
Abstract
Objectives
To assess the effect of the COVID-19 pandemic on the proportion of abnormal paediatric neuroimaging findings as a surrogate marker for potential underutilisation.
Methods
Consecutive paediatric brain MRIs performed between March 27th and June 19th 2019 (Tbaseline) and March 23rd and June 1st 2020 (Tpandemic) were reviewed and classified according to presence or absence and type of imaging abnormality, and graded regarding severity on a 5-point Likert scale, where grade 4 was defined as abnormal finding requiring non-urgent intervention and grade 5 was defined as acute illness prompting urgent medical intervention. Non-parametric statistical testing was used to assess for significant differences between Tpandemic vs. Tbaseline.
Results
Fewer paediatric MRI brains were performed during Tpandemic compared to Tbaseline (12.2 vs 14.7 examinations/day). No significant difference was found between the two time periods regarding sex and age (Tbaseline: 557 females (44.63%), 7.95 ± 5.49 years, Tpandemic: 385 females (44.61%), 7.64 ± 6.11 years; p = 1 and p = .079, respectively). MRI brain examinations during Tpandemic had a higher likelihood of being abnormal, 41.25% vs. 25.32% (p<.0001). Vascular abnormalities were more frequent during Tpandemic (11.01% vs 8.01%, p = .02), congenital malformations were less common (8.34% vs 12.34%, p = .004). Severity of MRI brain examinations was significantly different when comparing group 4 and group 5 individually and combined between Tbaseline and Tpandemic (p = .0018, p < .0001, and p <.0001, respectively).
Conclusions
The rate of abnormality and severity found on paediatric brain MRI was significantly higher during the early phase of the pandemic, likely due to underutilisation.
Introduction
COVID-19 caused a dramatic change in healthcare utilisation throughout the world. Medical services were redirected and there was a marked ramp-down in non-emergency care with deferrals of non-urgent/non-emergent imaging examinations. Behaviours of patients and their families regarding seeking of healthcare also markedly changed due to stay-at-home directives and fears regarding acquiring COVID-19 in the healthcare environment. This collateral impact on healthcare utilisation is a source for concern and has been characterised across various healthcare contexts, spanning from emergency medicine 1 to outpatient diagnostic imaging. 2 In the USA, the majority of diagnostic imaging groups saw an unprecedented drop in their volume of greater than 50%, spanning both inpatient and outpatient settings, but most marked in the latter, where there was an approximate 70% drop in imaging. 2 In many settings, providers were urged to reschedule non-urgent outpatient visits following national or provincial regulations. 3 In the emergency setting, the COVID-19 pandemic led to a sharp decrease in presentations to adult and paediatric emergency departments around the world.4,5 This is likely the result of advice given to the general public to stay at home and a desire to avoid environments with potentially large numbers of COVID-19 cases. 4 Such a decrease in utilisation of emergent healthcare raises concern about late presentation and increased severity of acute pathology. For example, a study from the USA revealed a 39% decrease in neuroimaging for acute stroke during the period of the pandemic, when compared to pre-pandemic levels. 6 Further studies have demonstrated a more general reduction in emergent neuroimaging. A Canadian group demonstrated reduced use of head computed tomography during the pandemic (10.4 scans/day vs 16.5 scans/day, p = .001). 7 This study also revealed a higher frequency of acute findings on CT during the pandemic compared to prior (p = .001). 7 Similar concerns regarding delays in presentation exist in paediatrics. A review of 4075 physicians in the United Kingdom and Ireland revealed that 32% of responding physicians had witnessed delays in presentation. 5 The most frequently encountered delayed diagnoses included diabetes mellitus (diabetic ketoacidosis), sepsis, child protection, malignancy, and appendicitis, 5 all of which are potentially life-threatening diagnoses.
To the best of our knowledge, there is no current data that characterises the impact of the COVID-19 pandemic on diagnostic imaging of paediatric neurological disorders. We hypothesized that the rate of abnormal brain MRI findings may serve as a proxy for underutilisation and that the rate of abnormal brain MRI findings would be higher during the pandemic. We therefore aimed to assess the rate of abnormal brain MR imaging findings at a quaternary paediatric specialist hospital before and during the early phase of the pandemic.
Material and methods
Study population
This retrospective study was approved by the research ethics board of *** (# 1000073627). In light of the retrospective nature of the study, the requirement for informed consent was waived by the local research ethics board. All patients undergoing MRI of the brain at *** were identified from the local picture archiving and communication system (PACS) database. Two time periods were used, to provide the pre-pandemic and pandemic groups respectively. All studies from March 27, 2019 to June 19, 2019 were considered the pre-pandemic group (Tbaseline, 85 days) and the pandemic cohort was from March 23, 2020 to June 1, 2020 (Tpandemic, 71 days). All patients undergoing brain MRI aged between 0 and 18 years of age were included in the study, with no exclusion criteria. Basic demographic data was collected directly from PACS, including age and sex of all patients.
MRI Acquisition
The entire study population underwent clinical brain MRI at 1.5T or 3T across various scanners (Achieva and Ingenia, Philips Healthcare; Magnetom Skyra, Magnetom Avanto fit, Siemens Healthineers) with a dedicated head-coil. Standardised departmental protocols were used throughout. These usually included a 3D T1-weighted sequence (sagittal or axial), coronal T2-weighted spin echo sequence, axial T2 FLAIR sequence, and axial DWI. These protocols were further customised with addition of various sequences according to the specific clinical indication, such as haemorrhage sensitive sequences, contrast-enhanced sequences and MR-angiographic and MR venographic sequences. Both non-sedate and general anaesthesia MRI examinations were included in the study groups.
Imaging classification
The imaging studies across both cohorts were reviewed to assess for the presence or absence of abnormal findings. Abnormal findings were categorised according to severity using a numerical scale (grade 0 – normal, grade 1 – incidental finding of no clinical significance, grade 2 – previously known and stable non-urgent abnormal finding, grade 3 – previously unknown and non-urgent abnormal finding, grade 4 – previously known or unknown abnormal finding requiring non-urgent intervention and grade 5 – acute illness prompting urgent medical intervention). Furthermore, the abnormal findings were categorized according to the principal pathology. Seven different disease categories were defined: 1 – trauma, 2 – vascular abnormalities, 3 – neoplastic lesions, 4 – infectious, inflammatory, and demyelinating conditions, 5 – hydrocephalus and shunt-related disorders, 6 – congenital malformations, and 7 – toxic, metabolic and degenerative disorders.
Statistical analysis
Statistical analysis was conducted using SPSS RStudio (2020) data analytical software RStudio: Integrated Development for R. RStudio, PBC, Boston, MA URL http://www.rstudio.com/). All tests were non-parametric tests, Pearson chi-squared test and Wilcoxon rank sum test with continuity correction (two tails) were used to compare disease severity and abnormal finding between pre-pandemic and pandemic groups and two-tailed. Observed differences were considered statistically significant when p ≤ .05.
Results
Study population
A total of 2,111 children undergoing brain MRI across the two study periods were included in the analysis, with no exclusions. Of these, 1,248 were within the pre-pandemic time period Tbaseline and 863 within the pandemic time period Tpandemic (2020). This corresponded to an average of 14.7 and 12.2 MRI examinations of the brain per day including weekends and holidays, respectively. There was no statistically significant difference in sex and age distribution between the groups: Tbaseline 557 females (44.63%), 7.95 ± 5.49 years; Tpandemic 385 females (44.61%), 7.64 ± 6.11 years; p = 1 and p = .079, respectively.
Severity and pathology
Distribution of normal and abnormal studies across the two cohorts.
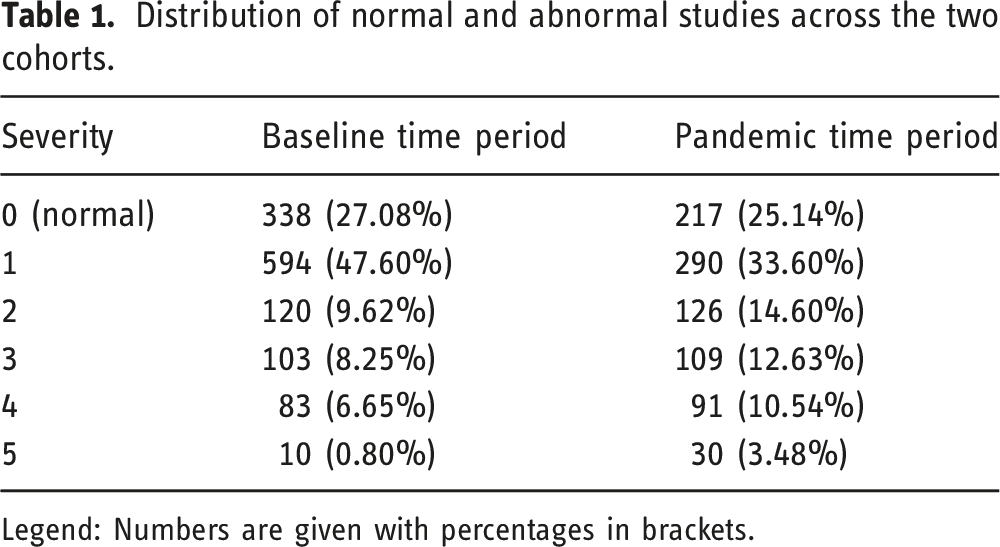
Legend: Numbers are given with percentages in brackets.
Severity of MRI brain examinations was significantly different when comparing group 4 and group 5 individually and combined between Tbaseline and Tpandemic. The proportion of examinations graded as group 4 was significantly lower in Tbaseline compared to Tpandemic: 83 examinations (6.65%) in Tbaseline compared to 91 examinations (10.54%) in Tpandemic, p=.0018. The proportion of examinations graded as group 5 was significantly lower in Tbaseline compared to Tpandemic: 10 examinations (0.8%) in Tbaseline compared to 30 examinations (3.48%) in Tpandemic, p<.0001. The proportion of examinations graded as group 4 and 5 was significantly lower in Tbaseline compared to Tpandemic: 93 examinations (7.45%) in Tbaseline compared to 121 examinations (14.02%) in Tpandemic, p<.0001.
Distribution of etiological classification across the two cohorts.
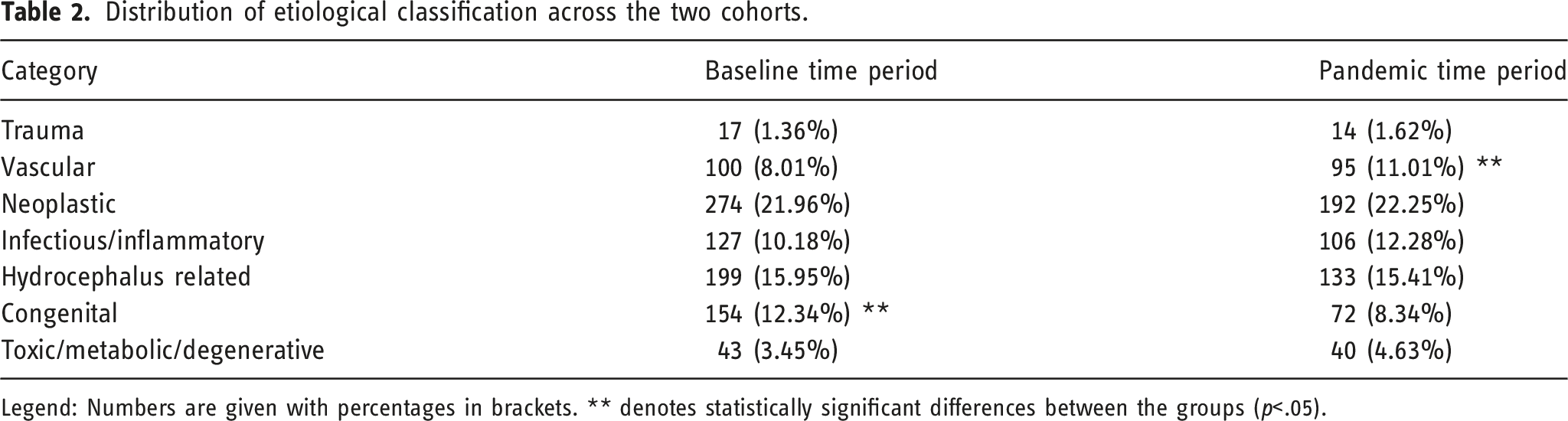
Legend: Numbers are given with percentages in brackets. ** denotes statistically significant differences between the groups (p<.05).
Discussion
Our study demonstrated a significantly higher rate of abnormal findings on brain MRI in a paediatric population during the early phases of the pandemic compared to a comparable time period in the year before. This included a significantly higher rate of clinically relevant abnormal findings requiring intervention. The number of MRI examinations of the brain was lower during the pandemic time period, which is in line with reports from general and adult hospitals that described a markedly reduced throughput of diagnostic imaging examinations during the early stages of the pandemic,2,8 both in the context of emergent and routine care. To our knowledge, this is the first demonstration of this in paediatric neuroradiology.
Our significantly higher rate of abnormal findings on brain MRI is in line with results from the adult literature. A multisite study assessing the use of emergent CT head examinations during the pandemic revealed that the volume of examinations dropped significantly and examinations performed during the pandemic were more likely to be abnormal and display acute findings. 7 Our data extends these findings into paediatric neuroradiology, covering both emergent and routine practice.
A reduction in imaging volumes has manifold adverse consequences on healthcare delivery. Potential considerations include delays in diagnosis, the economic impact on healthcare organisations and the resultant backlog in appointments. 9 The reasons for the observed changes in neuroimaging may be multifold. Firstly, they may reflect altered health seeking behaviour on behalf of the patients. Given international mandates to stay at home and redirection of healthcare facilities towards COVID-19, the patients’ and caregivers’ threshold for seeking medical attention may have altered. In addition, referring physicians likely altered their assessment models and decision making regarding when to proceed with imaging studies. In addition, many states, provinces, or countries issued mandates to defer elective examinations and procedures during the early stages of the pandemic.
When analysing our data according to different etiological groups, the incidence of most disorders was comparable across the groups. Previous work has shown that referrals to exclude traumatic injury decreased during the pandemic. 7 Our study does not confirm this finding. There are several possible reasons for this. Generally, the threshold for considering neuroimaging for trauma patients may be higher in the paediatric context, so that the baseline rate of abnormalities may be higher, blunting the effect of the pandemic. Also, in our study, we assessed MRI of the brain, while the prior study assessed CT in an adult healthcare setting.
Whilst there was no difference across the majority of etiological groups, vascular abnormalities were significantly more commonly observed on MRI of the brain during the pandemic and congenital malformations were significantly less commonly seen. The latter finding is favoured to reflect altered patterns of health seeking behaviour and decision making regarding referrals. It is likely that MRI examinations in a patient with longer standing symptoms were more likely to be deferred in the early stages of the pandemic. The increase in vascular findings can be explained by the fact that they commonly present acutely, which would necessitate medical attention regardless of the pandemic.
There are some limitations to consider when interpreting the results of this study. First, the length of the study periods is slightly unequal between the pre-pandemic and pandemic time periods. Also, a larger number of MRI examinations of the brain was performed in the pre-pandemic time period. Our analyses therefore focused on proportions rather than absolute numbers. Second, there is a degree of subjectivity in our severity grading scale which may have led to bias and there was no assessment of interobserver reliability. However, the majority of information needed to perform the severity grading was obtained from the electronic medical records/radiological reports, which limits the degree of the bias regarding image interpretation. Third, patients may have had combined pathology but were categorized according to their main pathology only.
Conclusion
Our study demonstrated a significantly higher rate of abnormal findings on brain MRI in a paediatric population, including clinically relevant abnormal findings requiring intervention, during the early phases of the pandemic compared to a comparable time period in the year before. This data provides further characterisation of the significant collateral effect the COVID-19 pandemic has had upon healthcare delivery. The far-reaching consequences have been felt across all spheres of healthcare delivery and the impact for organisations and individuals is likely to be long-lasting. Future studies are needed to demonstrate normative values for the rate of abnormal findings of various imaging examinations with deviations denoting under- or overutilisation of imaging.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.