
Abstract
Background
A low–fermentable oligosaccharide, disaccharide, monosaccharide, and polyol (FODMAP) diet (LFD) appeared to improve gastrointestinal symptoms in patients with Irritable Bowel Syndrome (IBS). However, evidence of its efficacy in Asia remains scarce.
Objectives
This study aims to investigate the clinical effectiveness of LFD intervention among Asian IBS patients and barriers to its adherence.
Methods
Patients with IBS who were instructed to follow LFD by dietitians at a tertiary hospital in Singapore between July 2013 and December 2014 were retrospectively reviewed. Severity scores of 19 gastrointestinal symptoms were recorded using an 11-point rating scale (0 = “no symptoms,” 10 = “extremely severe”) pre- and post-LFD intervention. Adherence to LFD was assessed based on patients’ diet history and a high-FODMAP food checklist.
Results
Eighty-two patients with a median follow-up of 5.8 weeks were investigated. The LFD adherence rate was 61.0% (n = 50). Overall, statistically significant improvement was observed in 14 of 19 gastrointestinal symptoms (median difference = −2.0 to −0.5, p < .05). The proportion of patients who had improvement in 10 individual symptoms (defined as ≥1 point reduction in symptom severity rating) was significantly higher in LFD-adherent patients (67.5%–82.4%) than that of the non-adherent group (27.8%–55.0%). Reasons reported for non-adherence included “limited availability of low-FODMAP alternatives” (n = 9), “limited understanding of LFD” (n = 7), and “perceived lack of benefit” (n = 4).
Conclusions
LFD intervention improved gastrointestinal symptoms in a cohort of Asian IBS patients. Limited access to low-FODMAP alternatives was the main barrier to adherence.
Introduction
Irritable bowel syndrome (IBS) is a functional bowel disorder characterized by recurrent abdominal pain and associated with a change in bowel habits. Common symptoms of IBS include bloating, abdominal distension, and disordered bowel habits, such as diarrhea, constipation, or a mixture of both. 1 IBS is a common gastrointestinal condition, with an estimated global prevalence of 11.2%. 2 It was known to affect 3–20% of Western populations 3 and 0.8–31% of Asians. 4 In Singapore, the IBS prevalence was first reported to be at 2.3% by the Manning criteria. 5 A subsequent population-based survey found a higher IBS prevalence of 11%, 10.4%, and 8.6% by Manning, Rome I, and Rome II criteria, respectively. 6 Furthermore, a cross-sectional study reported a 20.9% IBS prevalence by Rome III criteria. 7 Although different diagnostic criteria of IBS were used across studies, previous findings could suggest an upward trend in IBS prevalence in Singapore over the past decades.
Although not life-threatening, IBS has a significant impact on patients’ quality of life (QoL).8–9 Thus, the consensually agreeable management goals for IBS were to alleviate symptoms and improve QoL. 10 Evidence has shown that a novel medical nutrition therapy (MNT), the low–fermentable oligosaccharide, disaccharide, monosaccharide, and polyol (FODMAP) diet (LFD), appeared to improve gastrointestinal symptoms in IBS patients.11–14 FODMAPs were postulated to trigger gastrointestinal symptoms by increasing the luminal osmotic content and inducing colonic gas production as a result of fermentation by intestinal microflora.15,16 Hence, a reduction in dietary FODMAP intake could lead to IBS symptom alleviation, particularly reducing osmotic diarrhea and gas-related symptoms.
The potential benefit of restricting dietary FODMAPs was first proposed by a retrospective study. Up to 74% of IBS patients achieved overall symptom improvement by restricting dietary fructose. 17 Shortly afterward, a randomized, double-blinded, placebo-controlled re-challenge trial discovered that a wider range of fermentable carbohydrates (fructose and fructans) induced IBS symptoms in 79% of the patients. 18 Subsequent studies continued to demonstrate that IBS patients on the LFD had experienced more significant improvements in overall gastrointestinal symptoms than those on controlled diets.19–22 With the emerging evidence in the past decade, the LFD was recommended as an efficacious dietary intervention to reduce IBS symptoms.11,23
Most recently, LFD has been recommended as a potentially helpful treatment modality for IBS by the second Asian consensus on IBS, despite the scarcity of evidence on LFD in the Asian population. 24 Hence, this retrospective study aimed to investigate the gastrointestinal symptom response to LFD intervention among local Asian IBS patients and explore the main barriers to LFD adherence in the Asian context.
Methods
Study participants
Patients with IBS were referred to a dietitian if deemed appropriate by the primary physicians at a tertiary hospital in Singapore. The records of patients who were instructed to follow the LFD by dietitians from July 2013 to December 2014 were retrospectively screened. Eligible patients must have reported at least one symptom on a gastrointestinal symptom rating scale at baseline and post-LFD intervention. Patients were excluded if they were pregnant, had a medical diagnosis of eating disorders, had any co-existing organic gastrointestinal condition(s), or had undergone any previous gastrointestinal operation(s).
The Low-FODMAP Diet intervention
The LFD intervention was implemented as a routine MNT for referred IBS patients at a tertiary hospital in Singapore. The LFD MNT protocol at the research site was adopted from previously published resources.11,25–28 At the baseline visit, the patient received a 1- to 1.5-h one-on-one dietary consultation on LFD by the dietitian at the specialist outpatient clinic. Dietitians involved in the current study have all completed the LFD training session to ensure that consistent dietary consultation was provided to each patient as per protocol. Topics for the education session included the mechanisms of LFD, different categories of FODMAPs, examples of high FODMAP foods and low-FODMAP alternatives, label reading, cooking methods, and eating-out strategies.
Patients were advised to avoid high-FODMAP foods, of which the FODMAP content was above previously proposed cutoff values (i.e., >0.5 g fructose in excess of glucose/100 g, >3 g fructose per serve, and >0.2 g fructans per serve). 11 Low-FODMAP alternatives (i.e., foods containing the amount of FODMAPs below these cutoff values) were suggested to replace the high-FODMAP foods in patients’ usual diet. Besides, patients were advised to restrain from local Asian food items, of which the FODMAP content was unknown at the time. At the end of the consultation, patients were provided with detailed education materials along with an individualized meal plan tailored to their nutritional needs.
Patients were advised to follow the LFD for 3 to 6 weeks. At the follow-up visit, patients who had adequate symptom improvement were advised to reintroduce FODMAPs to test the individual’s tolerance, thus avoiding any unnecessary long-term restrictions. The FODMAP reintroduction stage is beyond the scope of this study and will not be discussed in detail here.
Evaluation of gastrointestinal symptoms
The primary endpoint of the current study was the change in gastrointestinal symptoms post-LFD. Due to a lack of objective biomarkers in measuring treatment efficacy in IBS, the present study reported subjective measures of symptom severity on a self-administered 11-point rating scale (Supplementary Material 1). This rating scale was modified based on a few clinical scales29–31 that measured symptoms in patients with IBS and peptic ulcer disease. It was initially adopted by the gastroenterologist and dietitians at the research site for clinical purpose. Patients rated the severity of each symptom on the scale from “0” (no symptoms) to “10” (extremely severe) at baseline and follow-up visits. At the follow-up visit, the improvement in each symptom post-LFD was defined as a minimally 1-point reduction on the severity rating scale from the baseline.
Evaluation of LFD adherence
Previously published studies assessed dietary adherence based on various self-determined criteria.17,20,22 The LFD adherence assessment in the current study were based on the clinical judgment of the dietitians who provided care to patients with gastrointestinal disorders and were collectively agreed upon by all authors. The dietitians assessed patients’ adherence to the LFD via a thorough investigation of their reported diet histories in combination with patients’ self-declaration of their FODMAP intake by completing a self-administered FODMAP food checklist at the follow-up visit. The FODMAP food checklist consisted of more than 140 food items, including 130 food items containing excessive FODMAP per serving size and 14 local foods that had not been tested at the time of the study. A patient was assessed to be ‘non-adherent’ to LFD if one or more of the following three conditions were fulfilled during the LFD trial period: (1) the patient consumed any high-FODMAP or untested food items at more than 50% of the meals; (2) the patient consumed more than 20% of the food items listed on the FODMAP food checklist (i.e., more than 28 out of 144 food items); or (3) the patient reported having been non-compliant to the LFD upon review.
At the follow-up visits, patients were asked open-ended questions on barriers to adhering to the LFD, where applicable. Patients’ responses, if any, were documented in the dietitians’ report. In the present study, the dietitians’ reports were retrospectively reviewed, and the patients’ responses were extracted and examined using thematic analysis. They were read, re-read, coded into categories, and summarized into relevant themes. Themes were only finalized when two study members reached a unanimous agreement on all of them.
Statistical analysis
The normality of the distribution of continuous variables was examined by Kolmogorov–Smirnov tests. Wilcoxon signed-rank tests were used to compare the gastrointestinal symptom severity ratings pre- and post-LFD. Chi-square tests of independence were performed to investigate the differences in the proportion of patients with improvement in each symptom between the LFD-adherent and non-adherent patients. The difference in the follow-up duration between the adherent and non-adherent subjects was compared using the Mann–Whitney U test. Statistical analyses were performed using IBM SPSS Statistics for Windows (version 25.0, Armonk, NY: IBM Corp), and graphs were generated by GraphPad Prism (version 8.0.2 for Windows, GraphPad Software, San Diego, CA, USA). A p-value of less than .05 was considered statistically significant. This study was approved by the SingHealth Centralised Institutional Review Board following the Singapore Guidelines for Good Clinical Practices.
Results
Baseline demographics
Ninety-six patients were screened for eligibility (Figure 1). Fourteen patients were excluded, including one with an eating disorder, seven who previously had gastrointestinal operations, and six with co-existing gastrointestinal abnormalities. Eventually, 82 subjects were eligible. The baseline characteristics of the subjects are detailed in Table 1. Most subjects were female (n = 59, 72.0%) and of Chinese ethnicity (n = 69, 84.1%). The median follow-up duration between two dietitian visits was 40.5 (range: 19–268) days. Fifty subjects (61.0%) were assessed to be adherent to LFD by dietitians at the follow-up visit. The median follow-up duration of the adherent group was significantly shorter than that of the non-adherent group (35 days vs 43 days, p = .032). Flowchart of subject selection. Baseline Characteristics of All Subjects (n = 82). aStandard deviation. bInterquartile range.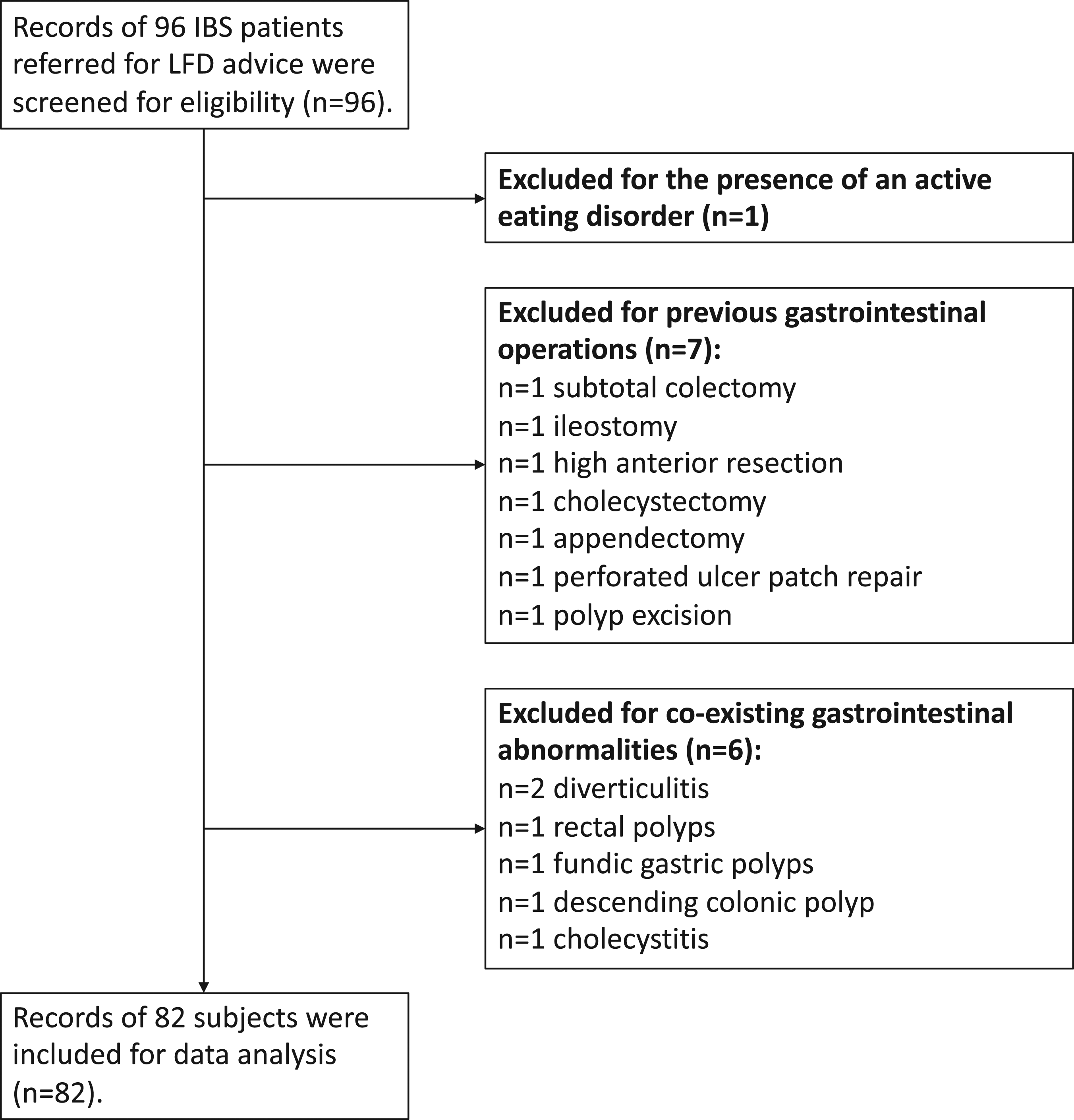

Baseline symptoms
Baseline Symptoms in All Subjects (n = 82).

Number of subjects who reported the symptom at baseline.
bMedian refers to the gastrointestinal symptom severity ratings at baseline.
Changes in gastrointestinal symptom severity post-intervention
Figure 2 illustrates the changes in symptom severity post-LFD intervention. Table 3 details the median difference (MD) of severity rating for each symptom. Overall, the severity of 14 symptoms reduced significantly post-LFD intervention in all subjects (MD = −2.0 to −1.0, p < .05). Albeit without achieving statistical significance, a reduction in severity ratings of four symptoms (“discomfort or pain anywhere in the abdomen—with fasting,” “stools appear frequently hard,” “bowels open with incomplete emptying,” and “fatty greasy stools”) was observed (MD = −1.0 to −0.5, p > .05). Differences in Gastrointestinal Symptoms Pre- and Post-Low FODMAP Diet. S1: discomfort or pain anywhere in the abdomen—all the time; S2: discomfort or pain anywhere in the abdomen—after meals; S3: discomfort or pain anywhere in the abdomen—with fasting; S4: discomfort or pain anywhere in the abdomen—does not go away after opening bowels; S5: abdominal rumbling; S6: bloating; S7: nausea; S8: vomiting; S9: loss of appetite; S10: burping or belching; S11: feeling uncomfortably full after a regular-sized meal; S12: flatulence; S13: stools appear frequently hard; S14: diarrhea; S15: alternate solid/loose stools; S16: constipation; S17: bowels open frequently with pain; S18: bowels open with incomplete emptying; S19: fatty greasy stools. Asterisks indicated statistically significant differences (p-value <.05) between the gastrointestinal symptom ratings pre- and post-LFD intervention. Median Differences of Symptom Severity Post-LFD in All, Adherent, and Non-Adherent Subjects. aNumber of patients who rated respective symptom at both baseline and follow-up visit. bMedian difference. cp-value refers to Wilcoxon signed-rank tests on the symptom severity ratings pre- and post-LFD intervention.

Similarly, the analysis of the subjects who were adherent to LFD alone revealed a significant severity reduction post-LFD in 14 out of the 19 symptoms (MD = −2.0 to −1.0, p < .05). The severity rating of the remaining five symptoms, including “discomfort or pain anywhere in the abdomen—with fasting,” “vomiting,” “stools appear frequently hard,” “bowels open with incomplete emptying,” and “fatty greasy stools,” improved to a lesser degree without reaching statistical significance (MD = −1.0 to −0.5, p > .05). On the contrary, only one symptom, “flatulence,” improved significantly post-LFD intervention (MD = −1.0, p = .025) in the non-adherent subjects.
Number and Percentage of Subjects Who Reported Improvement in Each Symptom Post-LFD.

aNumber of subjects who rated respective symptom at both baseline and follow-up visit.
bNumber of subjects whose symptom severity rating reduced by at least 1 point on the 11-point rating scale.
cPercentage of subjects who improved post-LFD.
dp-value refers to the chi-square tests of independence on the proportion of subjects who improved in each symptom between the adherent and non-adherent subjects.
Reasons for non-adherence
Among those who did not adhere to LFD, 20 subjects (62.5%) provided reasons for non-adherence. A total number of 23 reasons were stated by these patients. These were grouped into themes with the most frequently cited reason being “limited availability of low-FODMAP alternatives” (n = 9). Other reported reasons for non-adherence were “limited understanding of LFD” (n = 7), “perceived no benefit of LFD” (n = 4), and others (n = 3).
Discussion
To the best of our knowledge, while previous evidence on LFD in the western IBS population was abundant, the number of studies that investigated the effects of LFD on gastrointestinal symptoms among the Asian IBS cohort remains limited.32–34 The current study has thus far the largest sample size of IBS patients undergoing a dietitian-taught LFD in Asia. Subjects in the current study were representative of local IBS patients under the routine care of gastroenterology and dietetics at a tertiary hospital in Singapore. We, therefore, provided data on a wide range of gastrointestinal symptoms to present a fuller picture of IBS symptomology in Asia. Gas-related symptoms appeared to be a priority concern in not only the Caucasian IBS population but also in the Asian IBS patients. 10 Indeed, the most frequently reported symptoms by the current cohort were “bloating” (96.3%, n = 79), “burping or belching” (91.5%, n = 75), and “flatulence” (91.5%, n = 75). Significant improvements in these gas-related symptoms post-LFD were often observed in previous studies.19–22 In the current study, approximately 60–70% of all subjects experienced symptom improvement in “bloating” (59.7%), “burping or belching” (62.0%), and “flatulence” (70.1%). The median severity ratings of these symptoms significantly reduced post-LFD (MD = −1.0, all p-value <.001) among all subjects, and these improvements were more prominent among the adherent group (MD = −2.0 to −1.75, all p-value <.001). Our findings suggested that LFD was associated with a reduced severity in gas-related IBS symptoms in the Asian IBS cohort.
We investigated seven symptoms related to disordered bowel habits. The severity of “diarrhea,” “alternate solid/loose stools,” and “bowels open frequently with pain” improved significantly post-LFD (all MD = −1.0, p < .05), while “constipation,” “stools appear frequently hard,” “bowels open with incomplete emptying,” and “fatty greasy stool” did not. The LFD intervention appeared to be associated with reduced severity in diarrhea-related symptoms in the present study. The lack of improvement in constipation was also observed in the past. 19 Theoretically, methane production from intestinal bacterial fermentation of FODMAPs slows down gastrointestinal transit, which increases the risk of constipation. Hence, a reduction in dietary FODMAPs should lessen methanogenesis, thus alleviating constipation. 35 However, two possible factors may counteract this benefit. First, a reduction in dietary FODMAP intake could simultaneously reduce luminal osmotic fluid, which may increase the risk of forming hard stools. Second, FODMAP restriction could potentially lead to an incidental reduction in dietary fiber intake, especially when those high-fiber food items in patients’ usual diet were not replaced by suitable low-FODMAP alternatives. Unfortunately, this hypothesis could not be tested in the current study due to a lack of data on dietary fiber intake. Future prospective studies could consider more thorough dietary data collection for quantitative analysis.
Existing Western studies reported an overall 52%–86% symptom response to the LFD,19,21,36 whereas two Asian studies found a symptom improvement rate of 60% 33 and 68.8% 32 post-LFD, respectively. In the current study, we found a comparable improvement rate (46.9%–72.2%) in each symptom among all subjects. As expected, the symptom improvement rates were higher in the adherent than the non-adherent group, and these differences were statistically significant in 10 out of 19 symptoms (67.5%–82.4% vs 27.8%–55.0%, p < .05). This trend was consistent with an earlier study that reported a higher symptom improvement rate in the adherent than non-adherent patients (85% vs 36%). 17 Due to a lack of standard definition of adequate symptom response, the research team arbitrarily determined the definition of symptom improvement in the current study based on previous literature and clinical observations. An earlier study defined symptom improvement by a 50 out of 500 score reduction (10%) on an IBS severity scoring system (IBS-SSS). 37 Other studies recognized a responder to LFD by a reduction of 10 mm 20 or 20 mm 38 on a 100-mm visual analogue scale. The U.S. FDA recommended a responder definition for drug development as a ≥30% reduction in pain intensity. 39 In the current study, we defined the symptom improvement as a ≥1 point reduction on the 11-point severity rating scale, which was equivalent to at least 10% severity reduction from baseline and was comparable with some previous studies.20,37,40 However, a universally agreed definition of significant and clinically meaningful symptom improvement should be established to facilitate standardized comparison across studies in the future.
Previous Western studies reported adherence rates to LFD ranging from 75.6% to 80.0%,17,20,22 while an Asian study reported adherence in 50% of participants. 32 Since the definition of LFD adherence varied widely between previously published studies, comparison across studies could be difficult. In the current study, 61.0% (n = 50) of all subjects were assessed adherent to LFD. Several factors might have contributed to a relatively lower adherence rate. First, subjects in the current study had to spend more time and effort on food selection and meal preparation in real life than being provided with low-FODMAP daily meals in a controlled research environment. Second, the subjects in this retrospective study may not be as motivated to follow the LFD as those research participants who were actively recruited in prospective trials. Perhaps, those who were non-adherent to LFD felt less motivated, thus postponing follow-up appointments. The adherent subjects attended the follow-up dietitian visits significantly earlier than the non-adherent ones in the current study (median 35 vs 43 days, p = .032). Third, the delivery of LFD consultation could be affected by the time limit in the outpatient clinic and the initial learning curve of individual dietitians. However, the dietitian-taught LFD was a more accurate reflection of its clinical effectiveness in real-life scenarios. Our preliminary findings confirmed the feasibility to implement LFD in the routine clinical settings of Asian countries. Learning from current experience could help improve future trials.
We also explored barriers to LFD adherence experienced by the local Asian IBS cohort. “Limited availability of low-FODMAP alternatives” was the most frequently reported difficulty. Similarly, a previous Danish study reported low-FODMAP foods was costly and difficult to find in stores. 41 In Singapore, certain low-FODMAP food products, for example, lactose-free products, may only be available at high-end supermarkets or specialty food stores. Besides, subjects might fail to recognize some low-FODMAP items as the local products were not explicitly labeled “low-FODMAP.” Although the subjects were educated on label-reading skills, it could still be troublesome for them to scrutinize every ingredient listed on food packages. Furthermore, choosing suitable dishes when eating out appeared to be equally challenging. This barrier was also reported in an earlier study. 17 Similar to many other Southeast Asian cuisines, high-FODMAP ingredients, such as onion, garlic, and shallots, are used in most local dishes. 42 Besides, local restaurants and eateries have not yet progressed to become FODMAP-friendly. It might be inconvenient or even socially awkward for one to specifically request an individual serving cooked without certain high-FODMAP ingredients. Last, since there was a lack of complete food composition data on the FODMAP content of all Asian foods, a stricter elimination approach was adopted by the dietitians in the current study. Apart from the known high-FODMAP foods, subjects were advised to abstain from local Asian food items that had not yet been tested for their FODMAP content. This stricter approach might have potentially increased patients’ perceived difficulties in following the LFD since it could further limit their food choices.
“Limited understanding of LFD” and “perceived no benefit of LFD” were also reported as common reasons for non-adherence in the current study. Although low health literacy has been a suggested barrier to LFD implementation in South Asia, 43 we should also admit that the FODMAP restriction is a rather complex concept for non-professionals to understand. There are several subgroups of short-chain carbohydrates under the collective term of FODMAP, including fructose, lactose, fructans, fructo-oligosaccharides, galacto-oligosaccharides, and polyols. Possibly not all but just one FODMAP subgroup or a combination of some might trigger symptoms in each IBS patient. Each patient’s tolerance threshold to different FODMAPs could be different. The time required for symptom improvement from FODMAP restriction may also vary between each individual. Therefore, the subjects might experience a certain level of confusion, uncertainty, and lack of confidence with the LFD concept. Without fully understanding the purpose of LFD, some individuals might decide to only restrict certain FODMAP subgroups selectively or breach the diet restriction too frequently.
We acknowledge that this study had several limitations. The potential placebo effect could not be eliminated due to a lack of a control group, randomization process, and blinding in this retrospective study, which may increase the risk of false-positive findings. Besides, information on some potential confounders, such as changes in medications or psychological interventions during the LFD intervention period, was not available at the time of data collection, which may introduce further bias. Similarly, there was insufficient information on IBS subtypes to allow further subgroup analysis in this study. Last, the gastrointestinal symptom rating scale used in our study was not initially designed for research use, but as part of the routine clinical assessment for IBS patients seen in the dietetic outpatient clinic. This symptom rating scale was tailored to but not validated in local IBS patients. Since not every individual experienced all 19 gastrointestinal symptoms listed on the rating scale, many subjects did not provide severity ratings for all symptoms. Thus, this study could only evaluate changes in symptoms based on the number of subjects who had completed symptom ratings both pre- and post-LFD. Hence, study results should be viewed as indicative but not conclusive.
In conclusion, this study investigated the effects of a dietitian-taught LFD on gastrointestinal symptoms in Asian IBS patients. Most symptoms significantly improved in all subjects and LFD-adherent subjects. More LFD-adherent subjects improved in individual symptoms than the non-adherent subjects. Difficulties in accessing low-FODMAP alternatives and understanding the LFD concept were the main barriers to adherence among the local cohort. Prospective trials could consider better stratification of IBS subtypes and explore possible strategies to improve dietary compliance. Future directions of research on LFD in Asia include FODMAP content analysis of local Asian foods, the validation of IBS subtype-specific symptom measurement tools, and the development of standardized assessment tools for LFD adherence.
Supplemental Material
sj-pdf-1-psh-10.1177_20101058211051430 – Supplemental Material for Investigating the Role of Low-FODMAP Diet in Improving Gastrointestinal Symptoms in Irritable Bowel Syndrome
Supplemental Material, sj-pdf-1-psh-10.1177_20101058211051430 for Investigating the Role of Low-FODMAP Diet in Improving Gastrointestinal Symptoms in Irritable Bowel Syndrome by Jiahong Yang, Gina Ziruo Lin, Xiao Ying Li, Yu Tien Wang and Yet Hua Loh in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
The authors would like to thank Mr Lee Boo Tan (Department of Dietetics, Singapore General Hospital) for his assistance in data extraction and anonymization.
Author contributions
All authors conceptualized and designed the study. J.Y. and G.Z.L. collected data, performed statistical analysis, and wrote the first draft of the manuscript. All authors critically reviewed the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author.
Ethical approval
Ethical approval for this study was obtained from SingHealth Centralised Institutional Review Board (reference number: 2014/951/F).
Informed consent
Informed consent was waived for the present study due to its retrospective nature.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.