
Abstract
Introduction
A multi-disciplinary approach has often been advocated to improve the delivery of oncological care, as compared to a mono-disciplinary and linear approach. Our study elucidates the clinical and patient-reported outcomes from a urologic-oncology multi-disciplinary team (MDT) clinic in a regional general hospital.
Materials and Methods
Patients who attended a uro-oncology MDT clinic which was started in January 2019 were identified. This service was specifically catered to patients who were histologically diagnosed with urological cancers. The MDT service comprised a multi-disciplinary tumour board followed by outpatient clinical consults with representatives from urology, medical and radiation oncology. Demographic variables, disease characteristics and treatment rendered were analysed. A survey was administered to assess patient satisfaction.
Results
Fifty patients with a median age of 70 years with complete case records were identified. The cancer types included prostate cancers (46%), urothelial cancers (26%) and renal cell carcinoma (12%) as the most frequent urological cancers. The median time from MDT to therapy initiation was 8 days. Among those with prostate, urothelial, renal and testicular malignancies, 71% (32/45) of our patients received treatment that were in accordance to guideline recommendations. A post-clinic survey showed that patients were satisfied with the information provided during the clinic and this also facilitated decision and time to initiation of therapy.
Conclusion
A multi-disciplinary service comprising a tumour board followed by a one-stop clinic provides patients with multi-disciplinary care, improved access to subsequent therapy, better time efficiency and high patient satisfaction scores. More studies are warranted to demonstrate its oncological outcomes.
Introduction
A multi-disciplinary and patient-centric approach has often been advocated to improve the delivery of oncological care, as compared to a mono-disciplinary and linear approach. 1 Traditionally, multi-disciplinary approaches have been largely defined by paper discussions alone without actual patient involvement.
The idea of multi-disciplinary involvement in patient care was conceptualised several decades ago and its rapid uptake has often been cited to improve patient-outcomes across the various medical fields.2-3 Key to this strategy would be the provision of comprehensive evaluation and treatment recommendations from multiple perspectives, which potentially improves the level of care in complex clinical scenarios. For instance, Pawlik and colleagues studied the impact of a single-day multi-disciplinary clinic on the management of pancreatic cancer and found that multi-disciplinary case review resulted in an overall 23% change in therapeutic plan of patients with presumed pancreatic cancer. 4 Similarly, in the urological oncology space, multi-disciplinary clinics for prostate cancer have generally been well-received and played an important role in altering management decisions.4-5 There is sparse literature about the provision of a urologic-oncology multi-disciplinary team (MDT) clinic in a regional hospital, and there is limited data on patients’ perceptions related to such services.6-7
This study elucidates the clinical and patient-reported outcomes from a urologic-oncology multi-disciplinary clinic in a regional general hospital over a duration of 1 year since its conception.
Materials and Methods
In our traditional paradigm of patient care, patients diagnosed with a genitourinary malignancy would have management plans discussed at a regular genitourinary tumour board. This platform allowed clinical decision regarding treatment to be made amongst specialities, but did not have the benefit of in-person patient assessment. This would inevitably lead to multiple visits by the patient across all three oncology specialities, and pose a challenge to a holistic care plan when there was an ipsilateral change in management plan required.
A dedicated urologic-oncology MDT clinic was started in January 2019 in a regional acute care hospital with 1000 inpatient beds. This outpatient clinic was specifically catered to patients who were histologically diagnosed with urological malignancies including prostate, urothelial, renal, penile, testicular and adrenal cancers, in particular those with conditions where the management may require two or more specialities’ input. In this one-stop service, there is specialist representation from urology, medical oncology and radiation oncology, and was intended to facilitate clinical decision making between specialties and with the patient, as opposed to unilateral decisions between specialities at different visits in the traditional model. All relevant specialists were simultaneously present in the same consultation room during the MDT clinic visit. Each consultation episode was allocated 20 min for resource scheduling purposes. This clinic was held regularly before COVID-19 (coronavirus disease 2019) led to a temporary change in the clinical practice landscape in Singapore. Each MDT session was preceded by a genitourinary tumour board for a paper-based case discussion, together with mandated central pathological and radiological review.
With IRB approval, patient information was obtained from electronic case records. The patients’ treatment plans were reviewed and assessed if they had adhered to recommended first-line therapies based on current guidelines.8-9 The time savings to the patient from the MDT service were also approximated, assuming that a reduction of one clinic visit was equivalent to timing savings of 75 min (comprising 15 min of clinic consult time and 60 min of travel time). Within a month of each MDT clinic visit, a patient survey was administered by phone interview comprising three standardized questions. The responses were scored on a Likert scale ranging from 1 (very unsatisfied) to 5 (very satisfied). The three questions specifically enquired if patients found the MDT clinic session informative and reassuring, if there was travel time saved, and whether the MDT session facilitated the decision making and shortened the time needed to commencement of treatment (Supplementary Table 1).
Results
Baseline Characteristics of Patients Attending our Multi-Disciplinary Clinic.

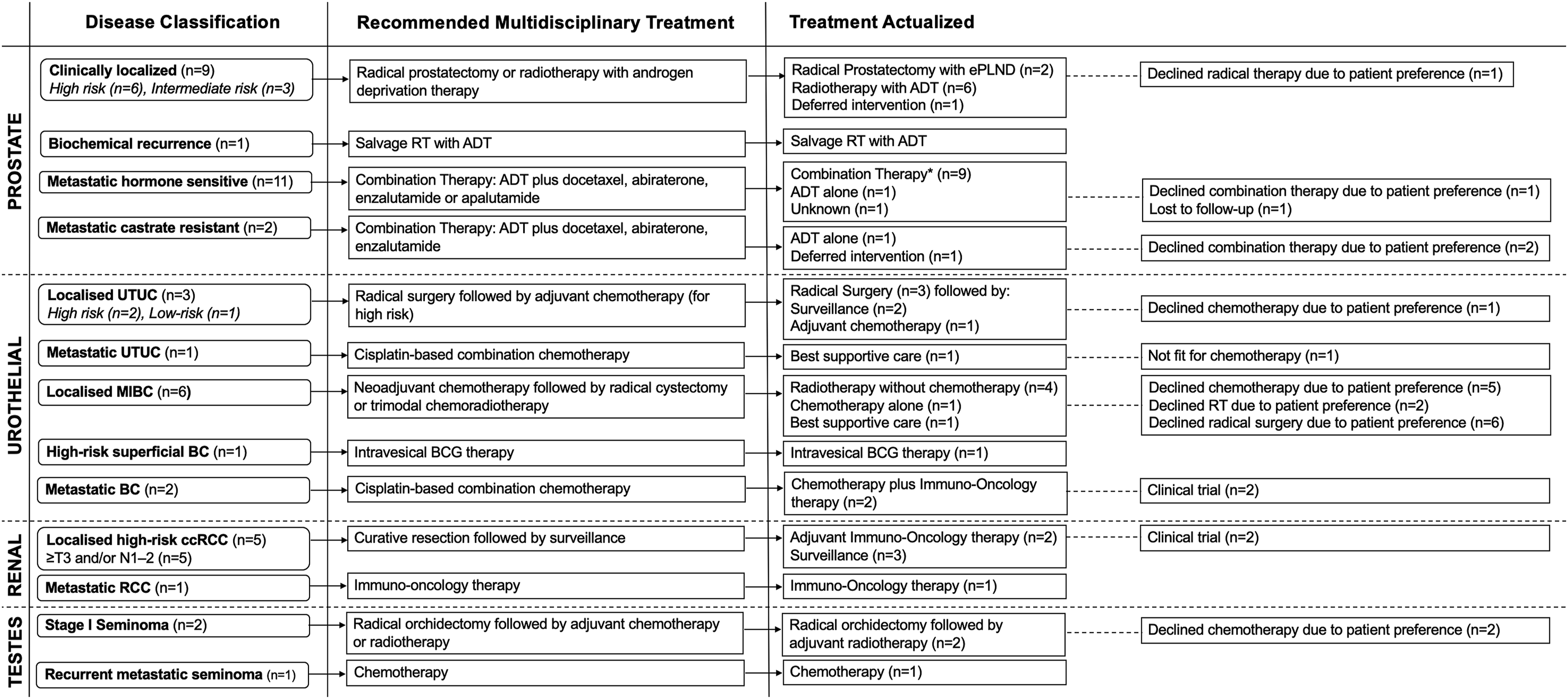
Schematic depicting the distribution and recommended treatment modalities of the most common urological cancers. *Combination therapy refers to androgen-deprivation therapy plus docetaxel, abiraterone, enzalutamide or apalutamide. ADT: androgen-deprivation therapy, BC: bladder cancer, BCG: bacillus calmette guerin, ccRCC; clear cell renal cell carcinoma, ePLND: extended pelvic lymph node dissection, MIBC: muscle-invasive bladder cancer, RT: radiotherapy, UTUC: upper tract urothelial carcinoma.
Results from Patient Satisfaction Survey.

Discussion
Our current model of care in patients with urological malignancies relates to an academic paper discussion at a multi-disciplinary genitourinary tumour board with necessary pathological and radiological review. In this traditional model, the patients’ case details are discussed at a separate meeting and the key decision-making treatment process often occurs without physical consultation of the patient. The multi-disciplinary team approach has been shown to affect diagnostic and management decisions in urological malignancies where there is a benefit for multi-disciplinary input and collaboration. 10 Jang et al. previously analysed the Surveillance, Epidemiology and End Results-Medicare linked database and found a strong correlation between the type of specialist that was visited, and the type of prostate cancer treatment subsequently received for organ confined disease. 11 Hence, patient preferences for treatment were very much influenced by specialist type at the initial consult, and that a significant proportion of men did not have the benefit of a multi-speciality consult prior to treatment initiation. These findings underscore the importance of providing a balanced viewpoint of the treatment options to the patient, especially in disease types where there is a lack of clinical superiority of one treatment modality over another. 12
Our current study describes the outcomes of the MDT process in our unit where the process of multi-disciplinary clinical collaboration is multi-faceted. Firstly, the initial multi-disciplinary discussion and central review of pathology and radiology provides the platform for accuracy and consistency in diagnosis and staging, while serving as an educational opportunity to residents in training. Secondly, it provides an opportunity for each relevant speciality to pursue meaningful discussions in person with the patient. For example, in muscle-invasive bladder cancer where staged treatment protocols are indicated (e.g. neoadjuvant therapy prior to radical cystectomy), there is facilitation of patient and physician(s) communication in this setting. In addition, there is also facilitation of inter-speciality scheduling and resourcing which would, otherwise, require more coordination in a historical linear model. The other specific benefits to the patient include a short time interval to initiation of treatment and indicates an attempt towards more expeditious cancer treatment in a public healthcare system which is consistently challenged with resourcing and wait time. 13 The timing savings that are approximated have positive implications on patients who are still in employment and require time off work. For care-givers accompanying the patients at these MDT sessions, the time savings to these individuals also apply, and the totality of effect is magnified as a system. Hence, the cost savings of this new initiative is difficult to quantify exactly, as the quantum extends beyond the calculable expenditure reductions in trip and consult savings.
Our patient-reported survey also suggests that the MDT clinic is well-received and affords convenience to the patient and care-giver. We postulate that the multi-disciplinary platform that affords in-person consult promote trust between the various parties and also allows the oncology team to execute best practices to foster connection and trust with patients. 14 Patient involvement in the decision-making process also helps in establishment of trust in the physician-patient relationship. 15 Only one patient reported feeling very unsatisfied with regard to the MDT reducing time to treatment. It is possible that the patient expected a recommendation to be made on his behalf during the clinic visit. However, the team maintained the need for the individual decision making by the patient. Hence, this led to a discrepancy in expectations.
However, the MDT approach does not ensure that all evidence-based recommendations are adopted, and treatment ‘deviation’ occurred in about 29% of cases, largely reflecting the decisions made by the individual patients. While there is evidence of alignment in priorities between patient and physician in prostate cancer treatment, other social and cultural factors may also be contributory especially in a multi-racial practice. 16 Hence, the MDT approach ensures ease of access to information and also treatment resources in our practice. The incremental benefit of the MDT clinic over the traditional linear approach is difficult to quantify precisely as it is not possible to conduct a randomised comparison between the two, in light that MDT board meetings are already highly prevalent in practice.
Several tertiary institutions around the world have already employed multi-disciplinary approaches towards providing holistic care for oncological patients. A group from Thomas Jefferson University had previously reported their 15- year experience in establishing a multi-disciplinary cancer clinic and demonstrated that their 10-year survival data for high-risk, locally advanced prostate cancer had exceeded that of the SEER cohort. 5 Arguably, there is likely selection bias and confounding factors which cast doubt on the true impact of the MDT clinic on their reported oncological outcomes. Men diagnosed with low-risk prostate cancer who attended the multi-disciplinary clinic at academic centres affiliated with Harvard Medical School were also more likely to choose active surveillance compared to those who were treated by individual practitioners in separate settings, thereby suggesting that multi-disciplinary clinics may reduce physician bias. 6 Kulkarni and colleagues also reported that bladder-sparing trimodal therapy yielded comparable survival outcomes to those of matched patients who underwent radical cystectomy, in setting of a multi-disciplinary bladder cancer clinic where patients were evaluated by urologic, radiation and medical oncologists. 17
Several limitations have to be addressed. Follow-up on oncological outcomes and further comparative studies using historical or parallel cohorts are warranted. While a matched analysis will allow for more robust and scientific comparison, confounding factors due to the heterogeneous profile of the patients seen in the MDT clinic may unfairly influence the comparative analysis. Moreover, it is important to distinguish the benefit of multi-disciplinary discussion from multi-disciplinary consultation. The former ensures that the patient’s disease is appropriately diagnosed and staged, while the latter ensures that the patient is given a fair representation of the available treatment options. In our study, time-savings calculations were merely estimations for consultation and travel time between each institution. While our sample size is small, this pilot initiative serves as a stepping stone for further expansion of this multi-disciplinary service locally. Importantly, multi-disciplinary clinics require dedicated resources and commitments from various speciality physicians and is seen as inefficient given that only a limited number of patients can be seen. 4 It is also recognised that significant administrative and logistical coordination is required to sustain the MDT clinic between three different specialities. Our MDT clinic was held monthly and were able to cope comfortably with 10 cases per session due to a stringent inclusion criterion. For holistic oncology care, our centre is working towards the future involvement of specialist cancer nurses, social workers and other allied healthcare workers.
Lastly, the oncological benefit of the MDT clinic is difficult to ascertain as there is significant evolution of treatment modality with time, and patient prognosis is also largely dependent on disease characteristics and response to treatment.
Conclusion
In conclusion, a one-stop MDT clinic provides patients with multi-disciplinary care, improved access to subsequent therapy, better time efficiency and high patient satisfaction scores. More studies are warranted to demonstrate its clinical significance on oncological outcomes.
Supplemental Material
sj-pdf-1-psh-10.1177_20101058211055222 – Supplemental Material for The Uro-Oncology Multi-disciplinary team (MDT) Clinic – Clinical and Patient-Reported Outcomes From Implementing a New Model of Care
Supplemental Material, sj-pdf-1-psh-10.1177_20101058211055222 for The Uro-Oncology Multi-disciplinary team (MDT) Clinic – Clinical and Patient-Reported Outcomes From Implementing a New Model of Care by Alvin Y Lee, Raj Tiwari, Shuhui Neo, Daanesh Huned, Arjunan Kumaran, Chloe Li Wen Lim, Melvin Lee Kiang Chua, Ravindran Kanesvaran and Lui Shiong Lee in Proceedings of Singapore Healthcare
Footnotes
Author Contributions
Alvin Lee: formal analysis, writing – original draft. R Tiwari: formal analysis, writing – original draft. SH Neo: Writing – review and editing. D Huned: Writing – review and editing. A Kumaran: Writing – review and editing. CLW Lim: Writing – review and editing. Melvin LK Chua: conceptualisation, writing – review and editing. R Kanesvaran: conceptualisation, writing – review and editing. Lee LS: conceptualisation, writing – review and editing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained.
Informed Consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Data Availability
The datasets generated and/or analysed during the current study are not available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.