
Abstract
Purpose
Recently, a novel device, the Woven Endo Bridge (WEB), was developed for wide-neck bifurcation intracranial aneurysms (WNBAs). The aim of this study is to investigate factors that contribute to adequate occlusion (AO) after the operation using detailed radiological images.
Methods
The subjects were 29 patients with 29 aneurysms who received WEB implantation for WNBAs between December 2020 and April 2022. We assessed the contributing factors to AO by retrospectively comparing the AO group and non-AO group.
Results
The mean age was 64.6 ± 13.1 years, and 18 were female (62.1%). The mean aneurysm dome width, aneurysm height, and aneurysm neck diameter were 4.8 ± 0.6 mm, 5.1 ± 0.6 mm, and 3.7 ± 0.6 mm, respectively. After about 6 months, 22 of 29 patients (75.9%) had AO. Complications were observed in 2 patients (6.9%), renal artery injury in one, and minor cerebral infarction in another, but the modified Rankin scale scores of both patients remained unchanged. Multivariate analysis extracted only WEB shape modification (WSM) as a contributing factor to AO (odds ratio: 0.912, p = 0.0287).
Conclusion
WEB implantation for WNBAs was a treatment modality with acceptable efficacy and safety. WSM was the only significant factor contributing to non-AO after the treatment. We should clarify the mechanisms or causes of WSM to achieve AO after WEB implantation in future.
Introduction
Endovascular treatment of wide-neck bifurcation intracranial aneurysms (WNBAs) is a challenging procedure due to the high recurrence rate. 1 Although stent-assisted coil embolization or flow diverter placement have been reported to reduce the recurrence rate, complete occlusion (CO) rates are 67.2% for stent-assisted coil embolization, 2 and 61.5%–73.2% for flow diverter placement,3,4 which are not satisfactory compared with clipping. 5 Recently, the Woven Endo Bridge (WEB; MicroVention, Tustin, CA, USA) was developed based on a novel treatment concept called the flow disruptor. The WEB is available in spherical (single layer sphere, SLS) or cylindrical (single layer, SL) type and is a device that modifies the flow within the aneurysm neck to promote intra-aneurysm thrombosis and endothelialization of the neck, resulting in CO. According to large studies including the WEB Intrasaccular Therapy and WEB Clinical Assessment of Intrasaccular Aneurysm Therapy, the adequate occlusion (AO) rate after WEB implantation for WNBAs is 80.0%–85.4%,6–9 which is favorable compared with previous outcomes using other devices. On the other hand, size selection is important to achieve AO after WEB implantation. 10 The WEB is a novel device, so various criteria have been proposed for its size selection, but the actual process of size selection can be confusing. There are also reports of a factor related to recurrence called WEB shape modification (WSM), which is a change in the shape of the device after WEB implantation.11–17 WSM is also described as WEB compression, and is often defined as vertical compression of the WEB device itself. The frequency is as high as 31.6%–75.0%, but studies as a factor involved in recurrence have not yet reached any conclusion. Our present study retrospectively investigated various factors including the contribution of WSM to AO after WEB implantation using detailed radiographical images in our institution.
Materials and methods
Patient assessment
A total of 32 aneurysms in 32 patients received WEB implantation at Juntendo University Hospital between December 2020 and April 2022. The inclusion criterion was intracranial aneurysm with a neck of 4 mm or more or a dome-to-neck ratio of less than 2, located at the bifurcation of the anterior or posterior circulation. The surgeon was one of the co-authors (HO) with adequate experience in endovascular treatment. Of the 32 patients, 29 aneurysms in 29 patients with follow-up angiography at approximately 6 months were finally considered eligible. Three patients were excluded, because two refused follow-up and one was not followed up after 6 months due to high exposure to radiation at the time of initial surgery. Age, sex, history, and smoking history were reviewed from the patients’ medical charts. Clinical evaluations were performed using the modified Rankin scale (mRS) preoperatively, immediately after surgery, and 6 months after surgery. The presence or absence of complications was determined based on the electronic medical record. This was a retrospective study conducted in a single center.
Antiplatelet therapy
All patients received dual antiplatelet therapy with aspirin 100 mg and clopidogrel 50–75 mg daily, depending on the patient’s body weight, at least 2 weeks before the procedure in the case of rescue stenting. Only aspirin 100 mg was continued for about 1 week after WEB implantation, and then aspirin was discontinued.
Device and procedure
The device selection between WEB SL and SLS was based on the dome-to-neck ratio. SL was selected for aneurysms with a dome-to-neck ratio of 1–1.5, and SLS for aneurysms with a dome-to-neck ratio of 1.5–2. The WEB size was selected according to the product protocol based on the mean aneurysm dome width and height. In almost all cases, an Axcelguide 6-French (Medikit, Tokyo, Japan), ultra-long guiding sheath was positioned through the transfemoral approach as distal as possible. A SOFIA Select 5-French (Terumo, Aliso Viejo, CA, USA) was coaxially advanced as close as the aneurysm neck, and then a VIA (Terumo, Aliso Viejo, CA, USA) for the WEB delivery was advanced. The WEB was delivered carefully while adjusting the position of the VIA. A Dyna-CT (Axiom Artis dTA, Siemens Healthcare, Forchheim, Germany) was used to confirm full opening of the device and apposition to the aneurysm wall.
Image analysis
Aneurysm locations and morphologies including dome width, height, and neck width were evaluated on the images produced with a biplane angiographic system (Siemens Artis Q BA Twin System, Siemens, Munich, Germany) with three-dimensional rotational angiography.
WSM refers to vertical compression of the device, which is relatively frequently observed during follow-up after WEB placement. The WSM rate was defined as the percentage determined by measuring the distance between the proximal and distal WEB makers in cross-sectional images by cone-beam CT after WEB implantation and at the last follow-up (Figure 1). Measuring method of WEB height on the cone-beam CT angiogram immediately after WEB implantation (a) and at 6 months follow-up (b). Two-headed arrows show WEB height distance. The WEB device was compressed within 6 months.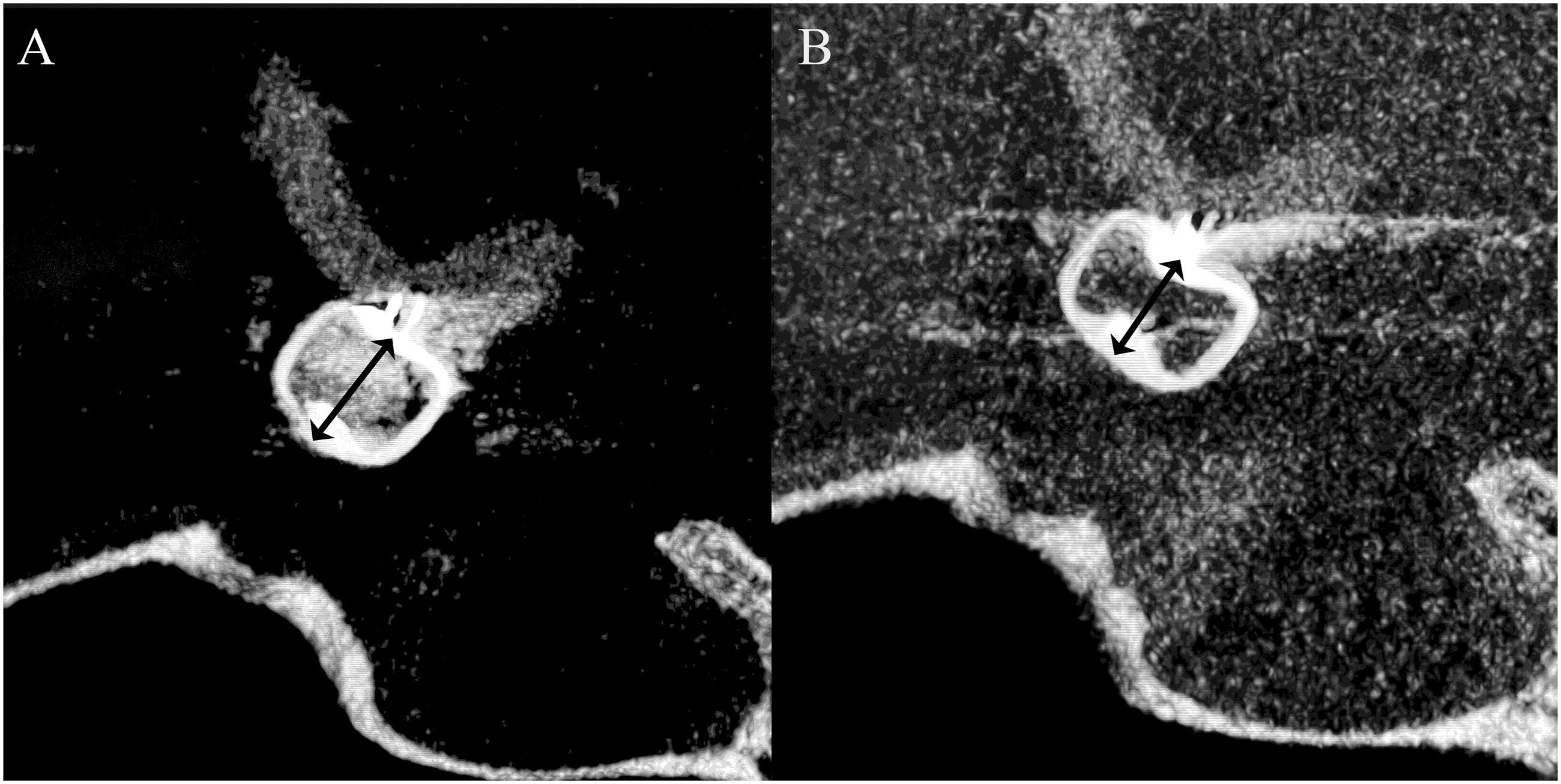
WSM rate (%) = (1- [distance at 6-month follow-up/distance immediately after WEB implantation]) x 100
Basic experiments have shown that the vertical resistance of the WEB is stronger if the WEB is horizontally compressed during placement. 18 Selecting a WEB that is larger than the actual aneurysm is also reported to improve the embolic status. Therefore, we defined the WEB oversizing ratio as a quantitative parameter. 19
Oversizing ratio = WEB width/aneurysm width
Based on the findings of the 6-month follow-up angiography, the embolization status was evaluated using the Raymond 3-point scale, which consists of CO, residual neck (RN), and residual aneurysm (RA). CO and RN were defined as AO, and RA was defined as non-AO based on the fact that the inflow of contrast medium inevitably remains in the recess on the bottom of the WEB device as found in other large studies.7–9,20 Anatomical evaluations were independently performed by authors of the present study (HO and TF). Discrepancies were resolved by another neurosurgeon.
Statistical analysis
Binary variables are presented as value and percentage. Continuous variables are presented as mean ± standard deviation and range. Differences between the two groups for the binary variables were assessed using the Fisher exact test. Differences between the two groups for continuous variables were assessed with the Mann–Whitney U test. Multivariate logistics analysis was performed to identify potential predictive factors of AO, using all candidate variables with p values of less than 0.15 in univariate analyses. p values less than 0.05 were considered statistically significant. The data were obtained using statistical software, GraphPad Prism 7 (San Diego, CA, USA) or EZR version 2.13.0 (Saitama Medical Center, Jichi Medical University, Omiya, Saitama, Japan).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study, patient consent is not required.
Results
Patient, aneurysm, and device characteristics
Demographic data of 29 patients.
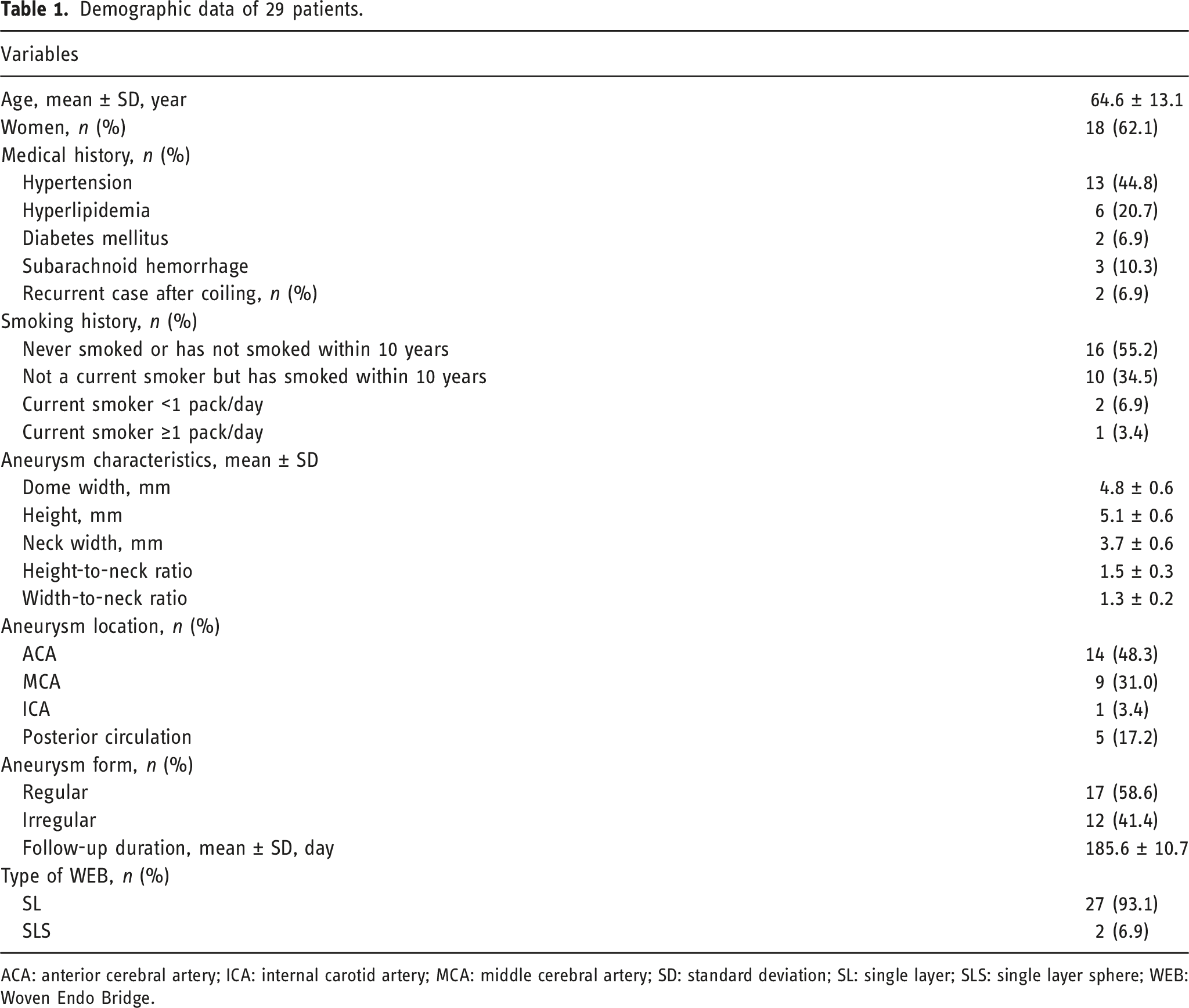
ACA: anterior cerebral artery; ICA: internal carotid artery; MCA: middle cerebral artery; SD: standard deviation; SL: single layer; SLS: single layer sphere; WEB: Woven Endo Bridge.
The types of WEB were 27 SL (93.1%) and 2 SLS (6.9%). The mean follow-up angiography period was 185.6 ± 10.7 days.
Anatomical and clinical outcomes
Summary of outcome after WEB implantation.
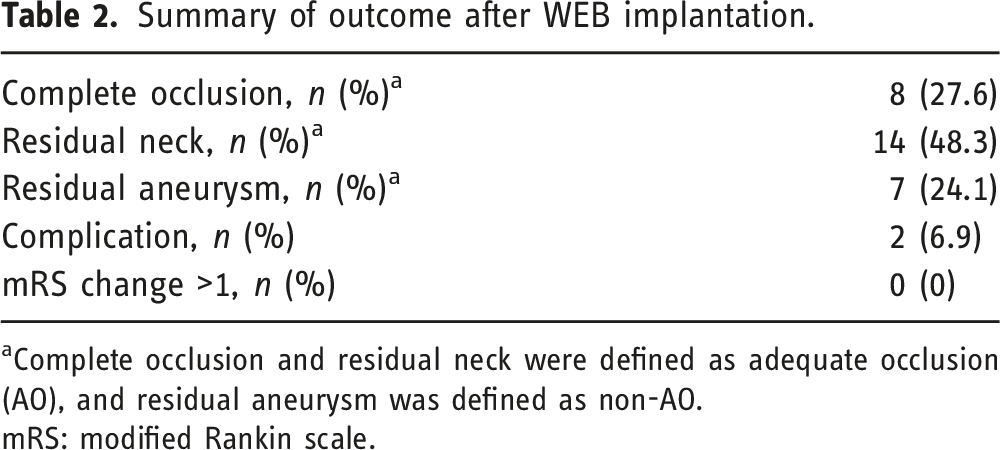
aComplete occlusion and residual neck were defined as adequate occlusion (AO), and residual aneurysm was defined as non-AO.
mRS: modified Rankin scale.
Complications were observed in 2 patients (6.9%), renal artery injury in one patient caused by a guide wire perforation during the procedure and minor cerebral infarction in another. The mRS score at discharge was unchanged from pretreatment in both patients. No patients had worsening of mRS score.
Contribution factors to adequate occlusion
Contributing factors to AO after WEB implantation by univariate and multivariate analysis.
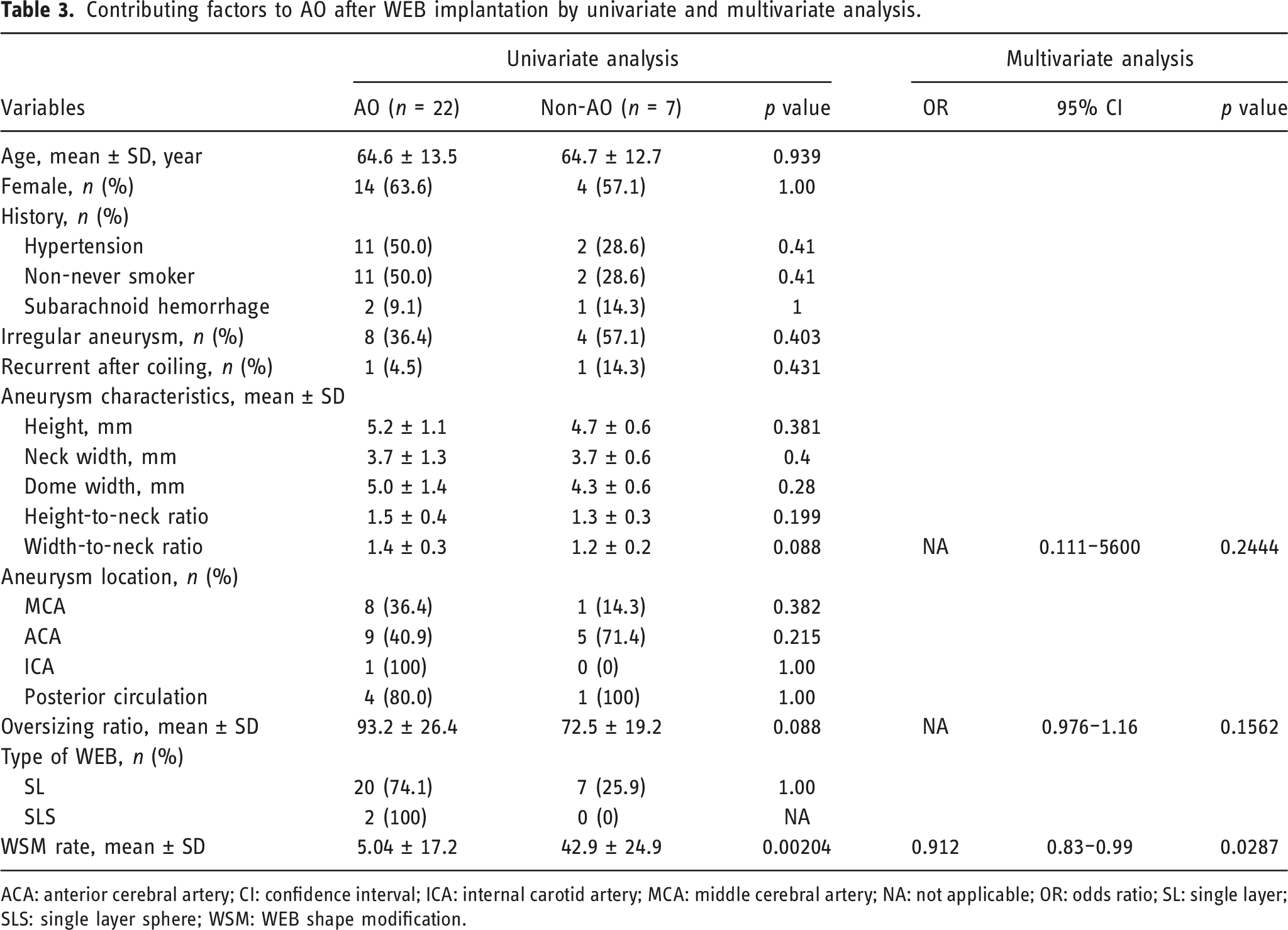
ACA: anterior cerebral artery; CI: confidence interval; ICA: internal carotid artery; MCA: middle cerebral artery; NA: not applicable; OR: odds ratio; SL: single layer; SLS: single layer sphere; WSM: WEB shape modification.
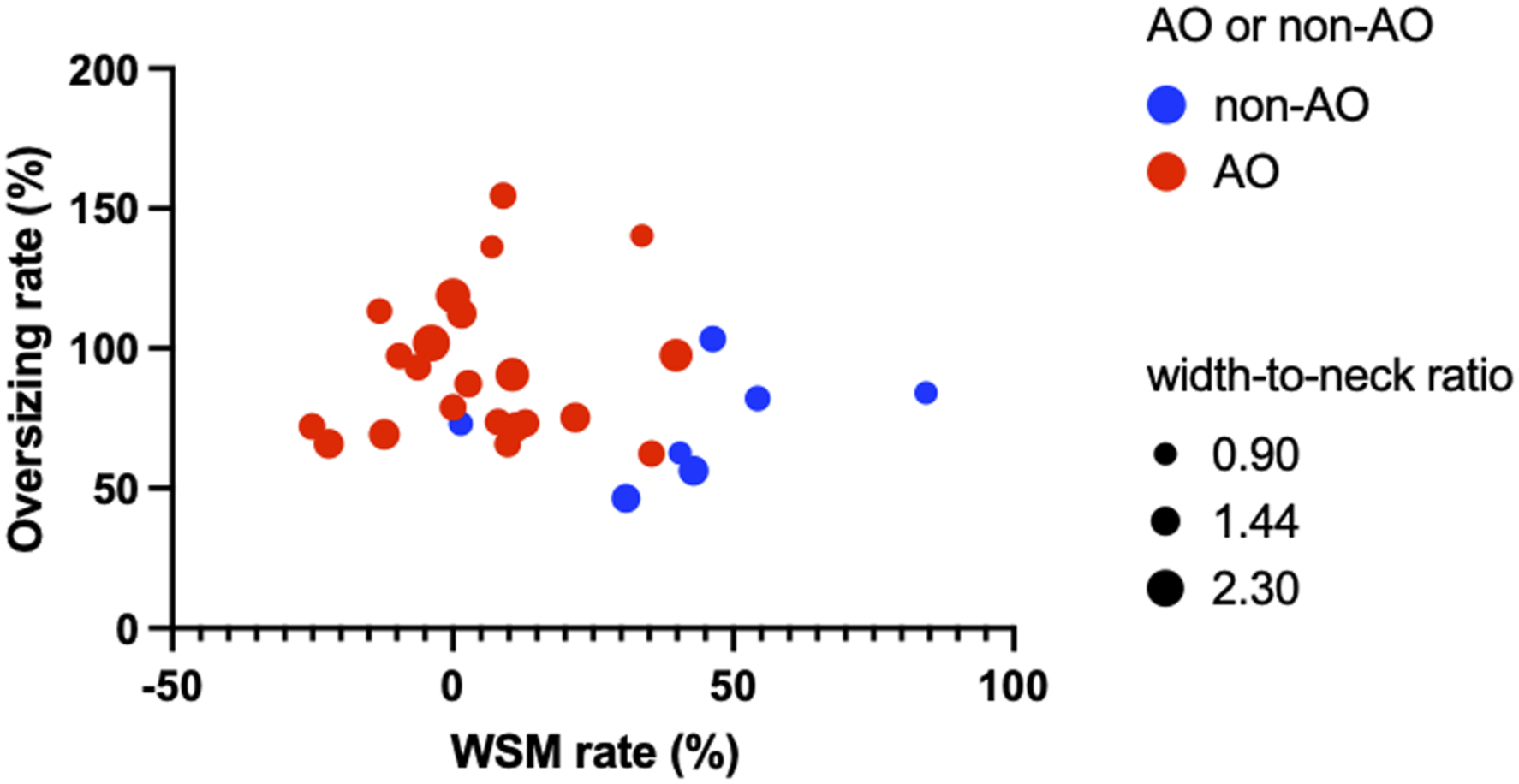
Bubble plots are color-coded into AO (red) and non-AO (blue) for each case, and the width-to-neck ratio is indicated by plot size. The positions of the plots are indicated by the WSM rate and oversizing ratio on the X and Y axes, respectively.
Discussion
Woven Endo Bridge implantation has acceptable adequate occlusion rate and low complication rate for treating wide-neck bifurcation intracranial aneurysms
The results of the present study showed that the rate of AO was 75.9% and the complication rate was 6.9% at 6 months after WEB implantation for WNBAs in Japan. Considering the acceptable AO rate and low complication rate in addition to the fact that no patients had worsening mRS, WEB implantation for WNBAs is a relatively effective and safe treatment. However, since the WEB is not a device that improves the occlusion rate with long-term follow-up20,21 as with flow diverter devices, inquiry into the causes leading to non-AO after WEB implantation is important.
Woven Endo Bridge shape modification is a significant factor contributing to non-adequate occlusion after Woven Endo Bridge implantation
In the present study, WSM was the only significant factor contributing to non-AO. The WSM does not act simply through device compression due to the hammer effect of blood flow, but rather involves connective tissue and collagen retraction during the healing process of aneurysms after WEB implantation according to a recent animal study. 16 Many previous reports indicate that WSM does not contribute to AO.12,14,15,17 The present study found the impact of WSM on AO was determined by measuring detailed device shortening. The average WEB shortening of 86% over the course of 6 months in this study suggests that this is a frequent phenomenon for the WEB as a whole. Although the metal coverage ratio of the bottom surface of the WEB is usually high, the observation that changes in the mesh structure due to WSM can cause a decrease in the coverage ratio is important. Although our study did not find that oversizing ratio contributed to AO, bubble plot showed the population of non-AO manifested low oversizing ratio and high WSM rate (Figure 2). Perhaps the most important consideration in selecting the WEB size for WNBAs is a size that is slightly larger than the aneurysm as far as possible and to maintain a high metal coverage rate on the bottom surface of the WEB, which will lead to the prevention of WSM, resulting in high AO rate.
Limitations
There are several limitations to this study. First, the population is small, but more cases are expected to be accumulated, since the WEB device itself has been covered by insurance since 2020 in Japan. Second, the follow-up period is short. Although the results of the phenomenon in the short term after WEB implantation investigated in this study were clear, further studies are needed to determine whether the WSM is stable or progresses in the long term, and how the occlusion rate depends on these changes. The third point is that the population is small. As mentioned above, WEB has been covered by insurance in Japan for only 3 years. In addition, this single-center study included a small population size, making generalization of the results of this study difficult. We hope that this study will encourage a future multicenter study. Finally, the selection bias for the WNBAs, the device is not available for all cases of WNBAs, since the procedure is difficult to complete unless the aneurysm trajectory is coaxial from the proximal vessel. This bias in particular makes comparisons with other techniques such as coil embolization and craniotomy clipping difficult. Further case series and device development will be needed to evaluate the true value of the WEB device in comparison with conventional treatment methods.
Conclusions
WEB implantation for WNBA is a treatment modality with acceptable efficacy and safety. WSM was the only significant factor contributing to non-AO outcomes after the treatment. We need to further clarify mechanisms or causes of WSM to achieve AO after WEB implantation in the future.
Footnotes
Acknowledgments
We thank all the operating room staff for their technical assistance and the electronic medical records clerks, who helped to collect patient data.
Declaration of conflicting of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: H.O. received a donation in the form of a research fund to the endowed chair of his departments and from Terumo Co., Ltd. The other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.