
Abstract
Background and Purpose
The results of the preclinical study of a novel polymer coil in treatment of elastase induced aneurysms will be presented in this paper.
Material and Methods
We induced 16 aneurysms in 16 New Zealand white rabbits at the origin of the right common carotid artery at the brachiocephalic trunk. Newly developed polymer coils in both groups for six aneurysms each and platinum coils for two aneurysms each were used. Control angiographies followed in both groups immediately after coiling as well as in the first eight animals 30 days after intervention (30 days group) and in the other eight animals 90 days after (90 days group). An explanation and histological evaluation of the treated aneurysms followed.
Results
The 12 animals in which the aneurysms were treated with polymer coils showed a complete occlusion (grade IV) in only 6 out of 12 aneurysms (50%), an almost complete occlusion (grade III) in 5 out of 12 (42%) and an incomplete occlusion in the treatment of one aneurysm (8%). Histologically, we observed a significantly more pronounced inflammatory response and neoangiogenesis in aneurysms treated with polymer coils only in the 30 days group.
Conclusion
Most difficulties and concerns with the polymer coils were related to the flexibility and detachment behaviour. Therefore, and due to the technical challenges of delivery, the novel polymer coil cannot be considered an alternative to the current platinum coils.
Keywords
Introduction
In recent decades, endovascular coiling has proven to be a successful alternative to neurosurgical clipping in the treatment of intracranial aneurysms.
In the ISAT (International subarachnoid trail) published in 2002, patients were observed for survival and freedom from severe physical limitations as a result of the intervention over a one-year period and endovascular coiling showed significantly better results than neurosurgical clipping. 9 In the last long-term follow-up of the ISAT from 2015, the results were further corroborated with regard to lower mortality and lower probability of severe physical disability after endovascular coiling compared to surgical clipping. 10 The BRAT (Barrow-Ruptured-Aneurysm-Trail), published in 2012, also compared coiling and clipping in the treatment of ruptured intracranial aneurysms and initially confirmed the benefits of the endovascular treatment option with a lower risk of secondary bleeding after coiling of aneurysms. 8 A study's follow-up from 2015 showed that in patients after coil embolization, at least in the treatment of aneurysms of the posterior cerebral circulatory system, coiling is still superior to clipping. 11
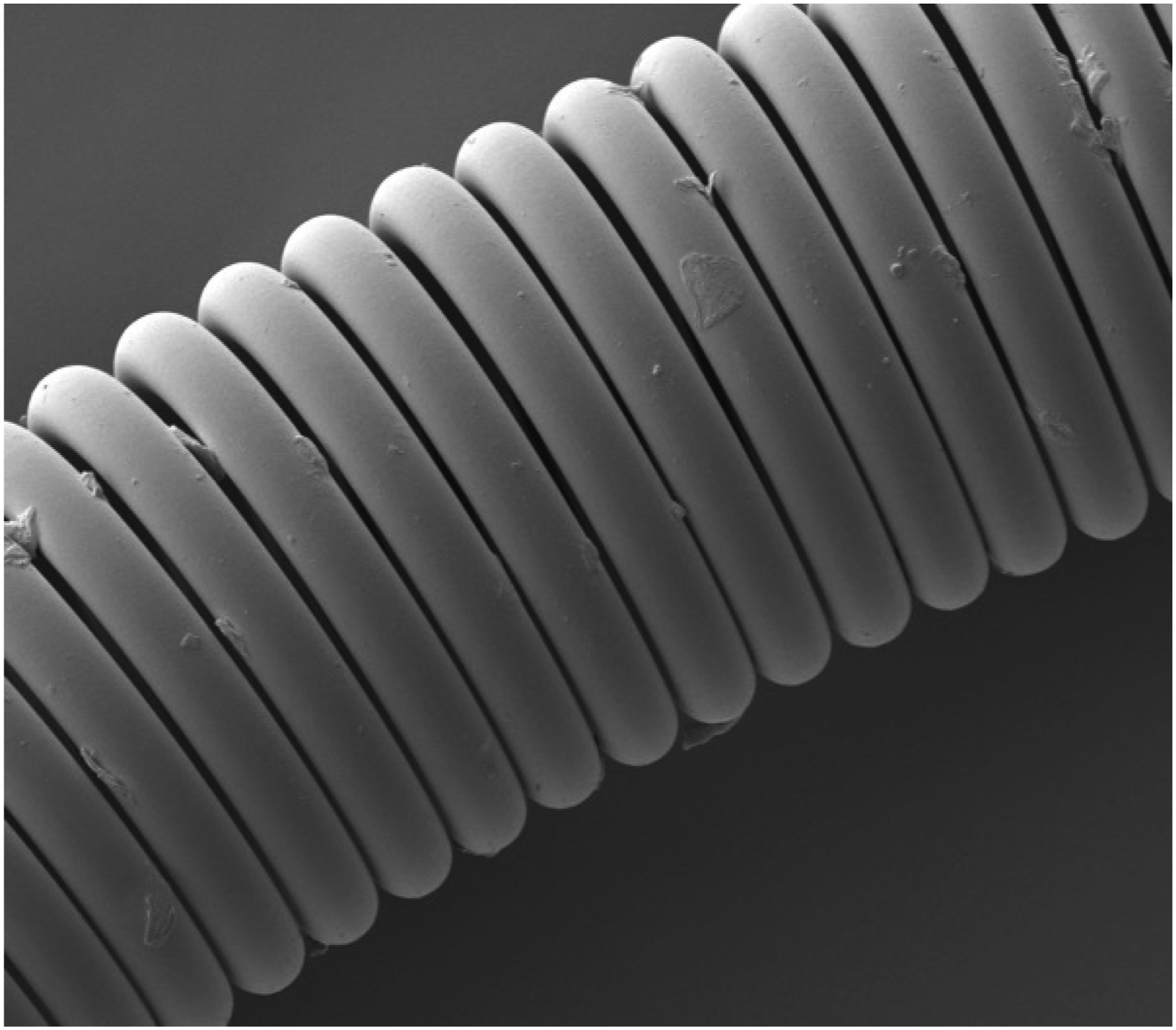
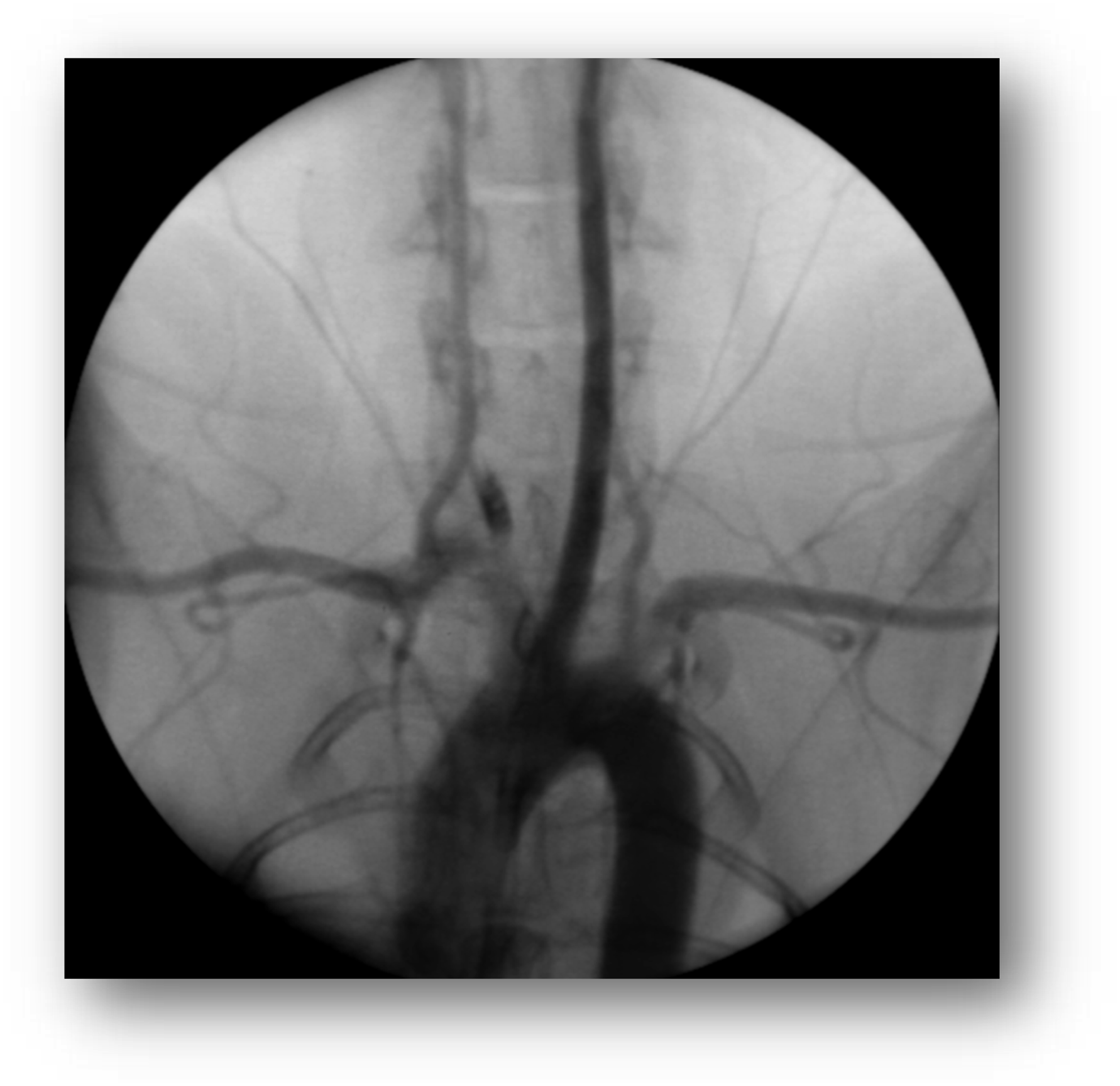
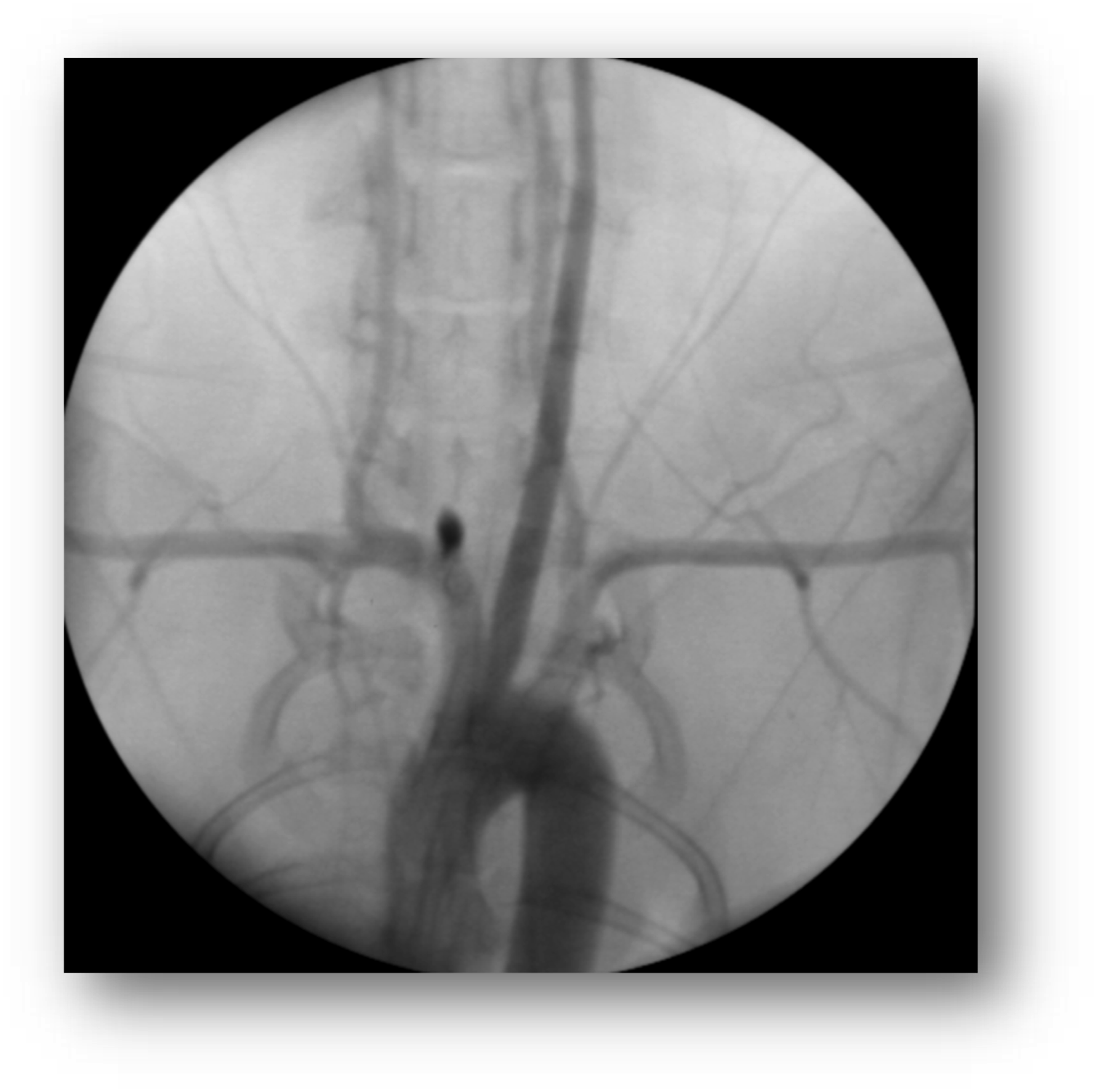
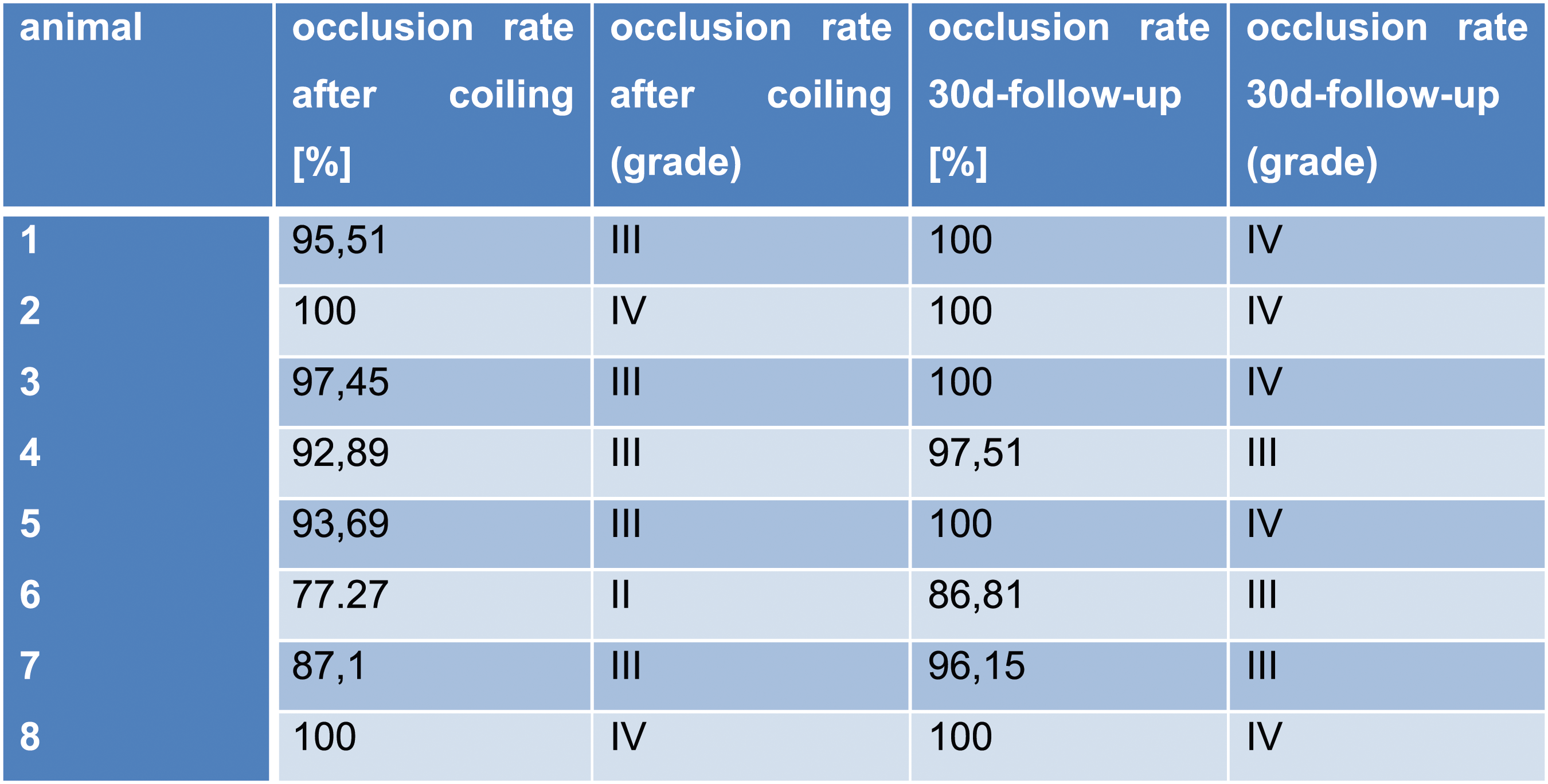
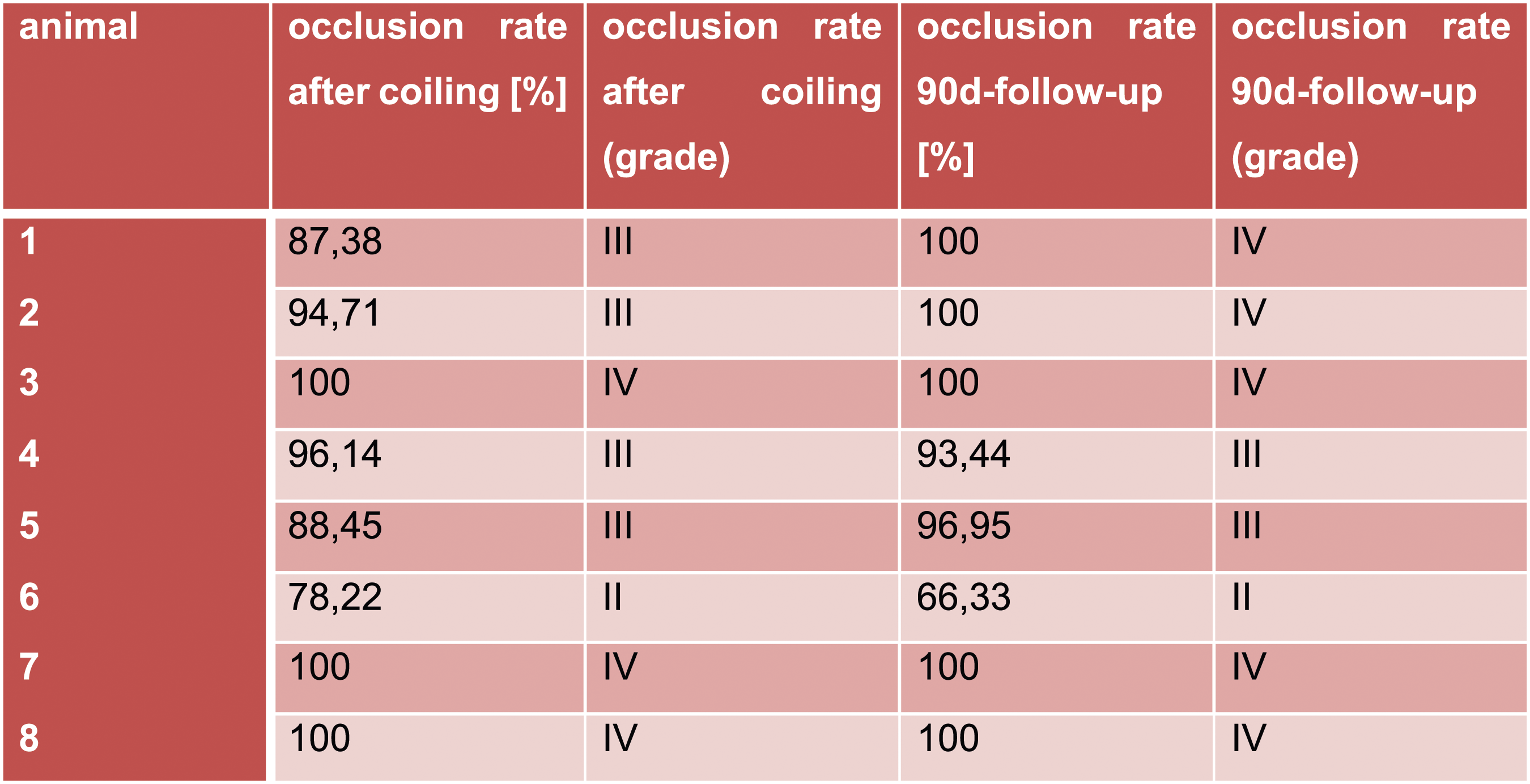
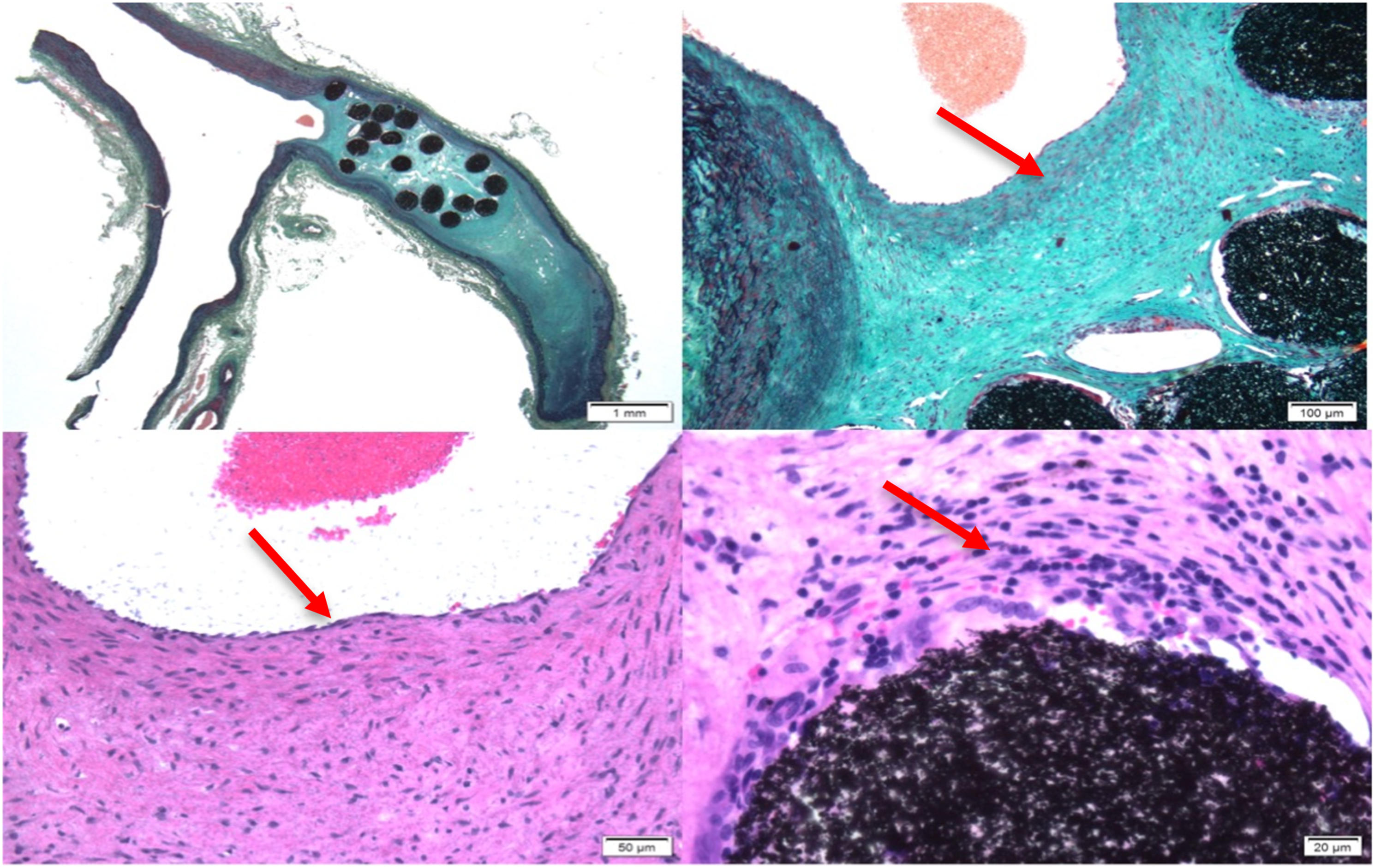
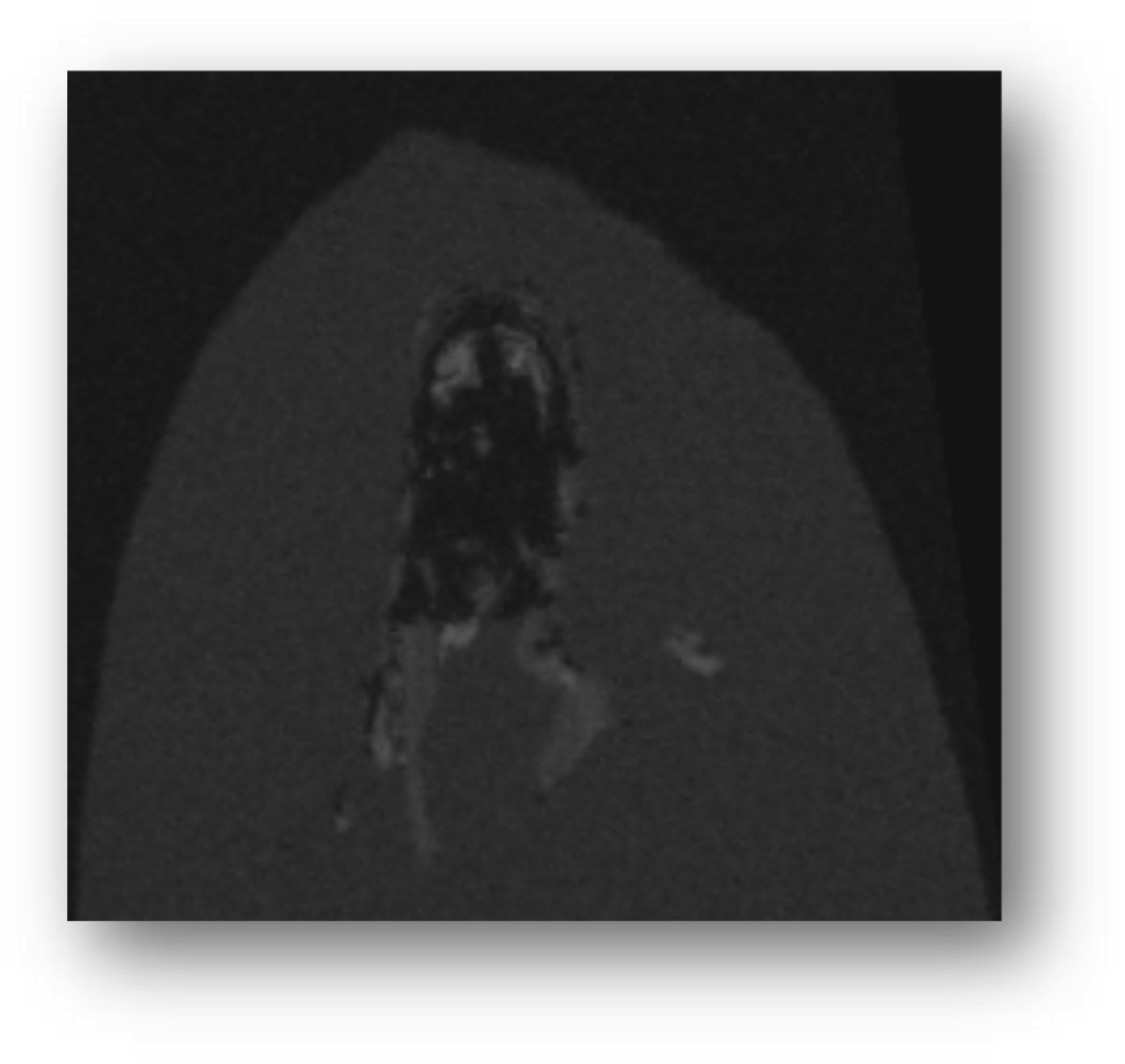
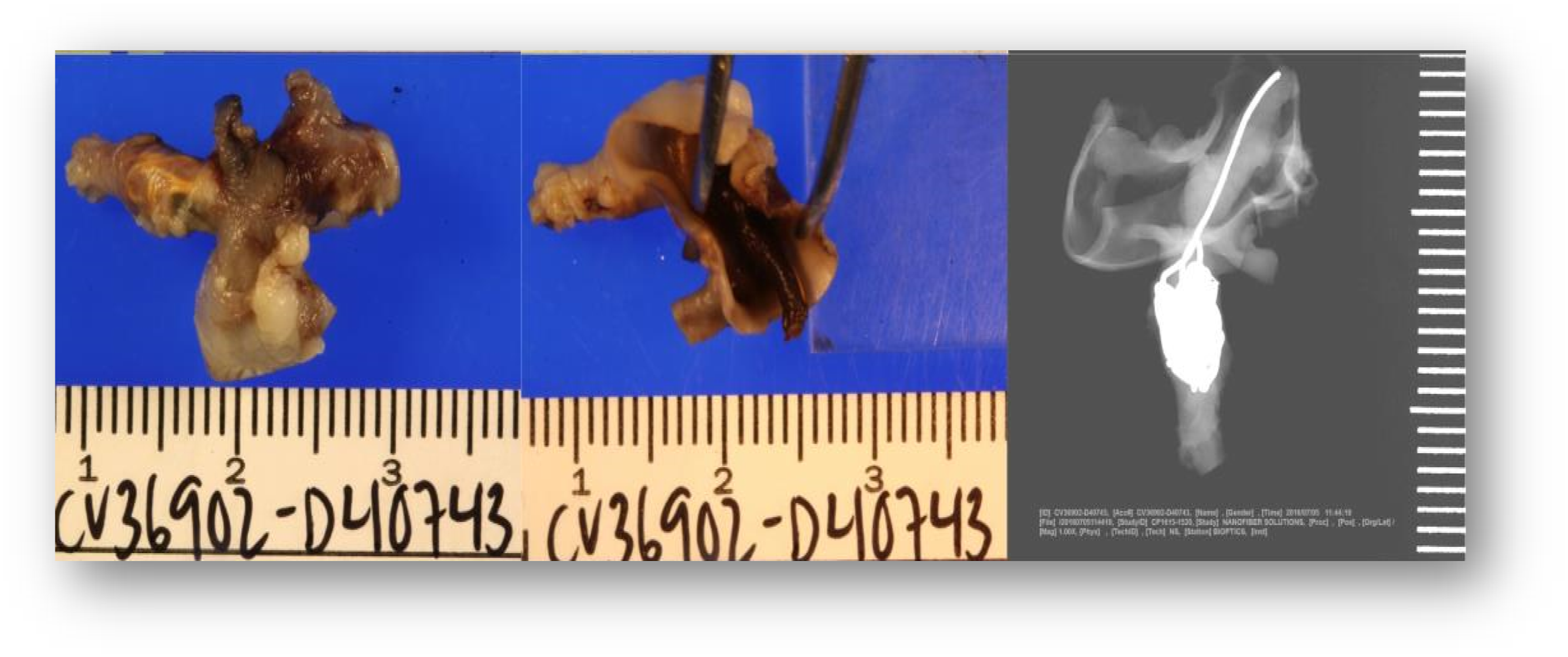
The results of the preclinical study of a novel polymer coil for the treatment of intracranial aneurysms which took place from March to November 2016 will be presented in this paper. The occlusion rates were evaluated angiographically in two different study groups immediately after coiling as well as 30 days and 90 days after intervention. In terms of product performance we also measured visibility, flexibility, stability during placement, possibility of coil protrusions and coil dislocations, as well as the detachment behaviour of the coils. After explanation, histological factors such as intraaneurysmal inflammatory response, thrombus organization, neoangiogenesis and endothelialization at the aneurysm neck were evaluated Figures 1–11 Polymer coil made of a 3D proprietary polymer structure that mimics an extra-cellular matrix. Conventional platinum coil. Aneurysm located in the region of the brachiocephalic trunk 1 month after coiling by DSA in animal no. 4 of the 30 days group (polymer coils). Aneurysm located in the region of the brachiocephalic trunk 1 month after coiling by DSA in animal no. 1 of the 30 days group (platinum coils). Classification of angiographically measured occlusion rates. Occlusion rates in the 30 days group in % and according to the 5-grade classification (polymer coils in animals 3 to 8, platinum coils in animals 1 and 2). Occlusion rates in the 90 days group in % and according to the 5-grade classification (polymer coils in animals 1 to 6, platinum coils in animals 7 and 8). 90 days group histology results show complete neck coverage and well organized neointimal growth. MRI of aneurysm treated with polymer coils. MRI of aneurysm treated with platinum coils. Polymer coil protrusion into the carrier vessel in aneurysm of animal no. 6–30 days group.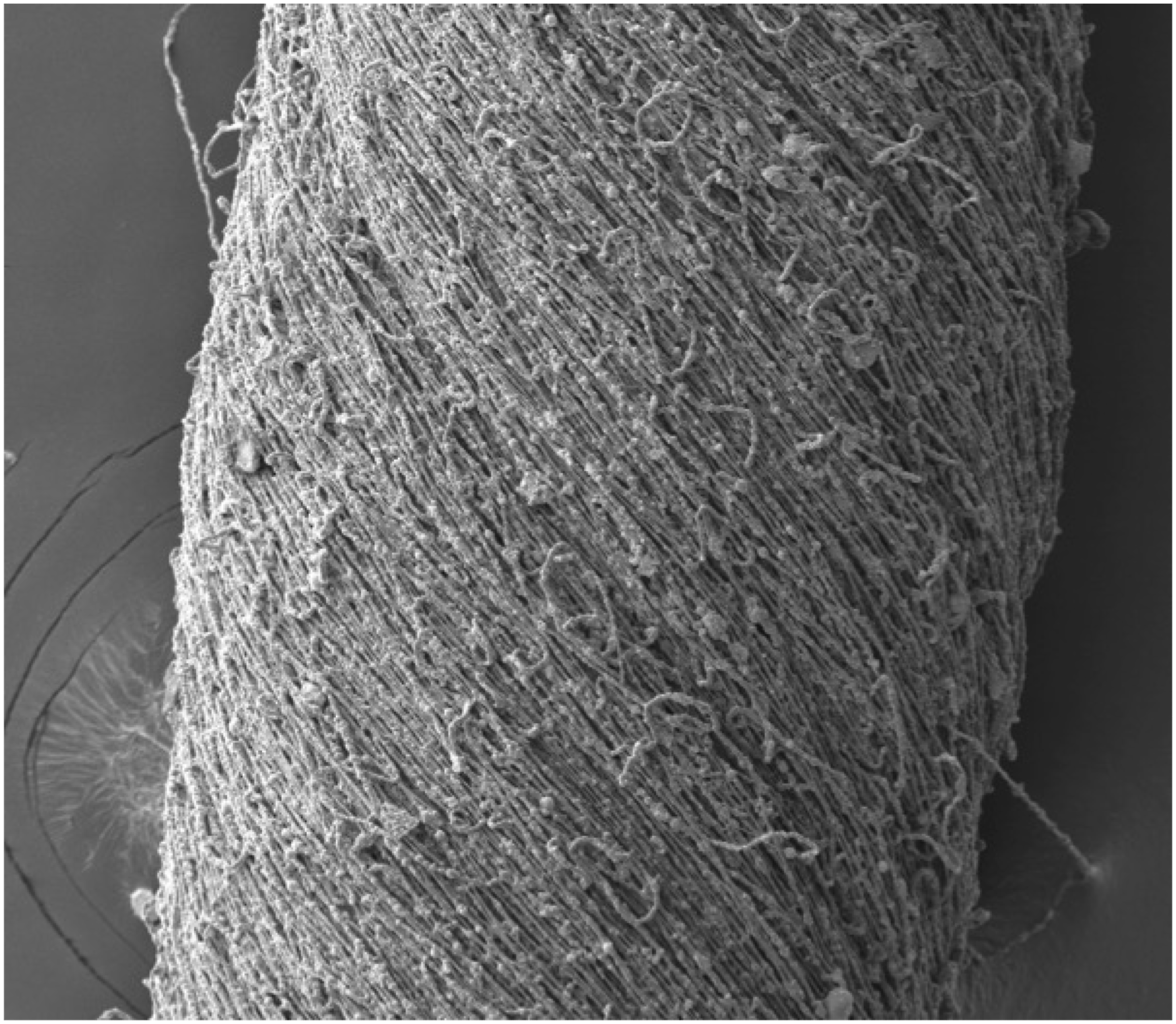

Materials and methods
Rabbit model
For the experimental performance, we used the bifurcation aneurysm model of Kallmes et al. on New Zealand white rabbits,2,3 which has been known since 1999 and nowadays is well established for the induction of aneurysms.
The experimental study in animals has been approved by the local ethics committee.
Anaesthesia protocol
After weighing, the animals were given 60 mg of ketamine and 6 mg of a two-percent xylazine solution per kg body weight intramuscularly for general anaesthesia required for the intervention. The anaesthesia began to take effect after an average of 10 min and would probably not have lasted much longer than 30 min if the anaesthesia had not been administered, but the rabbits were given an Optiva II intravenous cannula immediately after the full effect of anaesthesia, with a small diameter of 0.9 mm that was placed in an ear vein through which the same anaesthetic mixture of ketamine and xylazine in 10 mL 0.9% sodium chloride solution was administered to them by means of a perfuser at an average flow rate of 2.5 mL/h/kg.
Aneurysm induction
Following a longitudinal section of about 4 cm length on the right side of the neck centre, the right Common Carotid Artery (CCA) was exposed over a visible distance of about 3 cm after fascial cleavage. The vessel was then connected in the upper part with a non-resorbable thread. The middle and lower part of the vessel were also provided with a thread to facilitate subsequent treatment with the used sheath (Cordis Endovascular). The artery was punctured with small scissors suitable for fine preparations below the cranially located suture closure and then the 5F-lock could be inserted in caudal direction with the help of a guide wire.
This was followed by the application of approximately 3 mL of the iodine-containing contrast agent Ultravist 300 (Bayer AG) to provide angiographic imaging of the bifurcation of the brachiocephalic trunk and the resulting common carotid artery. A 3F-Fogarty balloon catheter (Edwards Lifesciences Corporation) was then introduced along the right common carotid artery to the bifurcation of the brachiocephalic trunk using the airlock. There, we fixed the balloon by adding a liquid mixture consisting of 0.9% sodium chloride solution and iodine-containing contrast agent in equal parts and controlled its position angiographically for correctness and sealing. If no permeability was visible in place of the balloon, in addition to the described mixture of sodium chloride and contrast medium, 100 U of elastase extracted from the pig pancreas (Worthington Biochemical) was administered. We then waited 20 min to allow the enzymatic effect of the elastase on the vessel wall in the applied area.
After the 20 min had elapsed, the previously applied fluid and the balloon catheter were removed from the sheath and finally the sheath itself with subsequent suture closure of the CCA below the puncture site. A subsequent displacement of the closure site further caudally along the elastase-damaged vessel wall resulted in the formation of a saccular aneurysm after several weeks. The size and filling of these aneurysms induced with porcine elastase can be influenced depending on the height of the suture closure. 4
Finally, the animal's skin was sutured with subcutaneous sutures. Aneurysm induction took about 60 min per animal. The rabbits regained consciousness about 20 min after the end of anaesthesia.
Intervention: Coiling
In a paper published in 2001, it was shown that aneurysms caused by the addition of pancreatic elastase show a progression in their growth only within approximately 3 weeks after aneurysm induction. 5 Therefore, after induction of the aneurysm, all of our rabbits underwent a resting period of 4 to 9 weeks in order to form the desired aneurysm and, in addition, to ensure sufficient recovery from the procedure performed during the induction. On the day of endovascular coiling intervention, the same anaesthesia protocol as for the induction procedure with ketamine and xylazine was performed first. The rabbits were then shaved in the area of the right groin, the area was disinfected with betaisodona solution and a sterile cover was applied. A skin incision of about 3 cm was made in the direction of the skin tension lines in the inner thigh area to expose the deep-lying femoral artery running through the adductor canal after fascial cleavage. After applying two sutures to the upper and lower part of the visible femoral artery and directly closing the lower part, we punctured the femoral artery with small scissors above the caudal vascular occlusion. This was followed by the introduction of a 5F sheath into the vessel (Cordis Endovascular). In order to view the aneurysms induced weeks ago and to get an impression of size and volume, we made angiographic images of the vessels in the area of the brachiocephalic trunk using DSA before the start of coiling.
The coiling of the depicted aneurysms with the described polymer coils followed, as well as in some animals with conventional platinum-containing coils – in both cases, the procedure was the same except for the different coils. We used an SL-10 microcatheter (Stryker Corporation), a Silverspeed 14 microwire (Medtronic) and a 4 x 10 mm Scepter Balloon (MicroVention Inc.). First, the aneurysm was probed via the groin and the microcatheter was placed. Then, the subclavian artery was probed and the balloon was inserted. After inflation of the balloon, the aneurysm was coiled and, after successful treatment, the balloon was deflated and removed together with its materials.
The sheath was removed from the vessel and the suture applied to the upper part of the visible femoral artery before the beginning of the procedure was tightened to close the vessel at this location. Finally, the skin of the animal was sutured with subcutaneous sutures, as in the case of aneurysm induction. Depending on the accessibility of the aneurysm, the number of coils required to achieve the desired density and the duration of the removal time of the coils per animal, the coiling process took 45 to 90 min. The rabbits regained consciousness about 20 min after the end of the anaesthesia.
Group classification
An equal division of 16 experimental animals into two groups of eight rabbits each in a 30 days short-term group and eight rabbits in a 90 days long-term group took place. Within the two groups, the aneurysms of six animals each were treated with novel polymer coils and of the remaining 2 with conventional platinum coils.
Performance of the final angiography and euthanasia followed by explanation
After 30 days in the first group and 90 days in the second group, DSA imaging was performed to angiographically assess the residual filling and occlusion rate of the aneurysms. The preparation of the rabbits for this last procedure was similar to that prior to aneurysm induction: After shaving in the neck area, this time the left carotid artery was exposed and a contrast medium containing approximately 3 mL of iodine (Ultravist 300) was applied via the vessel against the blood flow in the direction of the aorta, which thus also distributed into the brachiocephalic trunk, allowing imaging along the more or less occluded aneurysm depending on the result. The measurement and evaluation of aneurysm sizes in the obtained angiographies was performed with the software OsiriX. Directly afterwards, the euthanasia of the still anaesthetised animals was performed with a lethal injection of 8 mL of the barbiturate pentobarbital (Narcoren from Merial GmbH).
For the pending histological analyses, the part of the aortic arch including the brachiocephalic trunk with attached aneurysm was explanted and fixed in 3% phosphate-buffered formaldehyde solution.
In addition, after euthanasia, we performed MRI measurements on the aortic arches of individual animals to compare the occurrence of metal artifacts between aneurysms treated with polymer coils and those treated with platinum coils. FISP sequences (fast imaging with steady state precession) with an echo time (TE) of 2.8 ms, a repetition time (TR) of 10 ms, an inversion time (TI) of 800 ms and a slice thickness of 100 μm were recorded.
Histological analysis
After cutting the tissue fixed with formaldehyde, paraffin was used as embedding medium in which the samples were stored for 2 days. Afterwards, the tissue samples were transported to the United States and further processed by a US Pathology Institute. Tissue slices were made and analysed using Giemsa and haematoxylin-eosin staining.
The following histological parameters were examined in detail: -Intraaneurysmal inflammatory response -Intraaneurysmal thrombus organization -Angiogenesis -Endothelialization at the aneurysm -Integrity of the aneurysm wall
Statistics
For the creation of the statistics we used the SPSS statistics program from IBM. Mean values and standard deviations were determined for the parameters neck, length, width, area and residual filling directly after coiling, occlusion rate directly after coiling and final occlusion rate after 30 days or 90 days follow-up. We applied the chi-square test to determine frequency differences between the groups. The t test was used to compare the mean values of both groups. In addition, we defined a p-value of 0.05 as the alpha level.
Results
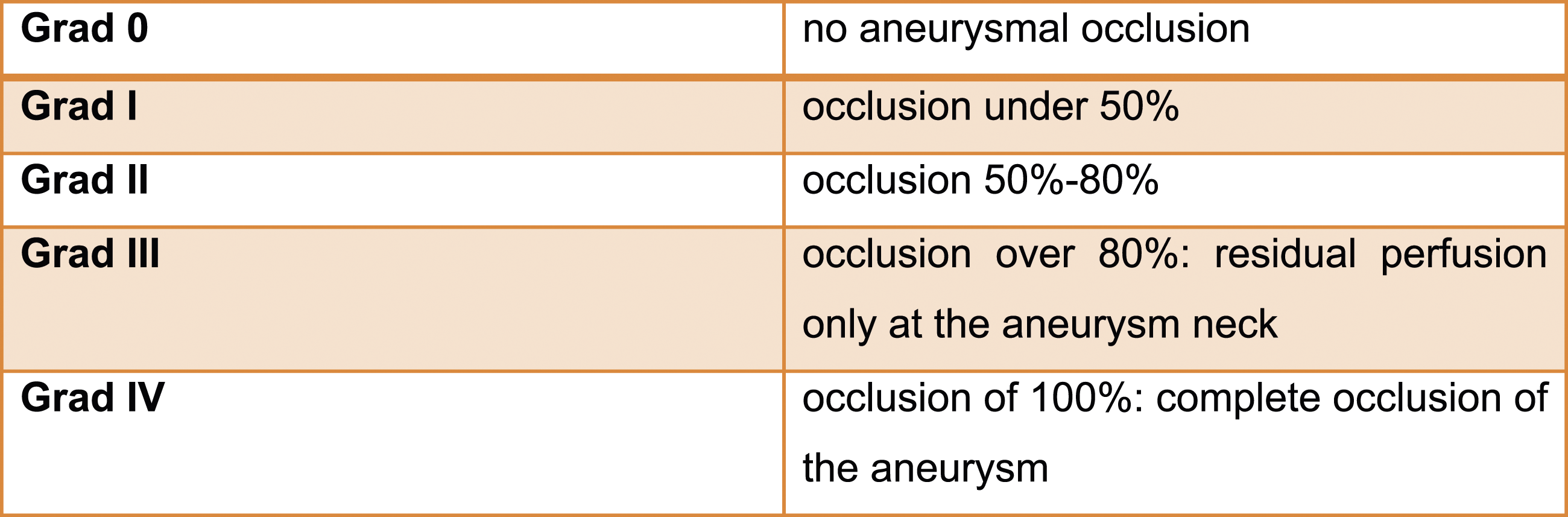
Aneurysm induction was performed in a total of 16 experimental animals with, depending on group membership, 30 or 90 days after endovascular intervention followed by angiography and histology. Within the two groups consisting of eight animals each, the aneurysms of six animals each were treated with the novel polymer coils and of the remaining 2 with conventional platinum coils. The sizes of the coils varied between 1 cm and 15 cm. A total of 63 coils were used in the two experimental groups, of which only 14 were platinum coils. The other 49 were the polymer coils to be tested. Neither the intervention for aneurysm induction nor the intervention for coiling therapy caused major complications in the rabbits – the animals enumerated survived the complete performance of the experiment without the need to change the intended protocol due to unplanned events. In all 16 induced aneurysms, very high occlusion rates could be measured immediately after coiling. In 14 aneurysms the occlusion rates increased or at least remained the same in the follow-up measurement and decreased in only two aneurysms in the follow-up. To illustrate the occlusion rate, we used a grade zero to four scale already established in the evaluation of flow diverters devices, which derives it from the residual filling of the aneurysm.
In the follow-up, we found a complete occlusion of the treated aneurysms in 10 out of 16 animals (63%, grade IV), an almost complete occlusion in 5 out of 16 animals (31%, grade III) and in one case (6%) an incomplete occlusion (grade II). In the four animals that received a treatment of the aneurysm with platinum coils, complete occlusion (grade IV) was achieved in all cases (100%) in the follow-up. The 12 animals in which the aneurysms were treated with polymer coils showed a complete occlusion (grade IV) in only 6 out of 12 aneurysms (50%), an almost complete occlusion (grade III) in 5 out of 12 (42%) and an incomplete occlusion in the treatment of one aneurysm (8%). In summary, in 11 out of 12 aneurysms treated with polymer coils we achieved complete (grade IV) or almost complete occlusion (grade III) of the aneurysm, resulting in 92% overall.
Compared to platinum coils, the polymer coils were less flexible, which resulted in limited stability when placing the coils. In 6 out of 12 (50%) aneurysms treated with polymer coils, the mechanical detachment of the coils within the aneurysm could not be optimally controlled and usually occurred too early. This resulted in a coil dislocation followed by a rescue manoeuvre in these 6 cases. In addition to that, coil protrusion was observed in 7 out of 12 aneurysms treated with polymer coils (58%), which is an extremely high rate that shows very high risk during aneurysm coiling. Thus, the coil protrusions and dislocations can be interpreted as a complication resulting from the combination of poor detachment behaviour, low flexibility and limited catheter stability of the polymer coils. In two cases of aneurysms treated with polymer coils, coil compaction was observed in the long-term group. The residual filling of the aneurysm in these two cases was greater in the 90 days follow-up than immediately after coiling. Histologically, we observed a significantly more pronounced inflammatory response and neoangiogenesis in aneurysms treated with polymer coils compared to the platinum coils only in the 30 days group. Furthermore in this group the thrombus organization was comparable and the endothelialization at the aneurysm neck was less pronounced than in aneurysms treated with platinum coils. In the 90 days group all histologically examined parameters, except for the intraaneurysmal inflammatory reaction, were more present than in the 30 days group and including the endothelialization of the aneurysm neck in aneurysms treated with polymer coils comparable to those where platinum coils were used. The integrity of the aneurysm wall remained completely intact in all cases.
Discussion
The still quite new endovascular therapy of intracranial aneurysms represents an established alternative to surgical clipping today and will become more and more important in the future thanks to advancements in medical technology and radiological imaging. These advancements also include further development of the materials used, such as the coils themselves. With the polymer coil tested here, an attempt was made to further expand the advantages of the coil.
In summary, 11 out of 12 aneurysms treated with polymer coils showed complete (grade IV) or almost complete (grade III) aneurysm occlusion, which is 91.7% and is a satisfactory result. In animals treated with platinum coils this was achieved in 100% of cases.
With regard to product performance, the visibility during the intervention of two polymer coils was found to be unacceptable. In addition, the material composition of the new polymer coil was expected to result in less artifacts in MRI imaging, which could not be confirmed in our individual measurements in direct comparison to the platinum coil. Otherwise, fewer metal artifacts in the polymer coil would have allowed a possible relief of DSA and the increased use of MRI in the aftercare of intracranial aneurysms treated with these coils. However, we found no difference in the occurrence of artifacts between the two coils in the MRI, which is why MRI-supported imaging as part of the aftercare with the polymer coil would not have a clear advantage over the platinum coil.
In terms of flexibility and stability, the polymer coil also lags behind the platinum coil: while in three out of four conventionally coiled aneurysms, the platinum coils showed good flexibility and stability and were considered acceptable in one aneurysm, these two parameters were rated in the acceptable rather than the good range for the polymer coils and in one case were rated unacceptable. In two cases of aneurysms treated with polymer coils, coil compaction was observed in the long-term group. The residual filling of the aneurysm in these two cases was greater at 90 days follow-up than immediately after coiling, which can be attributed to the non-optimal packing of the aneurysms by the polymer coils during the intervention. In addition, on average more polymer coils than platinum coils were used to fill one aneurysm. Despite these facts, there were no significant differences in the occlusion rates of the aneurysms of both groups according to statistical analysis. Only the neck length of the aneurysms was significantly larger in the 90 days group than in the 30 days group. However, when only the six animals treated with polymer coils in each group were compared, there were no significant differences - neither in the neck length nor in all other morphological parameters and measured occlusion rates. While unwanted coil protrusions were observed in 7 of 12 with polymer coils treated aneurysms (58.3%), which is an extremely high rate that shows very high risk during aneurysm coiling, this was only the case in one of four aneurysms in the with platinum coils treated animals (25%). The main concerns in terms of product performance were the flexibility and detachment behaviour of the polymer coils.
Compared to platinum coils, the polymer coils showed less flexibility, which resulted in limited stability when placing the coils. In 6 out of 12 (50%) aneurysms treated with polymer coils, the mechanical detachment of the coils in the aneurysm could not be optimally controlled and was usually performed too early (premature detachment). In these 6 cases, this resulted in coil dislocation followed by a retrieval manoeuver using the Alligator Retrieval Device, a specially designed micro forceps consisting of a 0.016" stainless steel insertion wire with microfabricated precision gripping arms. The failure rate with necessary retrieval was in both groups 30 days and 90 days the same with a total of 3 with polymer coils treated aneurysms. There were no problems with any of the platinum coils. Thus, coil protrusions and dislocations can be considered as complications resulting from the combination of poor detachment, low flexibility and limited catheter stability of the polymer coils, which ultimately clearly resulted from the material properties of the polymer. For example, when platinum coils are used in balloon-assisted coiling, coil protrusions can be expected in only 10% of cases on average. 7 Those numbers we have counted for polymer coils are therefore clearly too high in this respect. Coil compaction being observed in two cases of aneurysms treated with polymer coils in the long-term group is in turn not clearly attributable to the material composition of the polymer coil alone, since coil compaction is also a frequently occurring problem in aneurysms treated with platinum coils and can make renewed intervention necessary, although it is not entirely clear whether actual coil compaction or progressive aneurysm growth is mainly responsible for a larger residual filling observed in the follow-up.1,6 At this point it should also be mentioned that originally, with an additionally planned 180 days group, a total of three groups were planned for this experimental study, but due to the aforementioned problems regarding the flexibility and detachment behaviour of the polymer coils, the product developers decided to discontinue the study already after the 90 days group and to work on improving the product’s weak points first.
However, the polymer coil was convincing in the evaluation of histologically examined parameters. The intraaneurysmal inflammatory reaction measured by the deposition of immune cells was on average stronger in the 30 days group for aneurysms treated with polymer coils. In the platinum coils this was only minimal. In terms of thrombus organization at the neck of aneurysm, the polymer coils were able to keep up with the platinum coils. Only in two aneurysms treated with polymer coils in the 30 days animal group a comparatively weak thrombus organization of less than 50% of the neck surface was measured, which can be explained by the relatively short time after intervention. In the 90 days group, a thrombus organization of more than 75% in the neck area was found in all animals in the follow-up - both after treatment with polymer coils and after use of the platinum coils. The high degree of thrombus organization led to a complete occlusion of 100% in three aneurysms of the 30 days animal group and two aneurysms of the 90 days animal group, which angiographically showed a small residual filling directly after coiling. In the animals treated with polymer coils, neoangiogenesis in the aneurysm was more pronounced in the 30 days group than in the platinum coils, but platinum coils continued to be superior in endothelialization of the neck in this group, although the results in the long-term group were more comparable. Comparing the histologies of the two groups, the only difference being the elapsed time after coiling, the 90 days long-term group showed a higher rate of measured thrombus organization, neoangiogenesis and aneurysmal neck endothelialization than the 30 days short-term group. This is due to the longer duration of the coils being placed in the aneurysm. In contrast, the 30 days group showed a more pronounced intraaneurysmal inflammatory reaction. This, too, can be explained by a decrease in the immune response after a longer period of time and more advanced repair processes in the aneurysms of the 90 days group.
But it also has to be said that more polymer coils in total were used per intervention to seal the aneurysms. So this aspect speaks against our hypothesis that the polymer coils are more thrombogenic than the platinum ones because the goal should be to achieve a tighter packing with fewer coils - due to the higher thrombogenicity ‘in theory’ fewer polymer coils should be needed for complete aneurysm occlusion, but the experiment has shown that potentially more polymer coils are needed. This is not necessarily due to a longer thrombogenicity compared to the normal platinum coils, but rather due to the fact that the polymer coils were so stiff and therefore could not be placed so well and tightly in the aneurysm. This is why several and shorter polymer coils had to be used. The potential of more pronounced thrombogenicity and endothelialization could be demonstrated with individual polymer coils on the aneurysm neck compared to the normal coils.
Conclusion
A complete or almost complete occlusion of the aneurysm was achieved in 92% of animal’s aneurysms treated with the newly developed polymer coil. In animals treated with platinum coils this was achieved in 100% of cases. The flexibility and detachment behaviour of the polymer coil created most of the difficulties and concerns that were encountered in this study. The polymer coils weak points should be eliminated and the polymer coil further developed before having potential for being used in the therapeutic treatment of intracranial aneurysms in humans in the near future.
Finally, it became clear from this study that at the moment novel polymer coils are not a very promising alternative to platinum coils. Especially further improvements in controllability, visibility, flexibility and release behaviour will be necessary – the product developers recognized this and decided to make appropriate modifications. Nevertheless, it could be shown that coils made of polymers can achieve at least in some parameters, especially with regard to histology, comparable results in the treatment of intracranial aneurysms as coils containing platinum but are still overall inferior and cannot be used in human treatment of intracranial aneurysms yet. So they cannot be recommended till now as potential treatment in aneurysm management.
Footnotes
Acknowledgements
Many thanks to Prof. Dr. Med. Michael Menger and all employees of the Institute for Clinical-Experimental Surgery of the Saarland University for supporting this experimental study.
Author contribution
D. Bisharat: Manuscript writing, animal care and operations and angiographic evaluation. J. Johnson: Product development and performance evaluation. R. Mühl-Benninghaus: Animal care and operations. T. Tomori: Animal care and operations. J. Lago: Product development and coiling interventions. R. Virmani: Histopathological evaluation. W. Reith: Project development, interventions and angiographic evaluation. A. Simgen: Animal care and operations, interventions, manuscript writing, angiographic evaluation and statistical analysis.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study has been funded by Nanofiber Solutions Inc. (NFS) from Columbus, Ohio, US and Phenox German Engineering GmbH, headquartered in Bochum, Nordhrein-Westfalen, DE. ORCID iD.
Ethical Standards
We declare that our animal studies have been approved by the ethics committee of the Saarland University and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.