
Abstract
Temporomandibular disorders are a multifactorial disease. Occlusal support and the number of teeth in dentition have significant effects on the masticatory system. The current study aims to review the role of occlusal support in association with findings of temporomandibular disorders. Data sources were PubMed, Web of Science and Google Scholar, with 1411 citations published over the period 1992–2019. The selection criteria stipulated that articles must have reported the association between the number of teeth, occlusal unit, occlusal support and temporomandibular disorders. A total of 15 full-text articles was finally accessed for eligibility in the current review. The studies on temporomandibular disorders were collected from various sources, including articles reporting temporomandibular disorder symptoms (n=1), temporomandibular disorder signs (n=5), temporomandibular joint osseous changes (n=1), temporomandibular joint dysfunction using the Helkimo index (n=2), and temporomandibular disorder classification (n=6). Of these articles, significant associations were found between: the number of missing teeth and temporomandibular disorders (n=5); the number of occlusal units and occlusal supports and temporomandibular disorders (n=3); the position of the lost occlusal units and temporomandibular disorders (n=1). Loss of the occlusal unit has more impact on temporomandibular disorders than the loss of posterior teeth. The total loss of unilateral occlusal support seems to be an aetiological factor for temporomandibular disorders, and maintenance of balanced posterior occlusal support has a role in the prevention and management of temporomandibular disorders.
Introduction
According to medical subject headings (MeSH), temporomandibular disorders (TMDs) are classified as musculoskeletal diseases and stomatognathic diseases. TMDs are defined as a variety of conditions affecting the anatomical and functional characteristics of the temporomandibular joint (TMJ).1,2 The prevalence of TMDs among the general population varies widely depending on age, gender and diagnosis classification; however, the peak of TMDs is affirmed to be at middle age.3–6
TMDs are grouped into muscle disorders and TMJ disorders. In a non-patient population, masticatory muscle pain occurs in 3–25%,7–10 while disc displacement ranges from 7.0% to 37.6%.7,8,11 TMJ degeneration is present in 5.1–34.6% of the general population and is an age-related disease.7,8,12 The degenerative joint disease is of non-inflammatory origin; progressive degeneration causes osseous changes to the TMJ such as erosion, flattening, osteophytes, sclerosis and subchondral cysts.12–14 TMDs have an adverse impact on oral health-related quality of life and daily activities, even in asymptomatic TMD individuals.15,16
In addition to pain, TMD patients often seek treatment because of impaired mastication. Missing teeth is the main cause for the impairment of mastication and may affect TMDs, but studies have indicated that the number of missing posterior teeth is not associated with TMDs.17–22 The first reported occlusion and TMD was published by Granger in 1958; 23 however, the debate as to the relationship with occlusion, the number of teeth and TMDs has been inconclusive. 24
The functional tooth unit or occlusal unit is used to describe the number of posterior occluding pairs of teeth and is significant in determining masticatory efficiency and chewing ability. Maintaining good oral function depends on the number of functional tooth units.25,26 Previous studies have indicated that asymmetric loss of posterior occluding pairs can influence habitual chewing patterns and increase signs and symptoms of TMDs.20,27–29 Therefore, loss of functional tooth units or occlusal units inducing changes in oral function may be considered risk factors for TMDs.
Occlusal support creates balanced occlusion and maintains the stable vertical dimension of occlusion. Loss of occlusal support causes changes in craniofacial structures. People without occlusal support tend to have pseudo-prognathism to adapt their mastication; 30 and this parafunction can affect neuromuscular adaptation and influence the position of the TMJ condyle in the glenoid fossa. However, numerous studies have indicated that occlusal support and TMDs were weakly correlated because the stomatognathic system and motor function can adapt to lost occlusal support.31–34
Restoration of occlusal support is the core task in the field of dentistry to create the harmony of oral function and prevent TMDs for patients. 31 However, TMDs have multiple aetiology factors, and the association of occlusal support and TMDs is not conclusive. Therefore, the aim of the current study was to review the impact of occlusal support as well as loss of teeth on TMDs.
Methods
Search strategy
We selected relevant articles that reported findings on occlusal support, number of teeth and TMDs. In 1992, the research diagnostic criteria for temporomandibular disorders was developed and has since been widely used as a frame of reference in clinical and epidemiological studies of TMDs. The selected articles were based on a computerised data search on Web of Science, Google Scholar and PubMed published from January 1992 to December 2019. For the search terms in Web of Science and Google Scholar, the keywords ‘temporomandibular disorders’ and ‘temporomandibular dysfunction’ were used in combination with keywords evaluating occlusal support: ‘tooth loss’, ‘lost teeth’, ‘missing teeth’ and ‘occlusal support’. Also, the key term ‘Eichner’s classification’ was used to determine the number of posterior occlusal supports (Figure 1). The query in the PubMed search system was the following:
((Temporomandibular disorders [MeSH]) OR (temporomandibular dysfunction [MeSH]) OR (craniomandibular disorders [MeSH] )) AND
((Eichner [Title/Abstract]) OR (tooth loss [Title/Abstract]) OR (lost teeth [Title/Abstract]) OR (missing teeth [Title/Abstract]) OR (occlusal support [Title/Abstract])).
Study selection criteria for this review were that articles be published in English and target participants over 15 years old. Excluded articles consisted of duplicated publications, systemic reviews, case reports and updated or overlapping research by the same authors. In addition, articles reporting trauma or fracture of the craniomandibular structure, TMJ surgery, or participants using dental prostheses were also eliminated.

Number of occlusal supports according to Eichner’s classification.
Systematic assessment of articles
The article selection process was implemented according to the evidence-based medicine guidelines of the PICO model, requiring articles to have all four components: P (patient, population, or problem), I (intervention, prognostic factor, or exposure), C (comparison or intervention) and O (outcome).
Selected articles had the P component addressed to the population study gathering information on temporomandibular disorders and occlusion of the non-TMD and TMD group. The I component contained characteristic information of TMDs such as signs, symptoms, classification and level of TMD. Regarding the number of teeth and occlusal support, the criteria selection was a number of missing teeth, present teeth, functional tooth unit, occlusal unit and occlusal support. The C component reported data on loss of teeth and occlusal support in the TMD group and comparison with the non-TMD group. Finally, the O component had to show statistical methods to analyse the association between TMDs and the number of teeth and occlusal support.
Quality assessment of articles
The weighting criteria for article selection were based on the Newcastle–Ottawa scale. A total of nine stars was delivered for quality assessment, with four for an adequately selected sample, two for comparability of cases and controls on the basis of the design and analysis and three for outcome of the adequate ascertainment of the exposure (number of teeth, occlusal unit and occlusal support) in both the case and control groups. Articles were quality assessed by four independent reviewers. Three members of the evaluation team selected titles and abstracts for full-text reading based on the database searches. Next, each reviewer independently gave star scores and rated the quality of these articles. When reviewers disagreed about the scoring of a selected article, the last reviewer would contribute a tie-breaking score. The quality of the study was assessed with 8–9 stars for high, 5–7 for medium and others for low quality.
Results
Search results
The preliminary search identified 1411 citations from the Web of Science, Google Scholar and PubMed databases. A total of 188 abstracts was recorded for eligibility when applying limits and checking duplication. Among the selected abstracts, 157 of those did not meet the inclusion criteria and 31 abstracts were screened for full-text reading. The reviewers agreed to eliminate 16 articles (of 31 selected full-text articles) for reasons listed in Table 1.9,13,27,31,35–48 A total of 15 full-text articles was ultimately included in the current review (Figure 2).
Excluded articles after full-text reading.

Articles listed in alphabetical order of the first author.
CI: confidence interval; OR: odds ratio; TMD: temporomandibular disorder; TMJ: temporomandibular joint.

Search strategy of full-text articles.
Study findings
Nine articles (n=9) were cross-sectional designs that studied non-TMD patient populations and the remaining studies (n=6) were case–control designs. The findings of TMDs among the 15 articles included: TMD symptoms (n=1), TMD signs (n=5), TMJ osseous changes (n=1), Helkimo dysfunction index (n=2) and diagnosis classification of TMDs (n=6). Reports of occlusion among the selected articles consisted of the number of present teeth (n=5), loss of teeth (n=5), loss of occlusal units (n=2), loss of occlusal support (n=5) and position of lost occlusal units (n=2). Because of the inconsistency between studies, a meta-analysis of data could not be used to analyse outcomes.
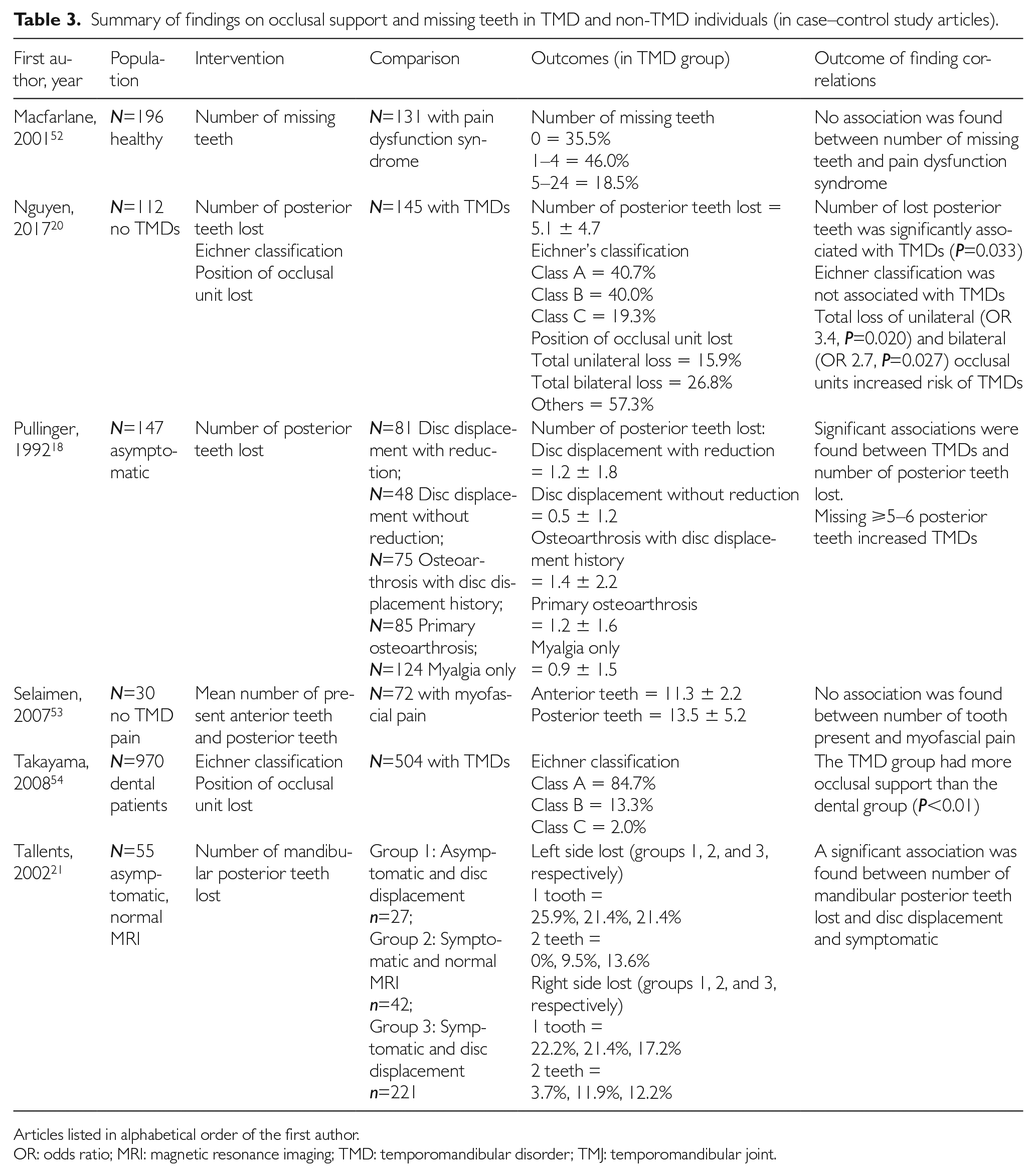
Tables 2 and 3 show the detailed findings concerning the number of teeth and occlusal support among the TMD samples.49–54 Among those suffering TMD signs, 17.5–52.2% of patients had less than 20 teeth and 10.9–34.3% had edentulousness.34,51 TMD sufferers lost an average of 0.5–5.1 posterior teeth, and 33% of TMD patients had lost more than five posterior teeth.17,18,20 Using Eichner’s classification, the highest prevalence of class C (no occlusal support) was found in 77.2% of individuals having TMJ dysfunction, 38 followed by 23.8–32.4% of muscle and TMJ tenderness, 41 20.3% of limited mouth opening 32 and 19.3% of TMD diagnoses. 20
Summary of findings on occlusal support and missing teeth in TMD and non-TMD individuals (in cross-sectional study articles).

Articles listed in alphabetical order of the first author.
OR: odds ratio; TMD: temporomandibular disorder; TMJ: temporomandibular joint.
Summary of findings on occlusal support and missing teeth in TMD and non-TMD individuals (in case–control study articles).
Articles listed in alphabetical order of the first author.
OR: odds ratio; MRI: magnetic resonance imaging; TMD: temporomandibular disorder; TMJ: temporomandibular joint.
Regarding the methods of statistical analysis, five studies used logistic regression to determine TMD risk due to loss of teeth and occlusal support. Three case–control studies indicated an association between loss of posterior teeth and TMDs (odds ratio (OR) range 2.0–3.7).18,20,21 One article reported a significant association between lost occlusal units and TMD symptoms. 49 A reduced number of teeth was significantly associated with decreased mouth opening of less than 40 mm, TMJ tenderness and muscle tenderness, and a severe level of TMDs;34,51 but it was not correlated with pain dysfunction syndrome, TMJ osseous changes and diagnosis classification of TMDs.14,52,53 Loss of occlusal support resulted in muscle tenderness 50 but did not associate with TMJ sounds, TMJ dysfunction, or diagnosis classification of TMD.20,32,38 Two articles indicated the effect of the position of the lost occlusal unit on TMDs (Table 4).19,20
Summary findings on occlusal support, number of present teeth and number of teeth lost in association with TMD characteristics (first author, age of participants in study).

No statistical significance.
Statistical significance.
TMD: temporomandibular disorder; TMJ: temporomandibular joint.
Quality and risk bias assessment
Two studies were scored as high quality,50,52 13 articles as medium quality,14,17–21,32,34,38,49,51,53,54 and none as low quality. Across studies, the main bias related to exposure measurement was the exact number of missing teeth. Age was also a factor contributing to risk bias for the current review. An age group of 15–18 years was reported in two studies, 19–60 years in eight studies and 60+ years in five studies (Table 4).
Discussion
The total number of teeth lost indirectly affects TMDs
The main finding of our review is that the maintenance of occlusal support significantly contributes to preventing TMDs. To improve dental arch deficiency is a main task for dentists, and comprehensive occlusion also contributes to the management of TMD prevention and treatment. The current review gathered 15 articles investigating the association of the number of teeth and occlusal support with findings related to TMDs. Of these, eight (53.3%) found a significant association, while the others indicated conflicting results.
We found that the probability of having TMDs was not significantly different among tooth loss categories. Our finding is supported by previous literature in which no conclusion has been made about tooth loss aggravating the extent of TMD signs and symptoms. 55 This is due to the influence of the bias factor of age. For instance, no association between the number of teeth lost and TMDs was found among studies with wide age ranges,17,52,53 but when focusing on older age groups, a statistically significant tendency between the number of teeth lost and TMDs was found.20,32
In the current review, we found that the prevalence of TMDs among persons with less than 20 teeth was 27.6–86.5%,32,34,51,52 but no studies confirmed that having fewer than 20 present teeth caused TMDs. Missing teeth influences not only aesthetics, but also oral function. The World Health Organization recognises the necessity of maintaining 20 or more natural teeth throughout human life. In other words, having 20+ teeth would create a balance of occlusion to maintain masticatory performance. Ueno et al. 25 found that the number of functional tooth units of individuals with more than 20 natural teeth was 2.4 times more than of those with less than 20 natural teeth. This suggests that the total number of lost teeth might influence oral function and indirectly affect TMDs.
Loss of occlusal units affects TMDs more than loss of posterior teeth
A posterior occluding pair of natural teeth creating one occlusal unit (for a premolar pair) or two occlusal units (for a molar pair) has functions of mastication and stable occlusion, and when a posterior tooth is lost its antagonist becomes dysfunctional; therefore, the number of occlusal units lost might be more important than the number of teeth lost. Previous studies have indicated an impact of occlusal units lost on TMDs.18,20,21,47,49 Using multiple regression, Pullinger et al. 18 found that the increase in probability of having TMJ osteoarthrosis from 1.2 to 2.0 correlated with the loss of two to five posterior teeth. In many cases related to lost molars, loss of two to five posterior teeth was equivalent to loss of four to nine occlusal units. Wang et al. 47 emphasised that the greater the number of dental quadrants missing posterior teeth, the greater the risk of developing TMDs (OR 7.71); in other words, the number of occlusal units lost and TMDs were strongly correlated. A study conducted on the general adult population aged 18–75 years using a TMD symptom-related questionnaire assessed the risk of difficulty in closing the mouth among persons having more than eight occlusal units lost. This suggested that there were structural changes inside the TMJs because of an altered distribution of functional and parafunctional loads. 49 Findings in the study by Nguyen et al. 20 reported that the number of maxillary posterior teeth of TMD individuals was similar to those of healthy individuals; however, the TMD group had more missing mandibular posterior teeth than the healthy group. A similar finding indicated a crude OR of two missing mandibular teeth per side in a TMD individual with disc displacement of 3.7–6.7. 21
Loss of occlusal units causes impairment of masticatory performance and bite force that were prevalent in TMD patients.27,56,57 However, whether loss of occlusal units causes TMJ dysfunction is still not clear because some studies have reported that individuals lost occlusal units but did not have TMDs.19,58 It is possible that a comorbid factor related to the loss of occlusal units may be an aetiological factor for TMDs.
Total loss of unilateral occlusal support seems to be an aetiological factor for TMDs
If the lost occlusal units coincided in one region (i.e. the premolar or molar region on one side of the dental arch), it would cause the loss of the occlusal support zone. The laterotrusive movements of the mandible are the bi-contraction of the ipsilateral temporalis and contra-inferior pterygoid muscle. Hence, the corresponding muscle might be functionally altered when unilateral occlusal support is lost. Schmitter et al. 9 confirmed that non-occlusion on at least one side accelerated myofascial pain 4.2 times more than having occlusal contacts on both sides. Supporting the study of Schmitter et al., 9 findings from our previous study 20 reported that the total loss of unilateral occlusal support increased the risk of TMDs 3.4 times. Moreover, TMJ sounds were reported more often in individuals with unilateral posterior support. 19 The absence of balance-side contact of occlusion positively correlated with TMJ sounds; hence, maintaining balance-side contacts could protect against TMDs. 59 An absent unilateral contact also influenced the condylar position in the glenoid fossa. A tomographic study found reduced posterior condylar space among subjects with lost unilateral extension of the posterior teeth. Such reductions caused overload on the condyle or articular disc and had adverse effects on biomechanical loading-related TMs.60,61
In experiments on chewing patterns, chronic unilateral chewing was more often significantly associated with TMDs than other chewing patterns. 27 Based on the findings of TMJ condylar path among participants having TMDs, Santana-Mora et al. 29 suggested that a new term, ‘habitual chewing side syndrome’, should be added to TMD diagnosis. The TMJ disc has the ability to adapt to the alteration of the space between the condyle and fossa caused by occlusal changes. 62 The bone metabolism of TMJ and histochemical aspects of masticatory muscles seem to be associated with occlusal alterations due to unilateral missing teeth. As unilateral extracted teeth increase interleukin 1β,63,64 which is known as an important mediator of the inflammatory response occurring in TMJs.65,66
Eichner class B2 guarantees for masticatory performances; in other words, there is a significantly reduced mastication from occlusal contacts of the bilateral premolars to only occlusal contacts of the unilateral premolars. 67 Having impaired mastication influences general and mental health, lowers quality of life and limits daily activities that might be correlated with TMDs. Therefore, preservation of bilateral contacts of premolars can prevent TMDs; in turn, only unilateral occlusal contacts seem to be an aetiological factor for TMDs.58,68
Does no occlusal support provoke TMDs?
Numerous articles using Eichner’s classification have shown that reducing occlusal support induces TMD problems. In the current review, a high prevalence of class B4 and class C was found in cases having severe TMDs (77.2%), muscle tenderness (28.1%), TMJ sounds (15.3%), or TMJ osseous changes (9.9%). No occlusal support provokes functional alterations in the TMJ structures. The risk of muscle tenderness is often found among individuals without occlusal support. Mundt et al. 50 showed that Eichner class B4 and class C increased the risk of muscle tenderness 2.7–3.9 times more than class A. Similar findings have been reported by Nguyen et al. 20 and Yekkalam and Wänman, 48 who concluded that total loss of bilateral occlusal support increases the risk for limited mouth opening (OR 2.2) and TMDs (OR 2.7).
This could be explained by the fact that mandibular protrusion for adaptive mastication occurs in cases of lacking posterior occlusal supports. Such changes would induce excessive muscular tension, triggering facial pain. 69 In edentulous individuals, a significant increase in muscle pain was found in both men and women.6,41,51 This may be because of the impairment and fatigue of masticatory muscles. Lack of posterior supports affects lateral pterygoid muscle tenderness, and the probability of masseter muscle tenderness can be 64% after 5 years of being edentulous.36,70
The absence of bilateral occlusal support would change the position of the TMJ condylar head in the mandibular fossa and cause loss of the occlusal centric relationship. Significant associations between TMDs and centric occlusion have been reported in previous studies.9,17,24,53 In addition, individuals without posterior occlusal support tend to experience temporary occlusal contact in the anterior tooth region. The higher the number of lost occlusal support zones, the more significant the changes to craniofacial structures. 30 This could cause variation in condyle–fossa relationships; eventually, in cases of edentulous jaws, the condyle would be situated upwards and forwards within the glenoid fossa. 71 Such variations create pressure on the articular disc and inflame articular surfaces, probably leading to degeneration of the joint. 12
Total loss of occlusal support can progress to edentulousness if any teeth have not been reserved. We assumed that if edentulousness was significantly associated with TMDs, the prevalence of TMDs would have increased more among the edentulous population than among the dentate population. However, there have been conflicting results about the rate of TMDs among these populations. Katyayan et al. 34 found that the prevalence of severe TMJ dysfunction among those with edentulousness (8.8%) was higher than that among dentate persons (2.6%), while the prevalence of TMDs among the edentulous and dentate populations were 10.6% and 34.6%, respectively, in the study by Takayama et al. 54 and a similar prevalence was reported in the study by Dervis. 33 Sipilä et al. 51 found that edentulousness was associated only with limited mouth opening and muscle pain in women, but that edentulousness actually reduced the risk of TMJ crepitus in men. This is because no pressure was placed on the TMJ condyle by occlusion. As TMDs occurred, TMJ signs could be stable with time and concurred with TMJ remodelling.
In the current review, we have given a hypothesis model for the tooth loss–TMD correlation (Figure 3). It is known that the number of lost teeth increases with age, whereas the peak of TMDs is in the middle age group among the general population. The line of tooth loss can cut the parabolic shape of TMDs at certain ages; therefore, a significant correlation between tooth loss/loss of occlusal support and TMDs can be identified when the cases drop below this line whereas no association has been found eventually in edentulous cases. The hypothesis model could explain why there have been different results in previous studies about the association between tooth loss and TMDs among the general population. Any risk factors simultaneously causing changes to the tooth loss line and TMD parabolic shape would influence tooth loss–TMD association.

The hypothesis model between tooth loss and TMD correlation among the general population. Line AB: Tooth loss occurred but was not associated with TMDs; line BC: Tooth loss and TMDs were significantly associated; line CD: increased tooth loss and eventual edentulousness was weakly correlated with TMDs. TMD: temporomandibular disorders.
Conclusions
The present study concludes that the loss of occlusal units might have more impact on TMDs than the loss of posterior teeth; furthermore, total loss of unilateral occlusal support seems to be an aetiological factor for TMDs. The maintenance of balanced posterior occlusal support has a significant role in the prevention and management of TMDs.
Footnotes
Acknowledgements
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Authors’ contributions
MSN collected the data, interpreted the results and prepared the manuscript. MS, TJ and QHN collected the data and edited the manuscript. UVO interpreted the results and approved the manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Ethical approval
The Danang University of Medical Technology and Pharmacy and the University of Tartu only need ethical approval in case of patients’ sensitive data are involved in the study.