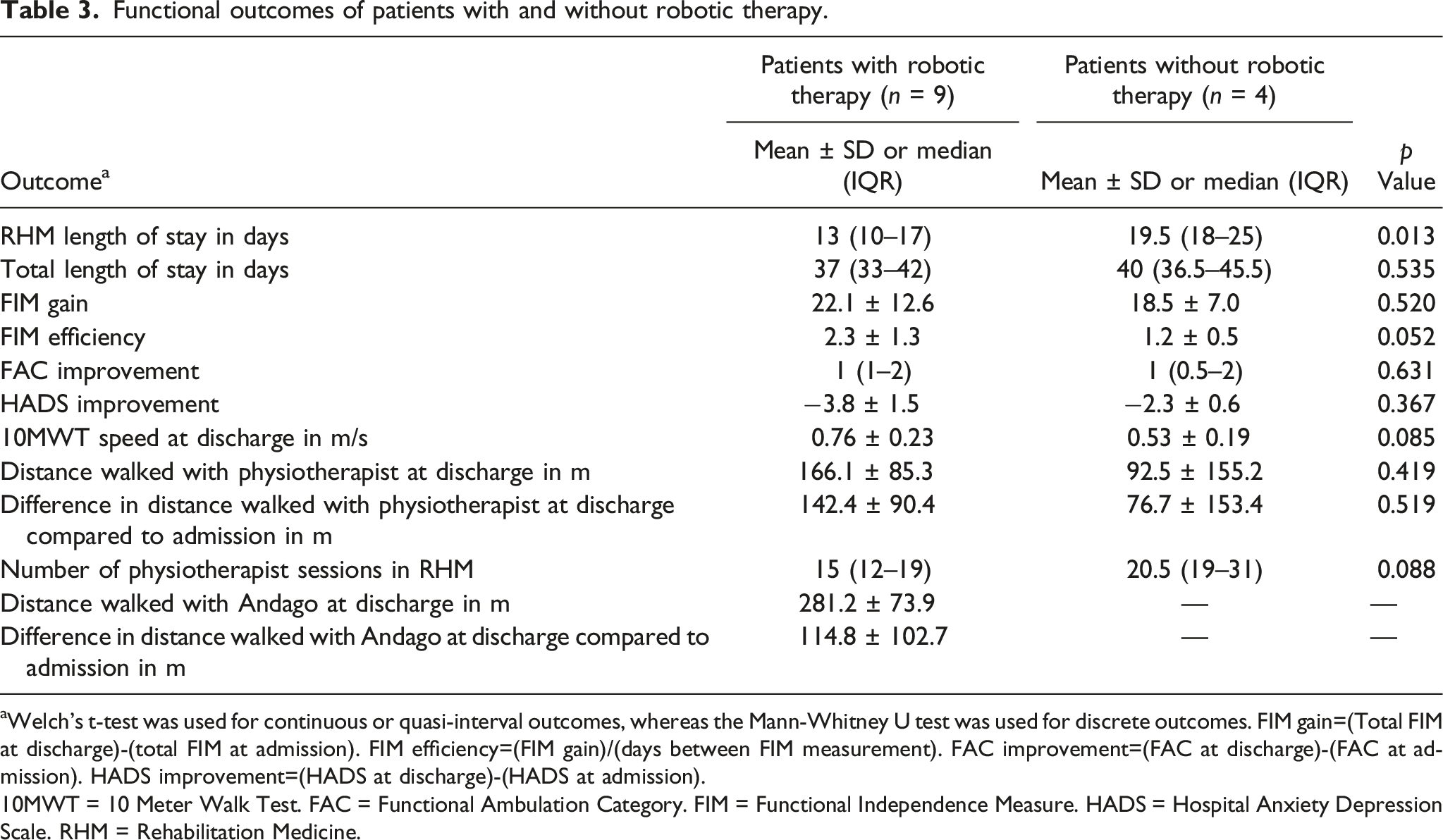
aWelch’s t-test was used for continuous or quasi-interval outcomes, whereas the Mann-Whitney U test was used for discrete outcomes. FIM gain=(Total FIM at discharge)-(total FIM at admission). FIM efficiency=(FIM gain)/(days between FIM measurement). FAC improvement=(FAC at discharge)-(FAC at admission). HADS improvement=(HADS at discharge)-(HADS at admission). 10MWT = 10 Meter Walk Test. FAC = Functional Ambulation Category. FIM = Functional Independence Measure. HADS = Hospital Anxiety Depression Scale. RHM = Rehabilitation Medicine.
It may also be associated with faster walking speed on the 10 MWT speed (mean 0.76 vs 0.53 m/s) at discharge, and a smaller number (median 15 vs 20.5) of physiotherapy sessions in rehabilitation medicine (Table 3) although these were not statistically significant.
Functional outcomes of patients who were frail vs. those who were pre-frail or not frail
Functional outcomes of patients with increasing frailty score.
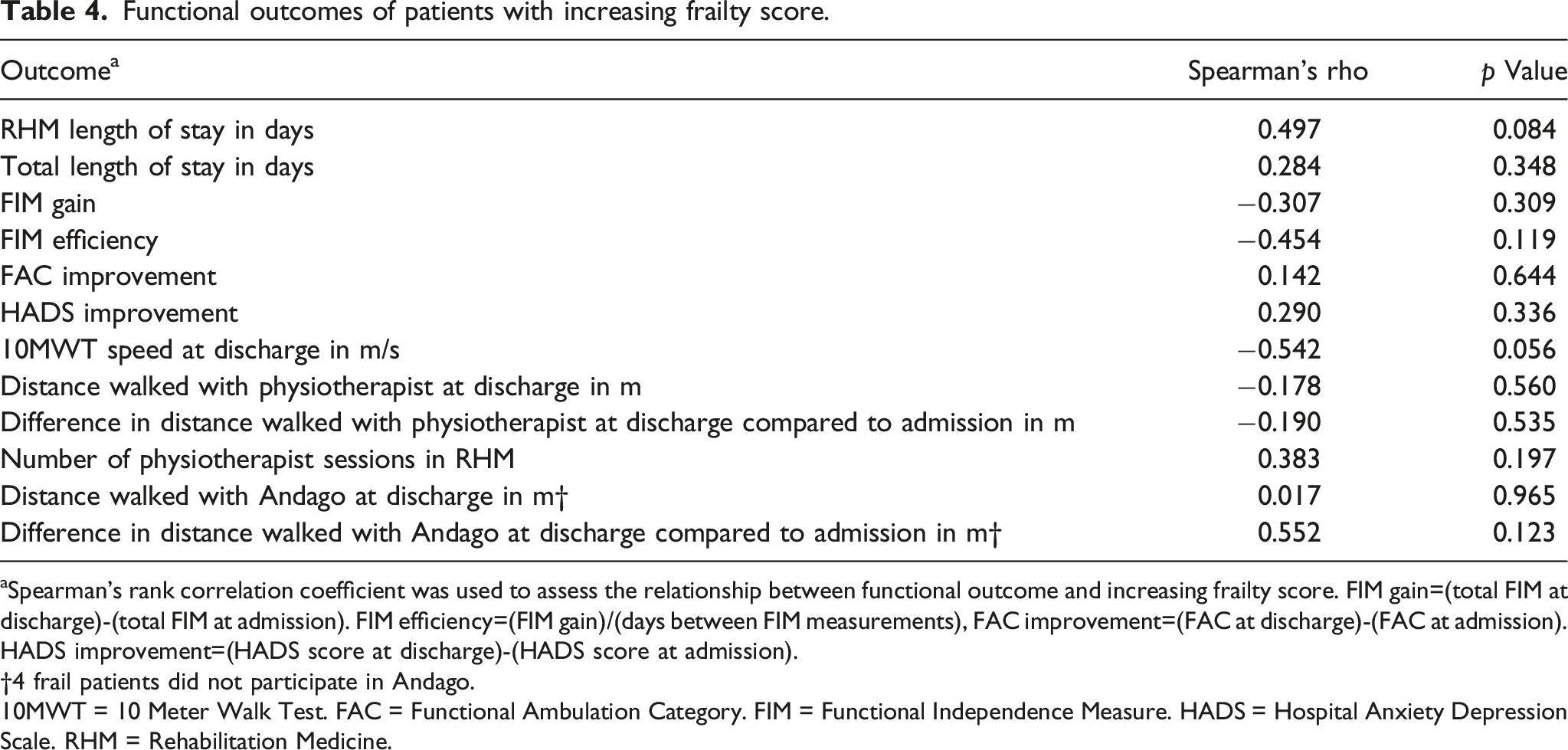
aSpearman’s rank correlation coefficient was used to assess the relationship between functional outcome and increasing frailty score. FIM gain=(total FIM at discharge)-(total FIM at admission). FIM efficiency=(FIM gain)/(days between FIM measurements), FAC improvement=(FAC at discharge)-(FAC at admission). HADS improvement=(HADS score at discharge)-(HADS score at admission). †4 frail patients did not participate in Andago.10MWT = 10 Meter Walk Test. FAC = Functional Ambulation Category. FIM = Functional Independence Measure. HADS = Hospital Anxiety Depression Scale. RHM = Rehabilitation Medicine.
Patient-specific characteristics and outcomes.
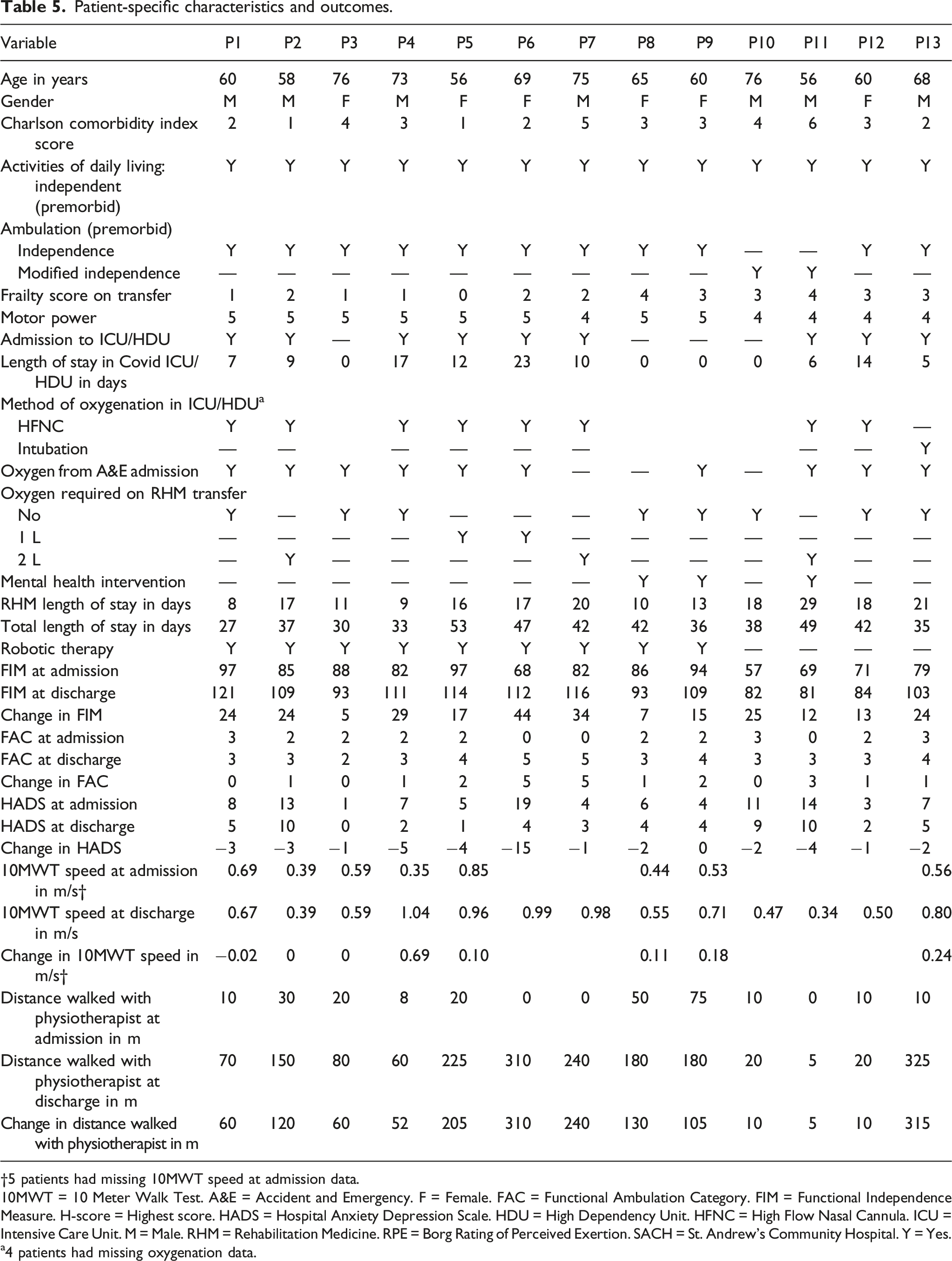
†5 patients had missing 10MWT speed at admission data. 10MWT = 10 Meter Walk Test. A&E = Accident and Emergency. F = Female. FAC = Functional Ambulation Category. FIM = Functional Independence Measure. H-score = Highest score. HADS = Hospital Anxiety Depression Scale. HDU = High Dependency Unit. HFNC = High Flow Nasal Cannula. ICU = Intensive Care Unit. M = Male. RHM = Rehabilitation Medicine. RPE = Borg Rating of Perceived Exertion. SACH = St. Andrew’s Community Hospital. Y = Yes.
a4 patients had missing oxygenation data.
Discussion
Our findings concur with those of previous studies demonstrating the benefits of rehabilitation after COVID-19.7,8 Significant improvements in functional outcome measures and mood symptoms were noted in the overall cohort, reiterating the role of acute inpatient rehabilitation after COVID-19.
Patients recovering from COVID-19 infection may have oxygen desaturation on exertion, 9 and those with early or severe desaturation may further decondition if physiotherapists are not able to mobilize them as such. Based on previous experience with the application of robotic therapy in patients with restrictive lung disease 17 and post-critical care COVID-19 patient, 10 we applied the same treatment to all post COVID-19 patients who were transferred to the inpatient rehabilitation unit and were willing and suitable. The principle was to provide off-loading of body weight, increase support and confidence, provide supplemental oxygen as needed, reduce the physical burden on the therapist, and enable the patient to walk a further distance than they could overground without the device. In doing so, it builds up neuromuscular endurance and possibly lower extremity strength. There were trends towards faster gait speed on the 10 MWT on discharge, greater distance ambulated with the physiotherapist on discharge, and greater improvement in the distance ambulated with the physiotherapist, although these have not yet reached statistical significance. There was also greater FIM efficiency approaching statistical significance, as well as a shorter rehabilitation length of stay of 6.5 days which is statistically significant. In general, those who received robotic therapy had fewer sessions of physiotherapy, which may be attributed to a shorter length of hospital stay and robotic therapy over the weekends. Gait outcome measures are yet to reach statistical significance, and this could be due to the small sample size. Robotic therapy is safe when the appropriate selection criteria are applied.
Patients who were frail, compared with those who were not frail or only pre-frail had lower FIM efficiency and a lower discharge walking speed on the 10 MWT, which approached statistical significance. Regardless of the presence of frailty, patients had improvements in FIM, distance ambulated with physiotherapists, and HADS scores. The improvements in HADS reached a minimal clinically important difference18–20 in both groups.
However, from the baseline data (Table 1), it was found that patients who did not receive RT were frailer. This may account for the increased length of stay, reduced FIM efficiency, and poorer 10MWT, rather than solely because of the lack of robotic therapy. Patients who are frailer may have less energy to participate in more activities (two patients declined robotic therapy).
A FIM gain of 18 was reported in a previous study with severe and critically ill COVID-19 patients who underwent pulmonary rehabilitation, 21 whereas the FIM gains in our study were 16 and 25 in the frail group and in the not frail or pre-frail groups, respectively. The latter is greater than the MCID of 22 for stroke 22 but should be interpreted with caution as it may not be specific for pulmonary rehabilitation. Although the differences in outcomes between the frail and not frail or pre-frail groups did not reach statistical significance, the frail group generally made fewer functional gains.
Limitations
There are trends towards the benefits of robotic therapy for post COVID-19 patients and the frail group making less gains in FIM and gait speed. These results did not reach statistical significance besides the rehabilitation length of stay favoring the robotic group in view of the limited sample size in this study. Furthermore, care must be taken when generalizing the findings to all COVID-19 patients, as this study consisted of patients who were deemed suitable for a trial of inpatient rehabilitation and may have excluded patients with milder symptoms who were discharged home directly with or without outpatient therapy. As this study looked at two time points, namely, at admission and at discharge, future work may consider the long-term benefits of rehabilitation with 3–6 monthly follow-up to review patients’ reintegration and function in the community.
This was a retrospective study, and we were not able to have equal numbers of patients in both the robotic and conventional groups and the frail and non-frail groups.
Conclusion
This study suggests that post COVID-19 patients benefit from inpatient rehabilitation with a comprehensive rehabilitation program and adjunct robotic therapy may be offered to further improve functional outcomes. Frailty may also be considered when establishing rehabilitation goals, as meaningful functional gains can still be achieved.
What is Known
• Post COVID-19 patients benefit from rehabilitation.
What is New
• Adjunct robotic therapy in conjunction with pulmonary rehabilitation may improve functional gains and outcomes. • Screening for frailty may be useful for managing expectations and establishing rehabilitation goals.
Footnotes
Author contributions
1st author designed the study and made the first draft. All authors reviewed the paper. The last author performed the statistical anaylsis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
CIRB 2022/2075.