
Abstract
Purpose
Metastatic pituitary neuroendocrine tumors (PitNET) are exceedingly rare tumors that are typically diagnosed at the time of metastasis. Given the rarity of metastatic PitNET tumors, the pattern of metastasis and imaging appearance of CNS and extra neural metastasis is under reported and poorly understood.
Methods
In this retrospective case series, we present 14 consecutive patients with pathology-confirmed metastatic PitNET tumors. We assess imaging features of primary pituitary disease at the time of diagnosis, temporal evolution of local disease, and distant metastasis on multimodality imaging. We also explore potential association of initial pathology diagnosis and time to metastasis and survival.
Results
At the time of metastasis, nine patients had evidence of disease in the sella and three additional had evidence of disease in the cavernous sinus. The most common site of metastatic disease was the CNS (78.6%). Dural deposits were the most common brain CNS metastatic disease manifestation (81.8%). Eight patients (57.1%) demonstrated multiple metastatic disease sites, with five of them (62.5%) showing both CNS and extra CNS metastases. Osseous metastatic disease was the most common extra CNS disease site (75.0%). Median time to metastasis did not significantly differ between patients with adenoma and those with more aggressive pathologies at initial diagnosis (p value = .39). Similarly, median overall survival from metastasis detection was not significantly affected by pathology (p value = .84).
Conclusion
Metastatic PitNET is a rare neuroendocrine neoplasm. In the present case series, we detail temporal imaging findings of the disease at the primary site and patterns of metastasis.
Introduction
Pituitary adenomas are considered the third most common primary brain tumor with a reported overall prevalence of 16.7%, rising to 22.5% in imaging studies.1,2 Furthermore, the incidence of pituitary adenomas has been reported to be increasing. 3 Pituitary carcinomas, however, are exceedingly rare and represent 0.1%–0.5% of pituitary tumors.3–7 In a review of SEER database between 2004 and 2016, Chen et al. reported 39 pituitary carcinomas in a total of 47,180 pituitary tumors, showing a prevalence of 0.08% among pituitary tumors. 8
Pituitary tumors, like other endocrine and neuroendocrine tumors, have undergone significant reclassification in the fifth edition of the WHO tumor classification system.9,10 Pituitary adenoma is now termed pituitary neuroendocrine tumor (PitNET) and no longer defined as benign. PitNETs are now classified by transcription factor lineage, which correlates with hormonal staining. Pituitary adenoma/pituitary carcinoma terminology convey the idea that there may be a feature in the sellar component of tumor that differentiates the 2: adenoma versus carcinoma. However, no feature of the pituitary tumor is definitively diagnostic of a tumor that will metastasize. Therefore, the previously termed pituitary carcinoma is now known as metastatic pituitary neuroendocrine tumor (PitNET).9–12 There are histologic features which may identify a more aggressive PitNET but do not definitely diagnose a PitNET that will metastasize. Imaging features of PitNET such as tumor growth rate and invasiveness correlate with more aggressive tumors though they do not entirely predict metastasis.
In this case series of 14 patients diagnosed with pituitary carcinoma, before reclassification as metastatic PitNET, we present imaging findings the sellar PitNET / pituitary adenoma and of the metastases.
Case series
Methods
This retrospective study was approved by the Institutional Review Board at The University of Texas MD Anderson Cancer Center. Some of the included cases were included in prior publications from our institution.13–15 However, prior publications focused on clinical and therapeutic data while this manuscript primarily focuses on imaging data.
Patient selection and clinical data
Between the period of January 2000 and October 2024, a total of 38 consecutive patients with potential diagnosis of metastatic PitNET/pituitary carcinoma were identified and included in the initial assessment of this case series. Subsequently, 14 patients met the criteria of inclusion of this study as summarized in Graph 1. The pathology was reported using the old system of classification of pituitary adenoma as PitNET, so the old nomenclature will be used in reference to these cases. Flow chart for patient selection. Incomplete imaging refers to lack of imaging of the pituitary at the time of metastasis or lack of CNS or systemic imaging to assess for the extent of metastasis.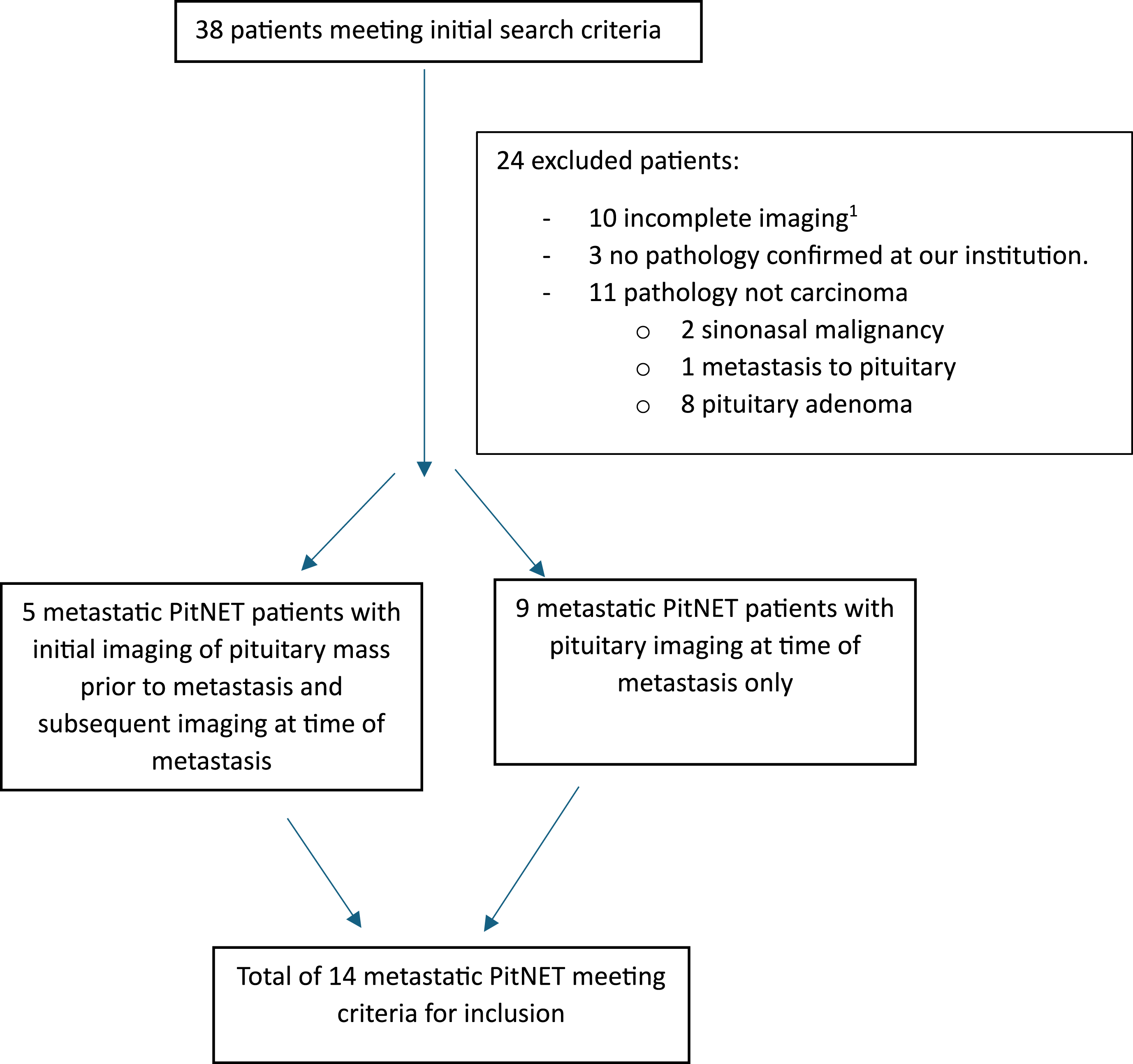
Inclusion criteria included all the following: Initial MRI showing pituitary tumor, pathology report of the pituitary adenoma or metastatic disease demonstrating pituitary origin finalized at our institution, pathological evidence of metastatic disease of pituitary/neuroendocrine origin, clinical diagnosis concordant with pituitary carcinoma, and imaging of metastatic disease.
Exclusion criteria included any of the following: Lack of MRI of the pituitary tumor, lack of pathological interpretation of the pituitary mass at our institution, lack of pathological evidence of metastatic disease of pituitary origin, lack of imaging of metastatic disease, and lack of clinical classification of the disease process as metastatic PitNET.
Clinical and pathological data review
The following clinical data were collected from each patient’s electronic medical record at the time of initial diagnosis, when available: age at presentation, sex, presenting symptoms, functional status of the pituitary tumor, pituitary hormonal lab panel, pathology interpretation of initial pituitary adenoma, and report of associated genetic syndromes.
The following clinical data were collected from each patient’s electronic medical record at the time of metastasis, when available: time from initial diagnosis to metastasis, functional status of the pituitary tumor, pituitary hormonal lab, pathology of the pituitary tumor, and pathology from site of metastasis confirming pituitary/neuroendocrine origin. Assessment of CNS metastasis was performed in the brain and spine, and categorized as parenchymal, dural, and/or leptomeningeal (LMD). The presence of extra CNS metastasis, its site(s), and character as solitary or multiple were recorded, and its temporal relationship with respect to CNS metastasis was also noted. Furthermore, any update in the pathological assessment of the pituitary mass at the time of metastasis was noted when available. Lastly, vital status and overall survival from metastatic disease diagnosis were recorded.
Imaging data review
Pituitary tumor
In cases where initial pituitary MRI was available, the following imaging data were collected. Tumor size in three dimensions (anteroposterior, transverse, and craniocaudal) was recorded in centimeters. Because invasiveness is a marker of an aggressive adenoma, the likelihood of cavernous sinus involvement was graded by the Knosp classification and was performed in consensus by two readers (RE, a fellowship trained neuroradiology attending with 6 years of experience; and HA, a second-year neuroradiology fellow with 1 year of dedicated neuroradiology experience).16,17 Additional imaging features of the initial tumor included relationship to the optic chiasm/optic apparatus, sphenoid sinus involvement, local osseous, and parenchymal involvement.
At the time of metastasis, the pituitary was assessed for residual disease. Any pituitary disease was measured in three dimensions. Assessment for cavernous sinus residual/recurrent disease was performed in similar consensus fashion. Brain and spine MRI was evaluated for the presence of dural metastasis, parenchymal involvement, and LMD. CT imaging of the chest, abdomen, and pelvis and/or PET/CT including 18F-FDG PET/CT and 68Ga-DOTATATE PET/CT were assessed for site(s) of metastasis outside the CNS.
Statistical analysis
Quantitative and qualitative variables were summarized as median (interquartile range (IQR)) and count (percent), respectively. The median time from diagnosis to metastasis and median overall survival from metastasis were computed along with their 95% CI. An exploratory, right-censored, Kaplan–Meier analysis was conducted to evaluate survival difference between patients with initial pathological diagnosis of adenomas and patients with initial pathological diagnosis of more aggressive subtypes such as atypical adenomas or neuroendocrine tumors. Survival times were compared with the Breslow test, and a p-value <.05 was considered significant.
The Barlow test was chosen for survival time comparison as it is a non-parametric test and therefore it offers a more robust analysis and comparison of survival probability distribution when compared groups are of small sample such as our case series.
Results
In total, 14 patients with metastatic PitNET met the criteria for inclusion. Five patients had available imaging of the initial pituitary tumor and subsequent imaging of pituitary/sellar and metastatic disease. Nine patients had imaging of pituitary/sellar and distant metastatic disease but no imaging of the initial tumor prior to the first surgery.
Clinical and pathological characteristics
Clinical and pathological data summary.
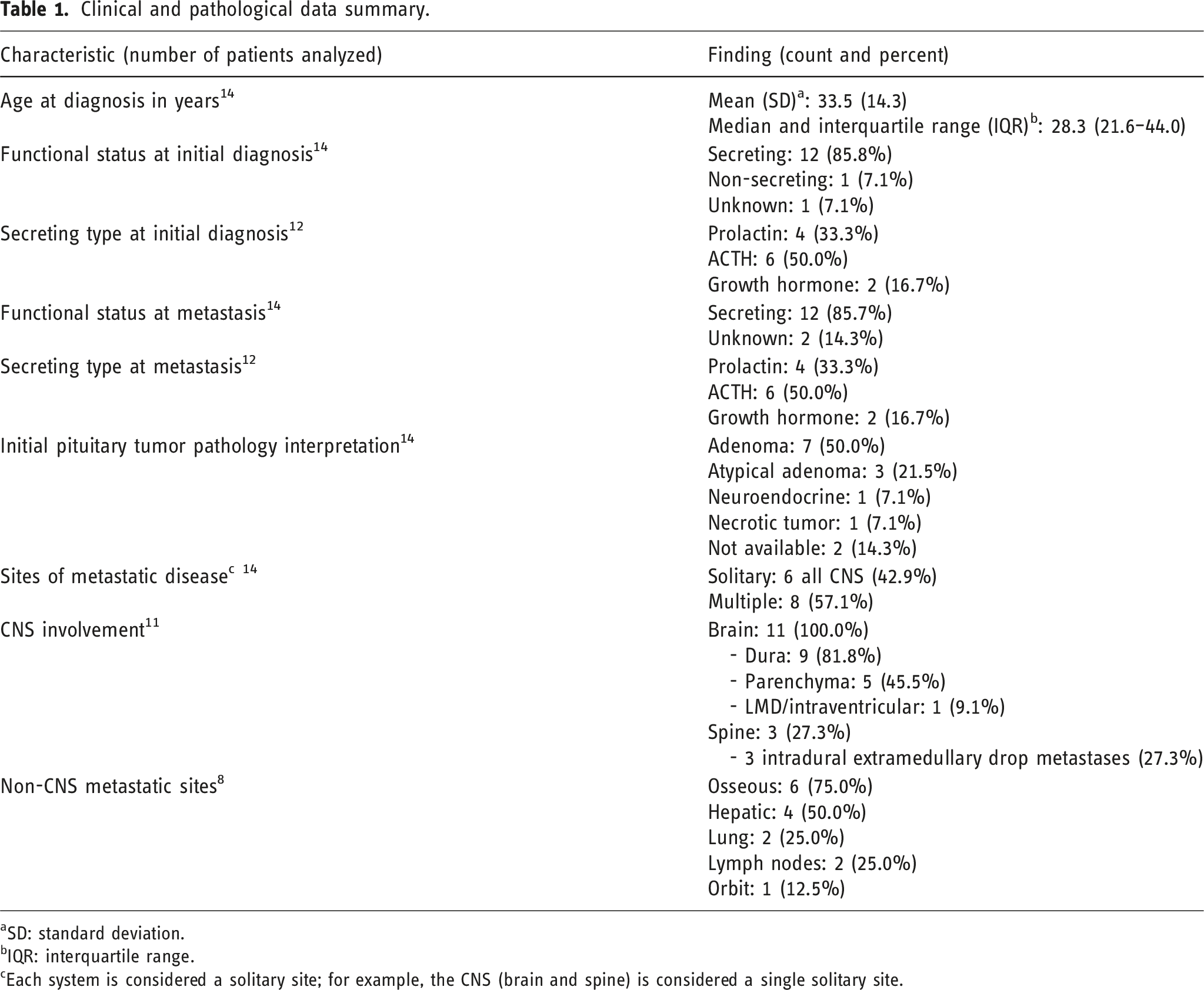
aSD: standard deviation.
bIQR: interquartile range.
cEach system is considered a solitary site; for example, the CNS (brain and spine) is considered a single solitary site.
Imaging characteristics of metastatic PitNET
Imaging characteristics summary.
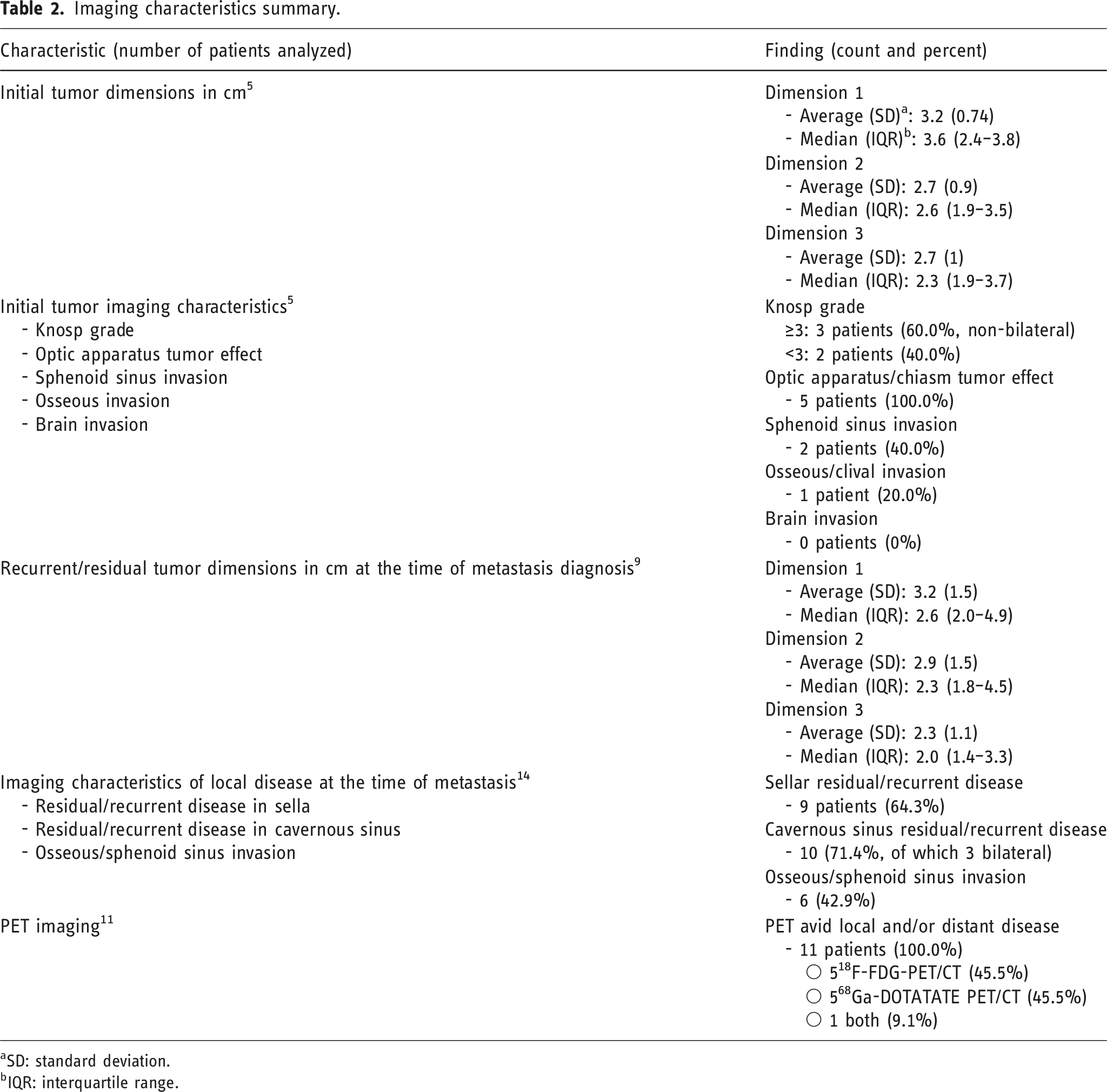
aSD: standard deviation.
bIQR: interquartile range.
Imaging of the sell/pituitary
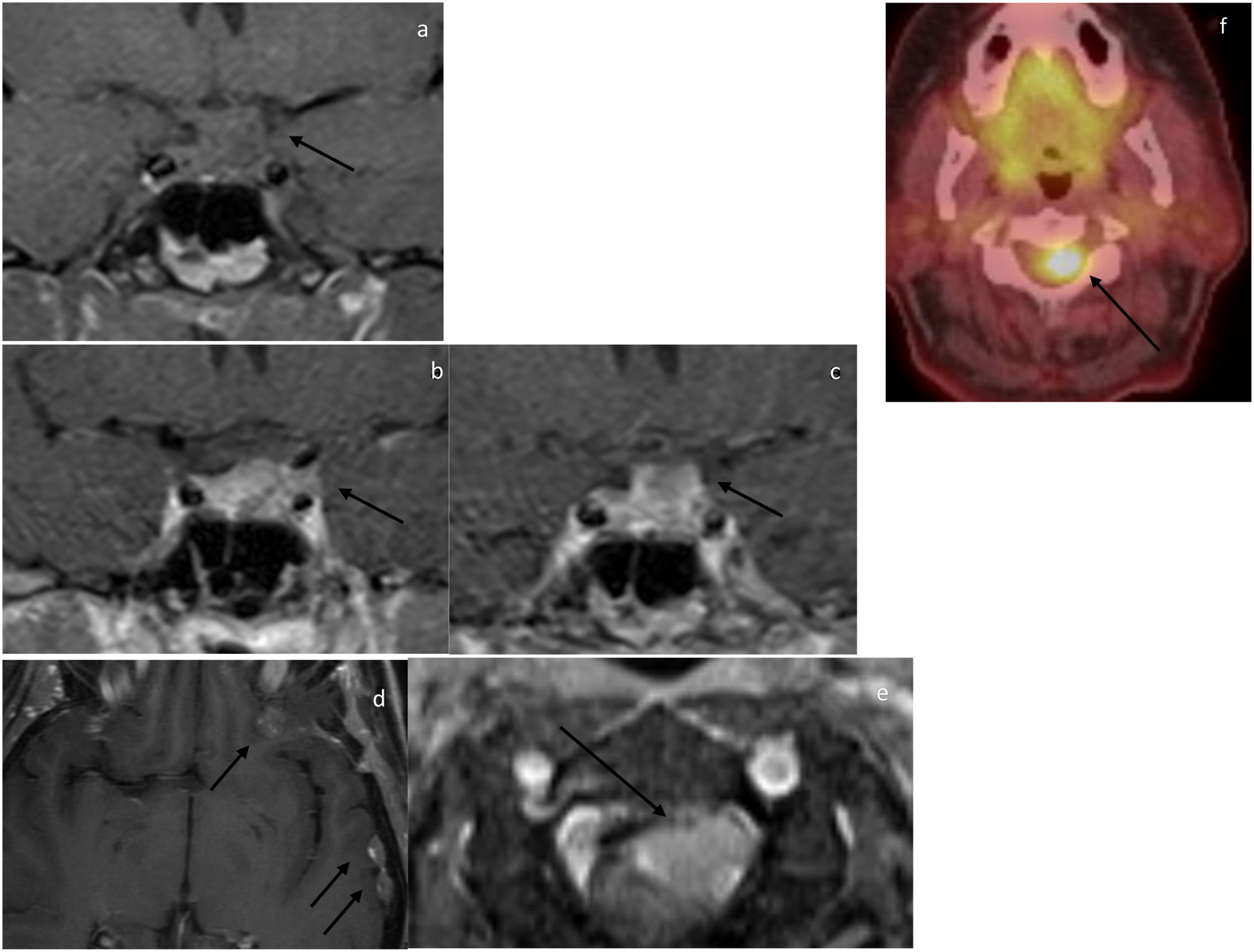
MRI of the initial pituitary/sellar tumor was present in five patients. In all five patients, the lesion demonstrated dimensions more than 1 cm in all three planes (Figure 1). Median dimensions were 3.6 cm (IQR 2.4–3.8), 2.6 cm (IQR 1.9–3.5), and 2.3 cm (1.9–3.8). Patients (60.0%) had Knosp grade of more than 3. In all those three patients, grade 3 was unilateral. In all five patients, pituitary/sellar tumor compressed the optic apparatus. Sphenoid sinus extension and osseous invasion were present in two and one patient (40.0% and 20.0%), respectively. No local brain invasion was identified. At the time of metastasis, imaging of the sellar/pituitary was present in all 14 patients. Nine patients demonstrated residual/recurrent disease within the sella/pituitary (64.3%) (Figure 2). All three dimensions demonstrated average residual disease of more than 1 cm. Median dimensions were 2.6 cm (IQR 2.0–4.9), 2.3 cm (IQR 1.8–4.5), and 2.0 cm (IQR 1.4–3.3). Of the five patients who did not demonstrate sellar/pituitary disease, three had residual/recurrent disease in the cavernous sinus (60.0%). In total, 10 patients (71.4%) had cavernous sinus disease, of which 3 had bilateral involvement (30.0%). Local aggressive extension of the disease into the adjacent osseous structure or cavernous sinus was present in six patients (42.9%). 21-year-old female presenting with visual symptoms. Figure 1(a). Sagittal T1 pre-contrast demonstrates a sellar/suprasellar mass abutting the optic chiasm and demonstrating internal intrinsic hyperintensity representing blood products or proteinaceous secretions (arrow). Figure 1(b). Coronal post-contrast T1-weighted MRI demonstrates a sellar/suprasellar tumor exerting tumor effect on the optic chiasm (arrow) with no evidence of cavernous sinus involvement. Figure 1(c). Coronal post-contrast T1-weighted MRI of the sella 5.5 years after resection of a pathologically diagnosed pituitary necrotic tumor demonstrates no evidence of residual/recurrent disease. Figure 1(d). Axial T1-weighted MRI of the brain at the same time demonstrates multiple dural deposits (arrows). Figure 1(e). Axial CT chest with contrast, lung window, demonstrates lung nodule (arrow). Figure 1(f). Axial CT abdomen with contrast, venous phase, demonstrates multiple liver metastases (arrows). Figure 1(g). Sagittal CT of the chest, bone window, demonstrates diffuse sclerotic metastasis. Figure 1(h). Axial 68Ga-DOTATATE PET/CT fusion demonstrates avid dural deposits (arrows). Figure 1(i). Sagittal 68Ga-DOTATATE PET/CT fusion demonstrates multiple PET avid osseous metastatic lesions. An osseous lesion was biopsied with pathology consistent with pituitary neuroendocrine origin, and patient was diagnosed with metastatic PitNET. 65-year-old female initially diagnosed with pituitary adenoma 5.5 years ago status post-multi-modality therapy with residual disease presenting with neurological symptoms localizing to upper cervical spine. Figure 2(a). Coronal pre-contrast T1-weighted MR demonstrates T1 isointense sellar/suprasellar mass abutting the undersurface of the optic chiasm (arrow). Figure 2(b). Coronal post-contrast T1-weighted MRI demonstrates residual disease involving the left cavernous sinus (arrow). Figure 2(c). Coronal post-contrast T1-weighted MRI demonstrates suprasellar extension and abutment of the optic chiasm (arrow). Figure 2(d). Axial post-contrast T1-weighted MRI of the brain demonstrates multiple dural deposits (arrows). Figure 1(e). Axial post-contrast fat saturated T1-weighted MRI demonstrates intradural extramedullary tumor along the left ventral aspect of the spinal cord at the level of C2–C3 compressing the spinal cord (arrow). Figure 1(f). Axial 18F-FDG PET/CT fusion of the same lesion demonstrates avidity of the lesion (arrow). Patient had resection of a T6 intradural extramedullary lesion with pathology consistent with metastatic PitNET.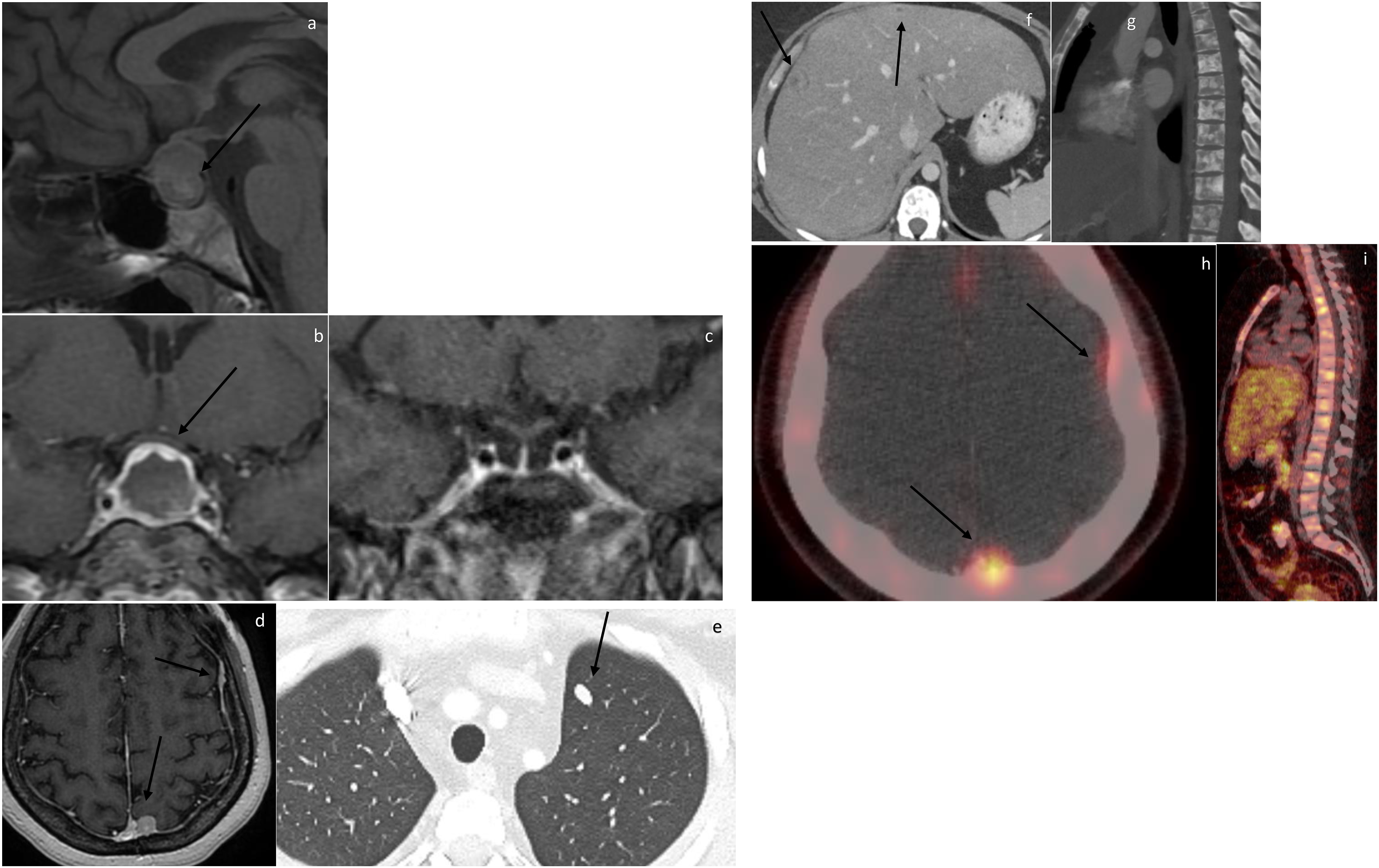
Imaging of metastatic disease
Six patients (42.9%) had metastatic disease confined only to the CNS. Eight patients (57.1%) had multiple system involvement, with the first site of disease being outside the CNS in all of them (Figures 1–3). 48.5-year-old male presenting with left neck adenopathy. He has a history of pituitary mass diagnosed 4.5-year ago status post-resection, with pathology interpreted at our institution as pituitary adenoma. Figure 3(a). Axial post-contrast CT neck demonstrates left neck adenopathy including stranding associated with a lymph node (arrows). Patient had biopsy with concern for neuroendocrine tumor and subsequently left neck dissection confirming metastatic PitNET. Figure 3(b). Axial post-contrast CT abdomen, venous phase, 2 years after the neck dissection demonstrates new liver masses (arrows) with one biopsied again and consistent with metastatic PitNET. Figure 3(c). Axial post-contrast T1-weighted MRI obtained few months after the CT abdomen demonstrates the development of parenchymal metastatic disease within the right cerebellar hemisphere (arrow).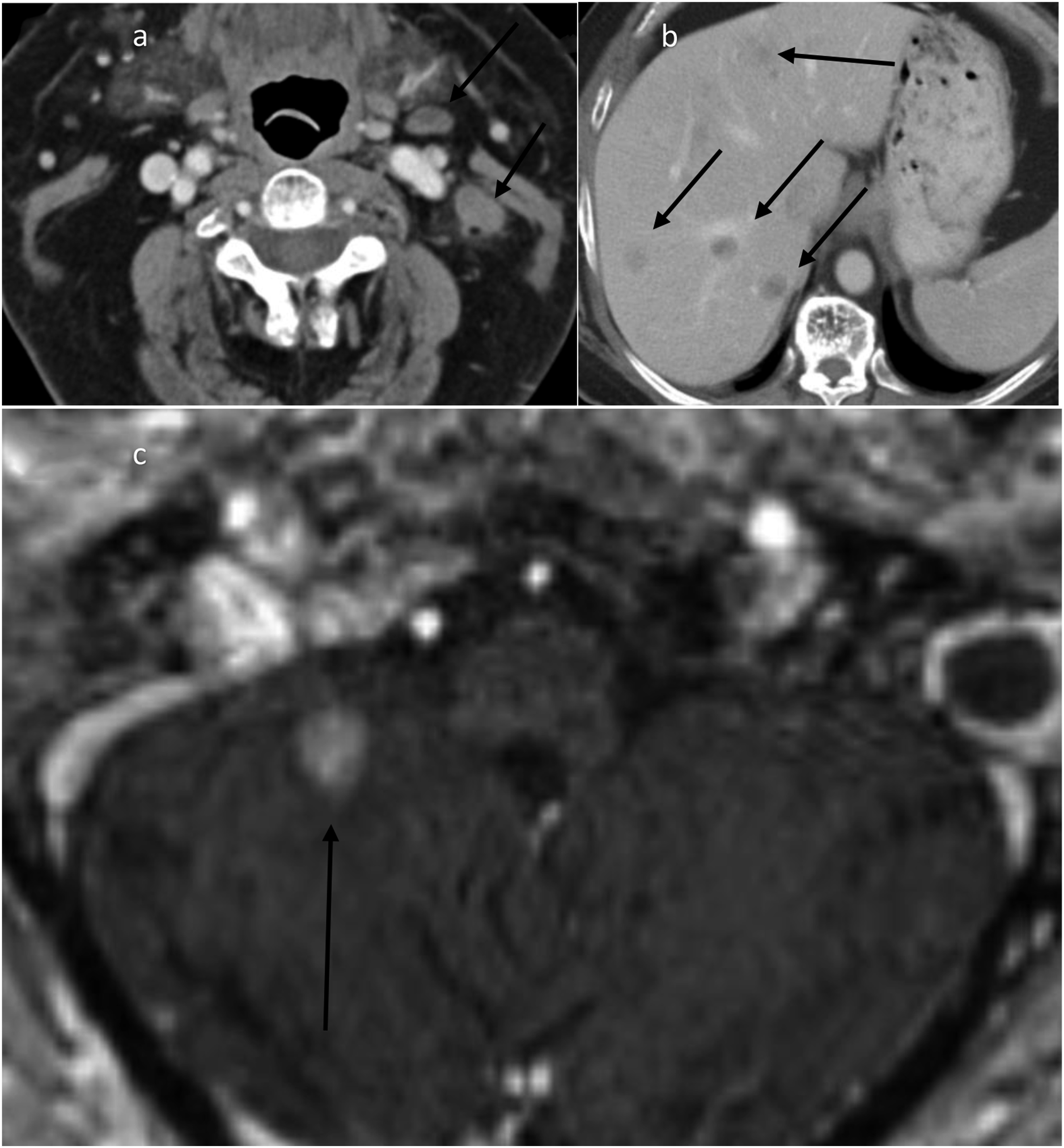
The most common site of metastatic disease was the CNS, and it was present in 11 out of 14 patients (78.6%). All 11 patients had intracranial involvement. Dural deposits were the most common brain CNS metastatic disease manifestation and were present in nine of the eleven patients (81.8%). Parenchymal metastatic disease was present in five patients (45.5%). LMD was uncommon and was present in one patient (9.1%) who also demonstrated spread to the ventricular system. All eleven patients had spinal imaging with three patients (27.3%) demonstrating spinal intradural extramedullary drop metastasis.
Eight patients (57.1%) demonstrated multiple metastatic disease sites, with five of them (62.5%) showing both CNS and extra CNS metastasis. Osseous metastatic disease was the most common extra CNS disease site and was present in six patients (75.0%). The bony spine was the most common site of osseous involvement, present in five patients (62.5%). Other extra CNS sites of metastasis included liver (4 patients, 50.0%), lungs (2 patients, 25.0%), lymph nodes (2 patients, 25.0%), and orbit (1 patient, 12.5%).
PET/CT imaging findings
In total, 11 patients (78.6%) had PET/CT imaging available for assessment of CNS and extra CNS metastatic disease. Five patients (45.5%) had 18F-FDG-PET/CT, five patients (45.5%) had 68Ga DOTATATE PET/CT, and one patient (9.0%) had both radiotracers. In all patients, CNS and extra CNS lesions demonstrated PET avidity with both radiotracers.
Survival analysis
Statistical and survival analysis.
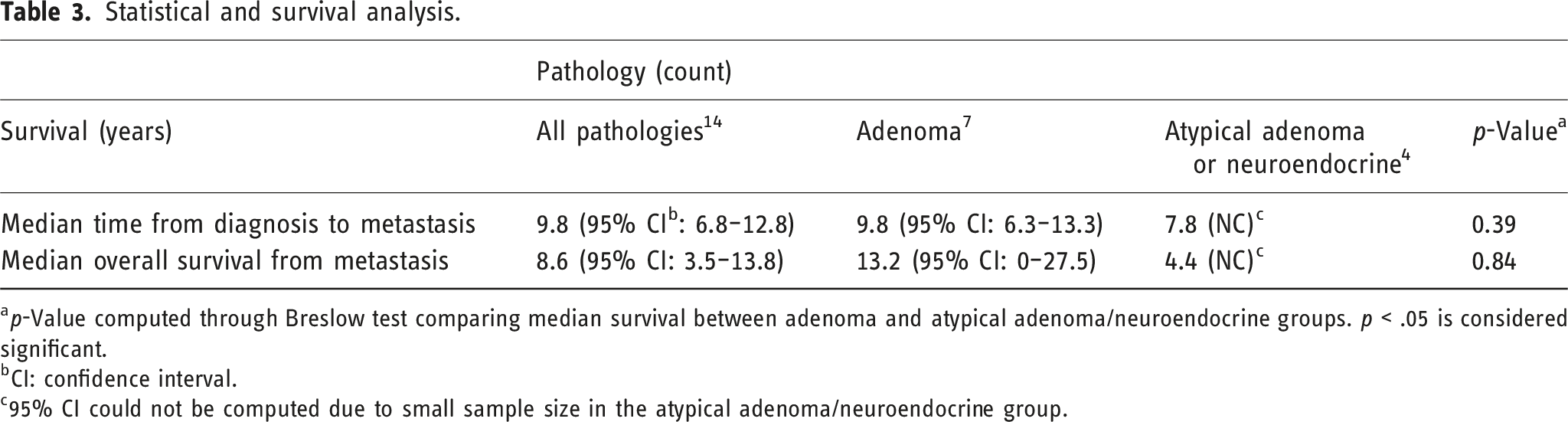
ap-Value computed through Breslow test comparing median survival between adenoma and atypical adenoma/neuroendocrine groups. p < .05 is considered significant.
bCI: confidence interval.
c95% CI could not be computed due to small sample size in the atypical adenoma/neuroendocrine group.
Discussion
Metastatic PitNET, previously known as pituitary carcinoma, is an exceedingly rare entity that is under reported, misreported, and frequently pathologically misclassified. 18 Recent studies have suggested that the incidence of metastatic pituitary tumors is increasing, in part due to increase in imaging detection. 19 However, dedicated imaging case series describing the imaging disease course are scarce and limited in sample size. In this case series of 14 patients, we report pertinent clinical and imaging findings relevant to the disease course.
In our case series, median age at initial diagnosis was 28.3 years, which is consistent with the reported literature indicating that most cases present between the third and fifth decades of life. 20 While the behavior and appearance of PitNET remain unclear with some demonstrating more aggressive course reflected in larger size and local invasiveness, metastatic PitNET has been reported to mostly resemble that of pituitary macroadenoma. 21 However, detailed imaging description of the initial and recurrent pituitary tumor remains underreported in the literature. In our case series, all five patients with initial imaging demonstrated macroadenoma Furthermore, all patients with initial imaging demonstrated symptomatic tumor effect on the optic chiasm and three patients demonstrated local invasiveness of the sphenoid sinus or clivus. At the time of pathological metastatic disease diagnosis, nine patients had residual/recurrent sellar disease with three additional patients demonstrating evidence of residual/recurrent disease involving the cavernous sinus for a total of 12 patients (85.7%) with evidence of local disease at the time of metastasis, reflecting the local aggressiveness of metastatic PitNET. These findings are consistent with McCormack et al.’s multi-institutional study that included 40 pituitary carcinomas, demonstrating that only 10% of the pituitary carcinomas achieved complete response to treatment. 22 In addition, our study demonstrated local invasiveness as a common feature of the recurrent/residual disease with 42.9% of patients demonstrating sphenoid sinus and/or local osseous invasion at the time of metastasis. Our case series also shows that the majority of metastatic PitNET are functional as 12 of 13 patients had biochemical evidence of pituitary hormone secretion with ACTH secreting tumors being the most common, representing 50% of the cases. This is consistent with the study by McCormack et al. that also demonstrated ACTH secreting tumors are the most common secreting subtype at a frequency of 47.5%. 22
CNS dissemination was the most common in our case series with a total of 11 patients (78.6%) demonstrating CNS dissemination. Dural metastasis was the most common CNS manifestation. Dural metastases were present in nine patients and in some cases prospectively interpreted as meningioma. Three patients with dural metastasis demonstrated concurrent spinal drop metastasis. Parenchymal involvement was present in five patients. Lastly, LMD/intraventricular disease was not common and was present in only one patient. Our case series suggests that total neuroaxis imaging should be considered for any patient with concern for metastatic PitNET.
Extra CNS metastasis was present in eight patients (57.1%) and a combination of both CNS and extra CNS metastasis was present in five patients (35.7%). Interestingly, all patients with combined metastasis had extra CNS metastasis prior to CNS metastasis. Osseous metastasis was the most common, with spine bone marrow being the most common site, followed by the liver. Our results are consistent with Burman et al., which demonstrated that osseous and liver metastasis are the most common sites of metastasis and are associated with ACTH secreting tumors, consistent with the prevalence of ACTH secreting tumors in our series. 23
Our case series did not uncover nodal metastasis despite full body PET imaging in 11 of 14. Nodal metastases were a prominent feature of an earlier series. 24
Our case series also suggests that PET/CT is effective for both screening and detection of metastatic disease with both 18F-FDG and 68Ga-DOTATATE radiotracers equally effective in detecting metastatic disease and local disease. All 11 patients that had PET/CT imaging in our case series had PET avid disease. Our results are consistent with the few small case series demonstrating the potential utility of PET/CT in assessment of metastatic PitNET with the added value of a larger case series than previously published studies.25,26
Lastly, we found no clear relationship between the initial pathologic diagnosis of the pituitary tumor and the presence of metastasis. This finding is in line with the prior literature. Historically, pituitary tumors were classified as adenomas, atypical adenomas (based on Ki67 index), and pituitary carcinoma.26,27 In total, we had seven patients initially diagnosed as pituitary adenoma and four diagnosed as atypical pituitary tumor/neuroendocrine tumor. There was no significant difference between these two pathologies in the time to metastasis detection from initial diagnosis (p-value = .39). Furthermore, there was no impact of pathology on overall survival (p-value = .84). This inability to predict metastasis is reflected in the recent update in classification of this entity as metastatic PitNET in the 5th edition of WHO classification.26–28 This point underscores how imaging is helpful to clinical assessment of PitNET. In the first place, imaging is most helpful in prospective identification of invasiveness and rapid tumor growth of a PitNET/pituitary adenoma. Later, in the context of aggressive adenoma and continued elevation of pituitary hormones, identification of meningioma like findings may prompt imaging of full neuroaxis and consideration of dural metastasis.
Our case series has a few limitations including the retrospective nature of this case series and the small number of patients. The retrospective nature of the study can result in selection bias. This was offset by consecutive inclusion of all patients with suggested diagnosis of metastatic PitNET into the study and subsequently only excluding patients without imaging studies, confirmed pathology at our institution, or clinical diagnosis and management of the lesions as metastatic PitNET. This approach ensured minimizing the effect of the retrospective limitation of the study. Another limitation is the potential effect of missing data on the study. Given that this is an imaging study with emphasis on imaging findings, any patient with missing or incomplete imaging data was not included in the analysis. Also, patients with missing clinical data that could impact the diagnosis of metastatic PitNET were excluded from further analysis and inclusion. The application of both of these conditions and emphasis on imaging features of metastatic PitNET limited the potential effect of missing data on our analysis. Any additional missing data that did not impact the purpose and scoop of this paper were reported as such and highlighted in the result section. Another limitation was the assessment of survival analysis. Given the small sample of the case series, a Barlow test was utilized given its more robust ability for assessment of survival difference in small subgroups. However, these results should still be interpreted with caution given that the observed survival differences could be due to confounders (such as age). On the other hand, our study has several strengths such as its robust inclusion criteria requiring pathological diagnosis, imaging of both CNS and body, and clinical diagnosis of metastatic pituitary tumor. Lastly, relative to prior reports, this is the largest dedicated study assessing multimodality imaging of metastatic pituitary tumors including assessment of local disease, CNS metastatic disease, and extra CNS metastatic disease with clinical correlation.
Conclusion
Metastatic PitNET is a rare neuroendocrine neoplasm. Dedicated imaging characterization of the entity is currently lacking in the radiology literature, and the scarce data available is primarily drawn from single case reports. In the present case series, we detail temporal imaging findings of the disease at the primary site and patterns of distant metastasis while discussing pertinent clinical associations. The presence of a locally aggressive functional pituitary lesion refractive to multiple treatment modalities should prompt imaging of the neuroaxis and body for a potential diagnosis of metastatic PitNET with close attention to the dura, bones, and liver. Extra CNS disease can be the first site of pituitary carcinoma that renders the diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.