
Abstract
Background
Controlling risk factors and lifestyle modification in coronary artery bypass graft (CABG) patients plays an important role and leads to the empowerment of these patients to take care of themselves. One way to empower these patients is to improve their self-efficacy and hope. This study aimed to investigate the effect of the planned discharge on cardiac self-efficacy and hope of CABG patients.
Methods
In this quasi-experimental study, the sample consisted of 60 people (30 in the intervention group and 30 in the control group). Data were collected using the Miller Hope Questionnaire and Sullivan Cardiac Self-Efficacy Questionnaire. Data analysis was performed using central indices of mean and standard deviation and Chi-square, t-tests and one-way analysis of variance. The software used for data analysis was SPSS version 19.
Results
The mean age of participants in the control group was 91/9 ± 86/91 and in the intervention, group was 33/7 ± 7/58. There was no significant difference between the demographic characteristics, heart self-efficacy and hope scores of the participants in the control and intervention groups. After the intervention, there was a meaningful statistical difference between the two groups at discharge time and 1 month afterward in both hope and cardiac heart self-efficacy scores (p = 0.001, 0.0001).
Conclusion
In this study, the implementation of the discharge program was effective in increasing the hope and cardiac self-efficacy of CABG patients and the use of the discharge plan is recommended to improve the outcomes of these patients.
Introduction
Cardiovascular disease has the highest mortality rate in the world. According to the latest statistics of the World Health Organization, 17.9 million people die from the disease every year. 1 Widespread coronary artery disease can cause complications such as congestive heart failure, acute pulmonary edema, cardiogenic shock and high mortality. It will also create enormous costs to patient care and treatment. 2
Coronary Artery Bypass Graft (CABG) is a surgical treatment option for patients with advanced coronary artery disease. 3 The number of open-heart surgeries is increasing and this surgery can increase the life expectancy and quality of life for patients with heart disease. 4 Although this procedure often increases the patient’s survival rate, chronic heart disease patients are still at high risk for future heart problems. 5 Patients undergoing CABG surgery require vast changes in lifestyles and they require careful care. In addition, the treatment outcome of coronary artery disease is adherence to the discharge treatment plan for assuring one’s ability to adapt to changes in life. 6
Controlling risk factors related to the patient’s lifestyle plays an important role in empowering patients to take care of themselves. One way to empower these patients is to improve their self-efficacy. 7 Self-efficacy is a key variable in clinical, educational, social, developmental, health and personality psychology. In addition to adapting to disease and treatment, it has also been shown to affect health activities. 8 Various studies have shown that high self-efficacy can promotes health behaviors and reduce disease symptoms and physical limitations of patients with heart disease, thereby improving their health. 3
Cardiac self-efficacy is a measure of one’s beliefs about the ability to perform activities and deal with the challenges of heart disease. It motivates the patient to follow a healthy lifestyle. It is also a very strong predictor of behavior change in patients of any age and economic status. 9 Therefore, cardiac self-efficacy is a valuable intervention tool for nurses use in health centers and a nurse’s evaluation and promotion of patient’s cardiac self-efficacy can increase patient’s self-care motivation. 7
Along with cardiac self-efficacy, hope is an important psychological characteristic. Hope is a basic concepts of positive psychology and a factor that enriches of human life.10,11 Hope can empower patients to see beyond their current unfortunate condition. Even more, despair reduces the quality of life and it leads to hopeless feelings. Studies have shown that higher hope is associated with higher morale and physical health, as well as higher ability to cope with disease. In practice, hopelessness and lack of purpose in life reduces patients' quality of life and creates negative beliefs. Providing hope to patients is an important intervention in the field of medicine, nursing and mental health. Supportive actions associated with hope in heart patients can affect the health of these people. 10 In addition, it has been shown that caring education and patient and family counseling are factors that increase patient hope. 12
As mentioned earlier, patients undergoing open-heart surgery have a high risk of ongoing heart disease and postoperative complications. It can be said the success rate of cardiac surgery is limited unless the patient has sufficient knowledge regarding appropriate activity, diet, exercise, and treatment regimen after surgery. 5 For patients undergoing open-heart surgery, the post-operative phase is the most critical period. During this period, complications such as pneumonia, cardiovascular or neural and kidney problems may increase the length of the hospital stay and treatment costs. These complications directly affect the patient’s survival rate. 13
The post-discharge period is the best opportunity for the treatment team to have a positive impact on the patient’s outcomes and is the priority intervention. 14 Studies have shown that discharge planning is related to the positive outcomes of the patients, and significantly reduces the hospitalization rate and increases survival rate of the patients. These plans improve the quality of life and physical function for the patient. 15 The plan also enables patients to perform self-care activities and meet personal needs. 16 The purpose of the discharge plan is to reduce the time of hospitalization or rehospitalization after discharge, and improve the coordination of services after discharge. 17
Nursing staff training for implementation of the discharge plan is a key component for health improvement services. 18 Planning for discharge should begin at the time of hospital admission and be coordinated by a multidisciplinary team of health professionals. However, cardiac surgery centers usually educate patients only at discharge time regarding postoperative care, diet, exercise, and rest. This is done by the nurses who play the most important role in patient education. 13
In the past, there have been several studies investigating the impact of discharge programs on a number of variables, including hope and self-efficacy among different communities. Here are some of these studies: A study of 403 cardiac patients by Zhou (2018) in Shanghai investigated the effect of nurse follow-up and telephone training for cardiac self-efficacy revealed the patients’ cardiac self-efficacy score 6 months after nurse follow-up with both intervention and control groups was increased, and the mean score of self-efficacy was higher in the intervention study group than the control group. 19 A study by Cajanding (2017) with a sample of 143 patients in the Philippines on, followed a 3-day nursing discharge plan, the intervention group improved significantly in performance and cardiac self-efficacy scores. 15 A study conducted by Poorgholami (2016) with 75 hemodialysis patients in Shiraz City, Iran examined the effect of self-care education with and without telephone follow-up on patients' hope level revealed that the level of hope was significantly higher in the intervention group receiving self-care training and in the intervention group receiving self-care training with telephone follow-up than in the control group receiving only routine care. 12
Despite the benefits mentioned for discharge planning, few studies have been conducted to evaluate the impact of its implementation on various variables, especially hope and cardiac self-efficacy for open-heart surgery patients in Iran. So, the aim of this study was investigating the effect of a planned discharge program on hope and cardiac self-efficacy of CABG patients referred to Shafa health center in Kerman.
Methods
Design
This study is a quasi-experimental study (before/after) conducted in the Department of Cardiac Surgery at Kerman Shafa Hospital. It is the first and largest cardiac surgery ward in the province, with 20 beds. The study population are patients undergoing coronary artery bypass surgery.
Sample
The number of patients in each group was 30, and finally 60 patients participate in the study. Random sampling was conducted first for the intervention group and then the control group by tossing a coin. Sample size was determined using the study data by Barnason (2003)
20
and the following formula.
Inclusion criteria included: patient awareness, ability to hear, to see and speak clearly, speaking Persian and exclusion criteria included: previous history of open-heart surgery, over 85 years of age, patient’s unwillingness to participate in study and patient’s death during or after surgery. Patients undergoing CABG surgery were included in the study if inclusion criteria were met. In this study, due to the obvious type of the educational intervention and discharge program in the intervention group, no blinding was performed for participants and researchers.
Data collection
The instruments used in this study consist of three parts: demographic information form, hope questionnaire and cardiac self-efficacy questionnaire. The demographic questionnaire included questions regarding participant’s age, sex, marital status, occupation, level of education and place of residence (city or village).
The Sullivan Cardiac Self-efficacy Questionnaire was used to measure patients’ cardiac self-efficacy. The questionnaire composed of 16 items on a five-point Likert scale was developed by Sullivan. 21 The scores range from 0 to 64. Scores between 0–21 indicate weak self-efficacy, 22-42 moderate self-efficacy, and 43–64 strong self-efficacy. In the research by Shamsizadeh (2012) the face and content validity of this tool was confirmed, and its reliability was reported by Cronbach’s alpha for the questionnaire of 0.977.22,23
The Hope Miller questionnaire was used to measure the hope of cardiac surgery patients. This questionnaire was first developed by Miller in 1988. The questionnaire is based on the 5-point Likert scale ranging from strongly disagree to strongly agree. This questionnaire has 48 items, and it should be noted that the Likert rating scores for 14 questions are reversed. The minimum score is 48 and the maximum score is 240. A score of 48–96 indicates low hope, a score of 97–144 indicates medium hope, and a score higher than 144 indicates high hope. Miller reported the validity of the questionnaire as desirable and rated it as Cronbach’s alpha over 0.80. 24 This questionnaire was translated from English to Persian and used in various studies in Persian. In the research by Hosseini (2006) and Khezri Moghaddam (2017), the questionnaire was valid and the Cronbach’s alpha coefficient was 0.90 and 0.81 for determining the reliability of the questionnaire, respectively.25,26
In this study, upon admission, patients were first told about the purpose of the study, and the informed consent paperwork was completed by patients willing to participate in the study. Next all patients completed demographic, cardiac self-efficacy and hope questionnaires. When necessary, the researchers completed the questionnaires via face-to-face interviews. Patients in both intervention and control groups filled out hope and cardiac self-efficacy questionnaires again at hospital discharge and 1 month after discharge to determine the impact of the discharge plan on hope and self-efficacy.
The discharge plan was conducted in three one-hour training sessions for the intervention group individually or in groups by the researcher.
Patients, at the time of admission to the hospital and before surgery, were trained regarding CABG cardiac surgery and possible recurring symptoms, as well as the preoperative preparation and, the general course of surgery. The training also covered possible complications occurring from open-heart surgery. (Before surgery)
Patients were trained regarding post-operative wound and chest care and how to bathe and manage postoperative pain such as relaxation techniques and deep breathing exercises and painkillers, as well as post-operative breathing exercises to improve lung function and patient activity. (During hospitalization (3–4 days after surgery and after hemodynamic symptoms stabilized)
Training continued on the day of discharge regarding management of the patient’s diet, medication and applying a healthy lifestyle. Training also included discussion regarding the optimal time to return to work, resume sexual activity and participation in a cardiac rehabilitation program. Problems and complications after surgery and when to see a physician were included in the day of discharge training All of the training sessions were held in the heart surgery ward of Shafa Hospital. Teaching methods included lectures and questions and answers. Educational aids such as computer and video projection and educational images and slides were also used. In addition, on the day of hospital discharge, a self-care training booklet was delivered to the patients in the intervention group. Patients in the control group only received routine training on the day of hospital discharge. In This research, data collection lasted from March 1 to August 15, 2020.
Data analysis
In this study, central and dispersion indices, Chi-square, independent t-test and one-way ANOVA with a significant level of 0.05 were used for data analysis. SPSS software version 21 was used for data analysis.
Results
In this study, data on 60 patients (30 in the intervention group, 30 in the control group) were finally analyzed (Figure 1). The mean age of participants in the control group was 60.86 ± 9.91 and in the intervention group it was 58.70 ± 8.33. The frequency of other demographic characteristics of the two participant groups, included gender, marital status, occupation, level of education, and residence are shown in Table 1. There was no significant difference between the demographic characteristics of the participants in the control and intervention groups (Table 1). Participants’ flowchart. Frequency of demographic variables in intervention and control groups. aChi-square test was applied.

Comparison of the mean score of hope and cardiac self-efficacy
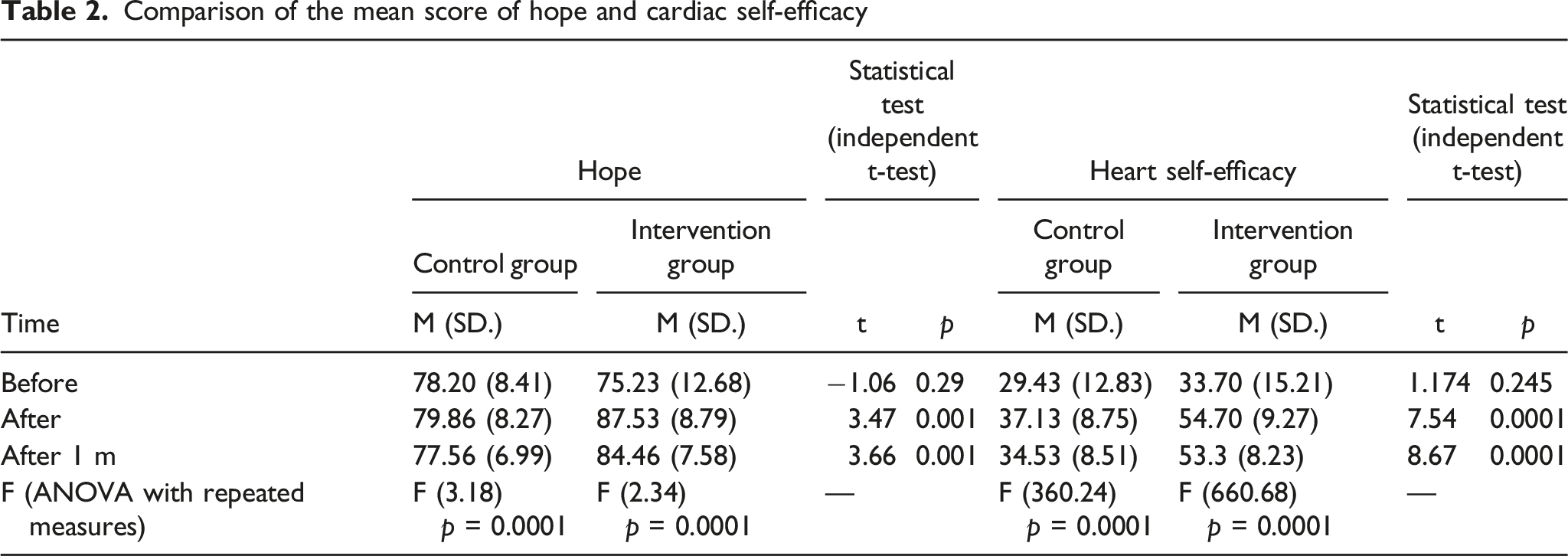
The results of this study also showed that the mean score for cardiac self-efficacy for patients in the intervention and control groups before intervention was 29.43 ± 12.83 and 33.70 ± 15.21, respectively, which were not significantly different (p = 0.24), and the level of cardiac self-efficacy was also low in patients in the intervention and control groups before intervention. Cardiac self-efficacy scores following intervention in the control and intervention groups were 37.13 ± 8.75 and 54.7 ± 9.27, respectively, and again one month following intervention, 34.53 ± 8.51 and 53.3 ± 8.23 were shown, respectively (p > 0.001). This means that cardiac self-efficacy increased in the intervention group immediately and 1 month following intervention compared to the control group (Table 2).
Discussion
Due to the nature of the disease and surgery, many patients undergoing CABG surgery face problems such as low self-confidence in performing daily tasks, anxiety, depression and a severe decline in quality of life, which in turn leads to loss of hope and cardiac self-efficacy. Effective interventions can reduce many of these patients’ problems. The results of this study showed the level of hope prior to surgery was low for patients in both intervention and control groups. The hope score for the intervention group showed a significant increase immediately following the discharge plan and 1 month later when compared with the control group.
The results of the Shojaee (2013) study to determine the effect of the educational program and telephone follow-up on hope in patients with heart failure were consistent with the findings of the present study. Educational intervention significantly increased the level of hope of patients in the intervention group. 27 In the Poorgholami (2016) study, which examined the effect of stress management and self-care educational intervention on the level of hope of patients undergoing hemodialysis, it was determined the implementation of education increased the hope of patients in the intervention group. 12 Although in both of these studies, the intervention program and patient sample were different from the present study, performing an educational intervention for patients such as the present study, performed at the time of discharge, increased patients' level of hope. In these studies, as in the present study, the Miller Hope Questionnaire was utilized. Overall, the intervention period in the present study was longer compared to the studies mentioned above. Additionally, the reviewed studies did not evaluate post-discharge patient hope. The present study included post-discharge evaluation of cardiac rehabilitation and its combination with education and counseling. The post-discharge intervention significantly increased the level of hope in CABG patients.
The findings of a qualitative study conducted by Ingram (2017) showed participants, including 37 parents of neonates admitted to the neonatal intensive care unit, had a generally positive view of the discharge program and they considered the implementation of this program to be effective in increasing their hope level. 28 The results coherence of the above studies indicates that training programs were effective in increasing hope for the group receiving the intervention.
There are advantages to training at the time of discharge. Heart surgery patients usually feel that the special nursing services provided to them in the hospital will end at discharge time. Therefore, they suffer from psychological reactions such as fear, anxiety, stress, and consequently they despair. Receiving training at the time of discharge can be a good incentive to continue home care and thus increase hope. In principle, nurses play an important role in this process by establishing a close caring and emphatical relationship with these patients. Shojaee (2013) stated “nurses can be a factor for motivation and transformation of hope in patients, and this is possible by having relationships with them, being by their side, actively listening to the patient, and providing empathy with the patient. We can say that nurses using interventions that meet these goals can raise patients' hope.” 27
The results also showed that the mean score of cardiac self-efficacy for patients before the intervention was low in both intervention and control groups. The self-efficacy scores of the intervention group increased significantly after the intervention and a month later. Ghonaem (2018) studied the impact of applying a discharge program for postoperative complications, knowledge and cardiac self-efficacy of patients undergoing coronary artery surgery, and showed that after the discharge plan, the cardiac self-efficacy of participants was significantly improved. 5 Kaveh Savadkooh (2012) implemented a self-management program to evaluate the self-efficacy of hypertensive patients, which investigated application of a self-management program to promote and improve patients' self-efficacy. In this study, only one training session was employed and the cardiac self-efficacy questionnaire used was a researcher-developed adapted from self-efficacy questionnaires for chronic patients. 29 In the study of Borzou (2018), after the intervention of the first phase of the cardiac rehabilitation program, the cardiac self-efficacy rate of CABG patients in the intervention group was significantly increased. 30 This result is in line with the result of the present study, despite the difference in the type of intervention and the researcher-developed cardiac self-efficacy questionnaire. Self-care education for heart patients significantly increased the level of self-efficacy in patients studied in Fors (2016). 31 However, it should be noted that in that study, a cardiac self-efficacy questionnaire different from the present study questionnaire was used to measure patients' cardiac self-efficacy.
Self-efficacy includes the patient’s confidence in the ability to perform self-care activities properly enabling the patient to achieve appropriate results. 32 What is certain is that self-efficacy is one of the important components that motivate patient recovery. Cardiac self-efficacy is the patient’s confidence in their ability to perform activities that are affected by the symptoms and complications of their cardiovascular disease. Psychological factors such as anxiety and cardiac self-efficacy may influence the development of chronic diseases through psychological distress and patient behaviors. 33 Therefore, due to the effectiveness of the training program at the time of discharge, many of the patient’s physical and mental problems, which are dependent upon self-efficacy, are eliminated or adjusted.
It should be noted in Mohamadinejad (2015) implementation of the educational program significantly increased the level of self-efficacy of patients with diabetes in the intervention group. 34 The self-efficacy questionnaire used in that study was different from the present study and the self-efficacy questionnaire of diabetic patients was used. Similarly, in the study by Dehnabi (2017), the implementation of a discharge program in patients with type 2 diabetes significantly increased the level of diabetes self-efficacy for the patients. 35 As it is clear, in these studies, despite the differences in the sample of patients and medical context with the present study, educating and supporting patients and implementing a discharge program improved the level of self-efficacy. In this regard, Varaei (2017), which investigated the effect of peer education on cardiac self-efficacy and readmission rate of for patients undergoing CABG surgery, the implementation of intervention significantly increased patient of cardiac self-efficacy levels. 36 In Naderi Pour (2014) study, the level of self-efficacy of patients with a history of CABG surgery after performing self-care education intervention to patients had increased but was not significant. 32 However, the difference may be due to study design and other intervention methods with participants. Also, in Naderi Pour (2014), a general self-efficacy questionnaire was used, which was different from the present study questionnaire.
The results of the above studies confirm the results of the present research design. Based on this study, the implementation of a discharge plan is effective for developing and sustaining hope and cardiac self-efficacy for patients undergoing CABG surgery.
Limitations
There were some possible limitations of this study. First, the number of participants was small and generalizing across populations would not be warranted. Second, the data collection was limited to one open-heart CABG surgical site. Third, more phase of training could be offered when the patient returned to the hospital for the rehab program.
Conclusion
According to the current study, the implementation of an educational discharge plan significantly increased the level of cardiac self-efficacy and hope of patients. It is highly important for caregivers to meet the physical and psychological needs of patients through training and support. Patients benefit from training to manage post cardiac surgery self-care and home recovery with confidence. The beneficial effect of implementing an educational discharge plan for patients before and following open-heart surgery is significant. Finally, according to the findings of this study and the reviewed literature, discharge plan training is recommended for patients undergoing CABG surgery as well as other chronically ill patients.
Footnotes
Acknowledgements
The authors would like to appreciate the personnel of cardiac surgery department for their assistance in this research and all of the participants.
Author contributions
MA researched literature and conceived the study and gained ethical approval. TE and ZD were involved in patient recruitment, performing the intervention and data collection and BT did the data analysis. TE wrote the first draft of the manuscript. All the authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The researchers conducted this study, after registering in Kerman University of Medical Sciences, obtaining a code of ethics from the Ethics Committee [IR.KMU.REF.1398.579], an introduction letter from Kerman University of Medical Sciences, informed consent from all participants, and complying with the principle of privacy.
Informed consent
Before conducting the research, the author explained all the required information to the participants and the written consent form was signed by all participants.
Data availability
The datasets and educational content used in current research are available by contacting the email address [forozy@gmail.com].