
Abstract
Clear cell sarcoma of the kidney (CCSK) is a rare primary renal tumor in children. It is known for its propensity to metastasize to bones and lungs at initial diagnosis. Distant metastatic relapses occur in about 15–16% of the patients, with the brain being the most frequent site of relapse. Imaging features of brain metastases from CCSK have only been reported in a few cases and most reports lack a detailed description of the imaging findings. We present brain magnetic resonance imaging (MRI) findings in an infant with relapsed CCSK who developed multiple parenchymal metastases with concentric signal alterations and no tumor-associated edema.
Keywords
Introduction
CCSK represents only 2–5% of all primary renal tumors in children. It carries a worse prognosis than Wilms tumor, with higher rates of bone metastases at initial diagnosis and higher rates of distant metastatic relapses. About 41% of distant metastatic relapses occur in the brain. Brain metastases have been suggested to stem from the regrowth of micrometastases that are present at an earlier stage. With the intensive chemotherapy that CCSK patients currently receive, the brain has become the most common site of distant metastatic relapse, probably due to the relative protection of the brain micrometastases from the treatment.1,2
Even though the brain is the most common site of relapse, overall, only 7% of children with CSSK develop relapses in the brain. 1 Because of the rarity of the condition, imaging findings of the metastatic brain lesions from CSSK have been reported in only a few cases, mostly without a detailed imaging description. 3 One case report indicated that the brain metastases from CCSK can have unusual imaging features for the metastatic brain lesions from extracranial solid tumors, such as the absence of metastasis-associated edema or contrast-enhancement, and a seemingly extra-axial location. 4 As MRI of the brain is being increasingly included in imaging screening and follow-up of patients with CCSK, knowledge of unusual imaging features of these metastatic lesions may aid in their early recognition.
Case report
Following the CARE guidelines, parental consent was obtained for the publication of this case
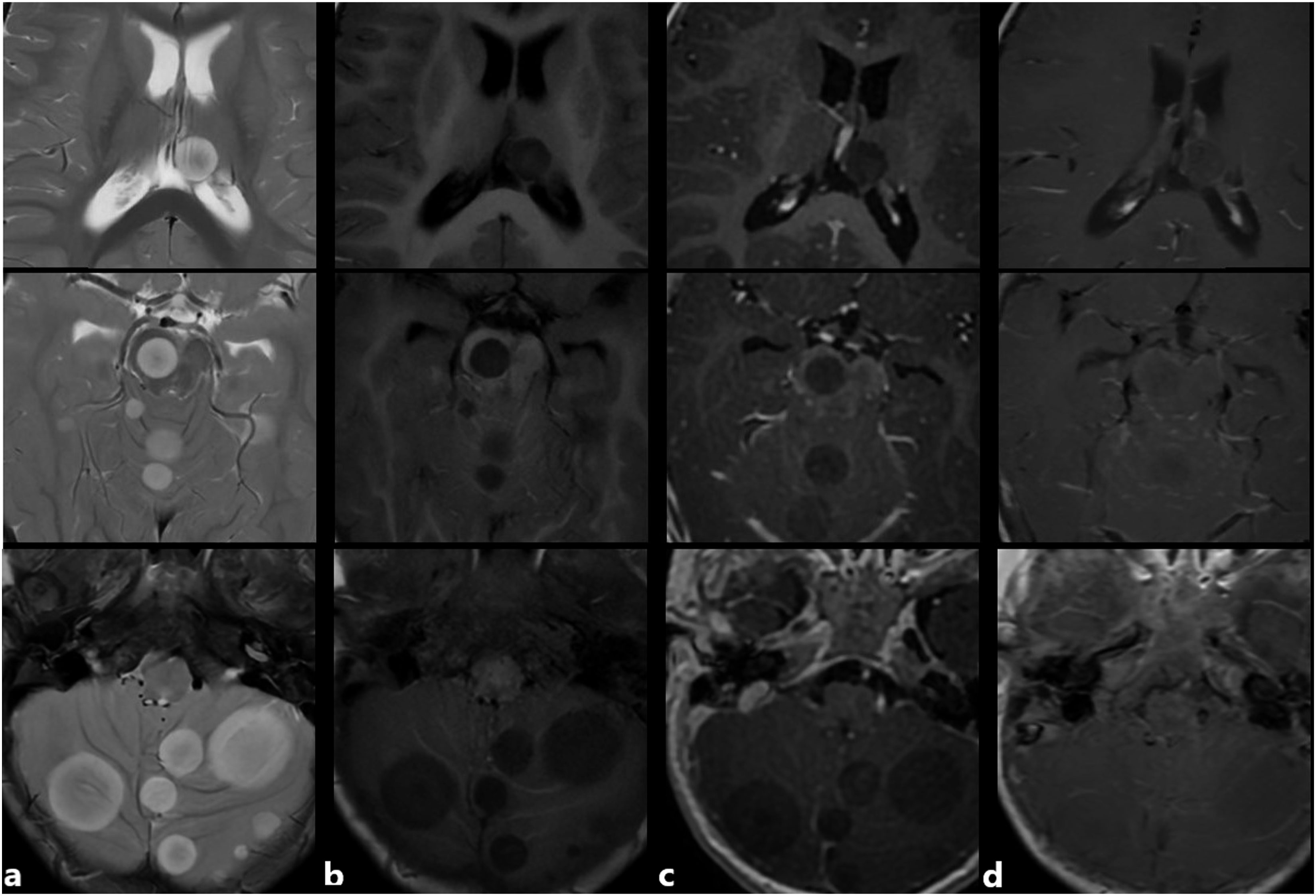
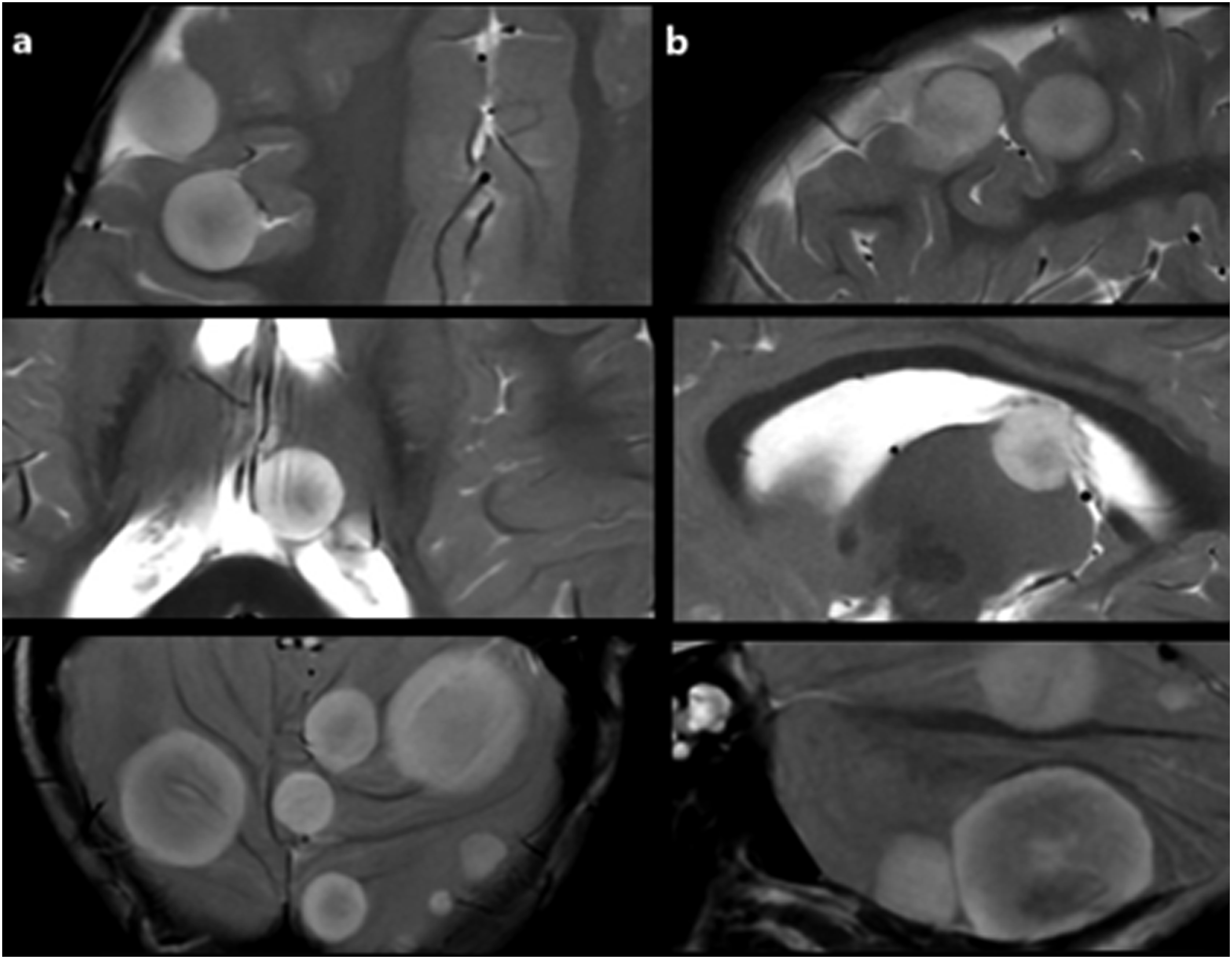
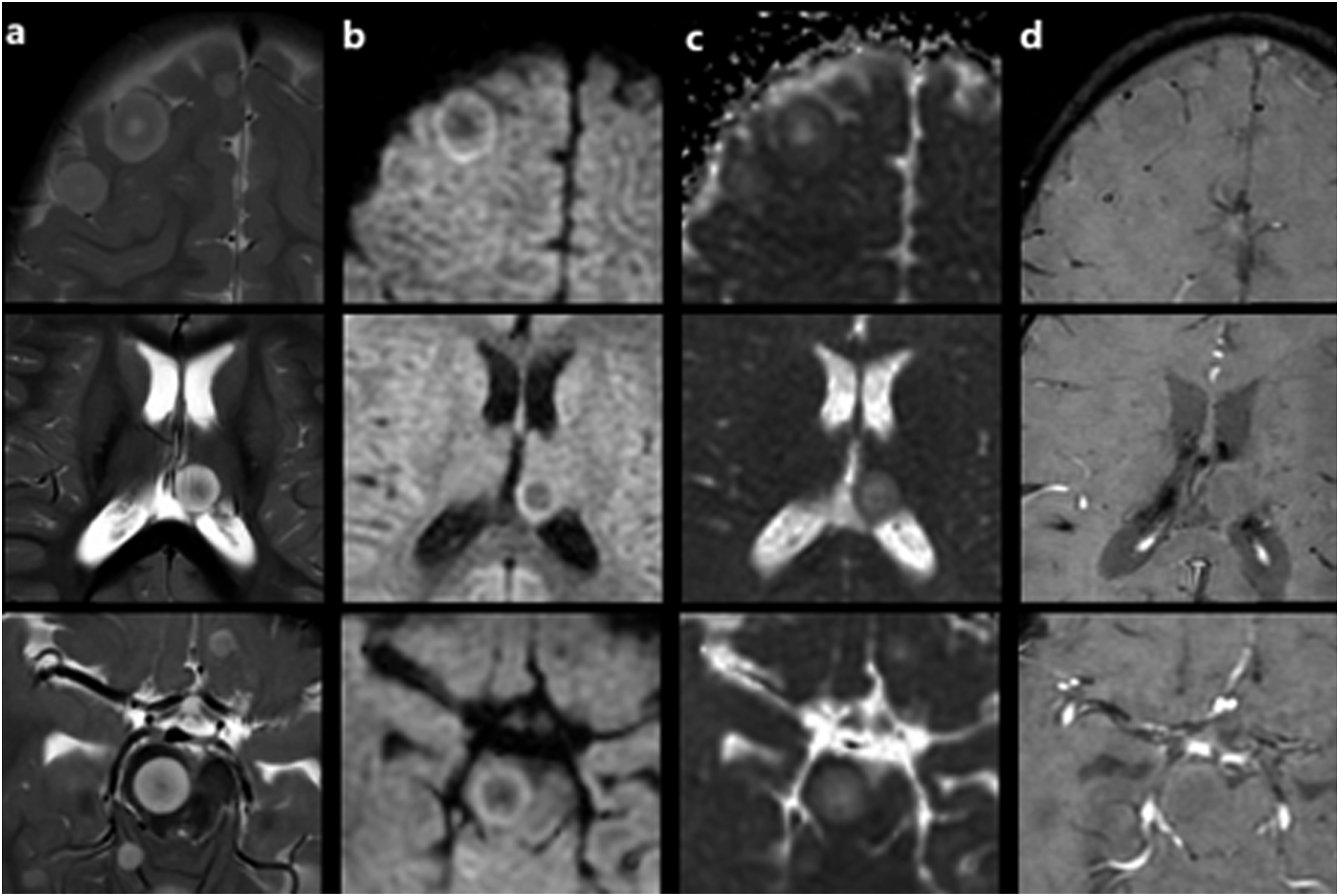
At the end of the protocol, the patient had no complaints or symptoms. A follow-up MRI of the brain at 3T obtained 8 months after the diagnosis showed multiple well-defined rounded lesions of various sizes on the cerebral hemispheres, basal ganglia, thalamus, brain stem, and cerebellum. Most of the lesions exhibited alternating circular layers of high and low signal intensities on T2-weighted fast spin echo (SE) and T1-FLAIR images, giving them a targetoid appearance. None of the lesions showed tumor-associated vasogenic edema (Figure 1). On post-contrast, 3D T1W spoiled gradient recalled (SPGR) images most lesions showed faint enhancement of their T2 hypo- and T1 hyperintense layers. Post-contrast T1W SE images demonstrated faint but relatively diffuse enhancement of most lesions (Figure 2). Some peripheral metastatic lesions seemed to be located extra-axially at first view. A multiplanar evaluation demonstrated that the lesions were located intra-axially on the cortex-subcortical white matter interfaces and were displacing the white matter tracts inwards (Figure 3). Diffusion-weighted (DW) images showed relatively restricted diffusion of the outer T2 hyperintense signal layers. Susceptibility-weighted images did not show any apparent signal abnormalities (Figure 4). As subsequent imaging studies demonstrated synchronous metastatic bone and lung disease, and the parents declined further diagnostic or therapeutic procedures, the brain lesions were not biopsied (Supplementary File 3). T2W FSE (TR:7700, TE: 102, 4 mm) T2W T2W appearances of the metastatic lesions on axial Axial T2W 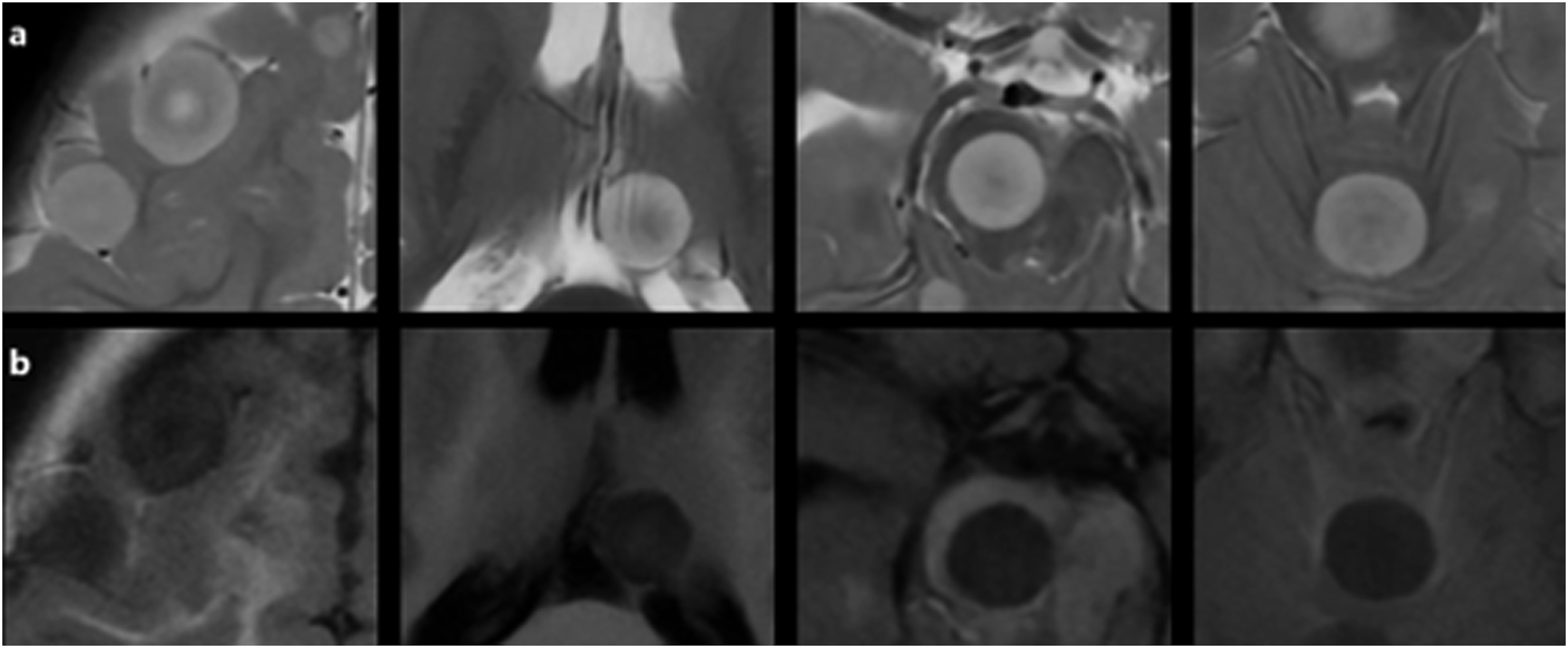
Discussion
The reports with T2W MR images have described the parenchymal metastatic lesions from CSSK as large, peripherally located, hyperintense tumors with mass effect. The presence or absence of peritumoral vasogenic edema was not mentioned in those reports.3,5 The absence of peritumoral edema in a metastatic brain lesion from CCSK has been reported so far by Shajpaul et al. 4 A single large-sized frontal hemispheric metastatic lesion, in that case, showed no tumor-associated edema and no contrast-enhancement. Those features have been attributed to the poor vascularity and cellularity of that metastatic lesion by the authors, reflecting the histopathology of the primary tumor. Although large-sized intraparenchymal metastases of the brain mostly exhibit vasogenic edema, the presence or degree of vasogenic edema may be influenced by other factors than the lesion size, such as the primary tumor type, location of the lesion in the gray or white matter, desmoplastic effects of the chemotherapy, and the presence or absence of reactive astrogliosis around the lesion.4,6 As the histopathological evaluation of the metastatic brain lesions in the presented case was not performed, addressing the exact cause of the absence of the peritumoral edema is not possible. A faint contrast-enhancement of the metastatic lesions, however, might be due to the lesions’ poor vascularity and the signal alteration layers with T2 hypointensity and T1-FLAIR hyperintensity within the lesions might suggest the presence of relatively hypocellular fibrotic components. The hemispheric metastatic lesions in the presented case were located at the gray-white matter interfaces; however, they exhibited an asymmetrical growth pattern into the cortex toward the cerebrospinal fluid. That growth pattern of the lesions might also have restricted the development of vasogenic edema. Non-visualization of the nearby cerebral cortex and absence of surrounding vasogenic edema gave some of the lesions a seemingly extra-axial appearance. In the case report by Shajpaul et al., 4 the large-sized frontal metastatic lesion was also presumed to be located extra-axially on the initial CT scan. A subsequent MRI showed the lesion’s true intra-axial location and a resection showed that the lesion was attached to the overlying dura but not originating from it.
Alternating concentric signal intensity changes in MRI of metastatic brain lesions from CCSK have not been reported before. The target sign describes central hypointensity and peripheral hyperintensity on T2W images in a lesion. Observance of that sign in most metastatic lesions in the present case might be due to the simultaneous presence of circularly arranged fibrotic and fluid-rich components, represented by T2 hypointense and T2 hyperintense signal changes, respectively. Interestingly, Shajpaul et al. 4 have described the presence of a metastasis-associated cyst on CT, as a rim of hypodensity surrounding the solitary metastatic lesion. The cystic appearing part of the lesion corresponded to the avascular lesion surface at resection. Although not mentioned in the report, the presented T2W image in that case also demonstrates a circular hypointense inner layer. The T2 hyperintense signal layers in the case we present showed some degree of contrast-enhancement and exhibited relatively low ADC signal, thus, were not truly cystic.
Despite the similarities between the imaging features of the presented case and Shajpaul et al.’s 4 case, the metastatic brain lesions from CSSK do not seem to have a common or typical imaging appearance, as Park et al. 7 have reported two large-sized, intensely enhancing, dura-based extra-axial metastatic lesions at relapse and Zekri et al. 8 have reported metastatic involvement of the brain from CSSK as diffuse leptomeningeal thickening and enhancement.
The presented imaging findings of the metastatic lesions in this report indicate that early detection of the described lesions may be difficult due to the absence of perilesional vasogenic edema, the outward growth pattern of the lesions from the gray-white matter junction, and faint enhancement of most lesions on post-contrast T1W SE images. That may be particularly true if the myelination of the subcortical white matter is not completed. Including 3D T2W and 3D gradient recalled T1W images in follow-up brain MRI protocols of the patients with CCSK may increase the early detection of such metastatic lesions.
Supplemental Material
Supplemental Material - Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report
Supplemental Material for Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report by Çiğdem Öztunalı, Ersin Töret, and Zeynep Canan Özdemir in The Neuroradiology Journal
Supplemental Material
Supplemental Material - Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report
Supplemental Material for Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report by Çiğdem Öztunalı, Ersin Töret, and Zeynep Canan Özdemir in The Neuroradiology Journal
Supplemental Material
Supplemental Material - Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report
Supplemental Material for Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report by Çiğdem Öztunalı, Ersin Töret, and Zeynep Canan Özdemir in The Neuroradiology Journal
Supplemental Material
Supplemental Material - Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report
Supplemental Material for Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report by Çiğdem Öztunalı, Ersin Töret, and Zeynep Canan Özdemir in The Neuroradiology Journal
Supplemental Material
Supplemental Material - Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report
Supplemental Material for Brain metastases with unusual MRI features in an infant with relapsed clear cell sarcoma of the kidney: A case report by Çiğdem Öztunalı, Ersin Töret, and Zeynep Canan Özdemir in The Neuroradiology Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.