
Abstract
Thrombophlebitis is a known complication of head and neck infection, which can result in propagation of infected thrombi and associated complications. While antegrade/downstream propagation of thrombus is well described—the Lemierre syndrome—thrombophlebitis can spread in atypical patterns which has specific diagnostic and treatment considerations. In this series, we highlight 6 cases of atypical thrombophlebitis patterns complicating head and neck infection, 5 of which extend intracranially. Through these pathways, head and neck infections such as oral cavity, oropharynx, or skin can be the culprit of remote, including intracranial, complications, which may be overlooked. Furthermore, understanding pathways of venous drainage and communication can help accurately diagnose thrombophlebitis patterns and associated complications.
Introduction
Thrombophlebitis is a known complication of head and neck infection, typically involving the internal jugular vein (IJV). Infected thrombi can then propagate either antegrade or retrograde resulting in distant complications. Antegrade propagation of IJV thrombophlebitis following oropharyngeal infection by Fusobacterium Necrophorum resulting in pulmonary and systemic emboli is classically described as Lemierre syndrome. 1 Atypical patterns of propagation of thrombosis, including cephalad and against the normal direction of venous flow, can occur through various head and neck venous drainage pathways resulting in remote orbital and intracranial complications. Although there are considerable variations in venous drainage, understanding these pathways can help accurately localize sites of thrombophlebitis and detect its associated complications.
Furthermore, while the paranasal sinuses, mastoid temporal bones, and the skull base are usual culprits for intracranial extension of head and neck infection, the venous system allows for primary infections in sites such as the oropharynx, oral cavity, or skin to result in intracranial complications and therefore must be recognized by the interpreting radiologist. We report six cases of atypical propagation of thrombophlebitis from head and neck infection, five of which extend intracranially (Table 1).
Case 1
A 16-year-old male with fever and sore throat for a week treated with antibiotics, presenting with headache, dysarthria, right sided facial pain, and swelling. Physical examination revealed mild right ptosis from a partial right third cranial nerve palsy and proptosis.
Magnetic resonance imaging (MRI) demonstrated inflammatory changes in the right oropharynx (Figure 1) extending to the deep spaces of the neck with ascending thrombophlebitis extending through the right pterygoid venous plexus to the right cavernous sinus and right superior petrosal sinus. There was associated right cavernous and supraclinoid internal carotid artery (ICA) irregularity. MRI demonstrates edema surrounding the right palatine tonsil, extending to the right parapharyngeal and parotid spaces (Figure 1(a)), ascending thrombophlebitis involving the right pterygoid venous plexus (Figure 1(b)), extending to the right cavernous sinus and superior petrosal sinus (Figure 1(c)) with low diffusivity (not shown). There is associated narrowing of the right cavernous and supraclinoid internal carotid artery (Figure 1(d)).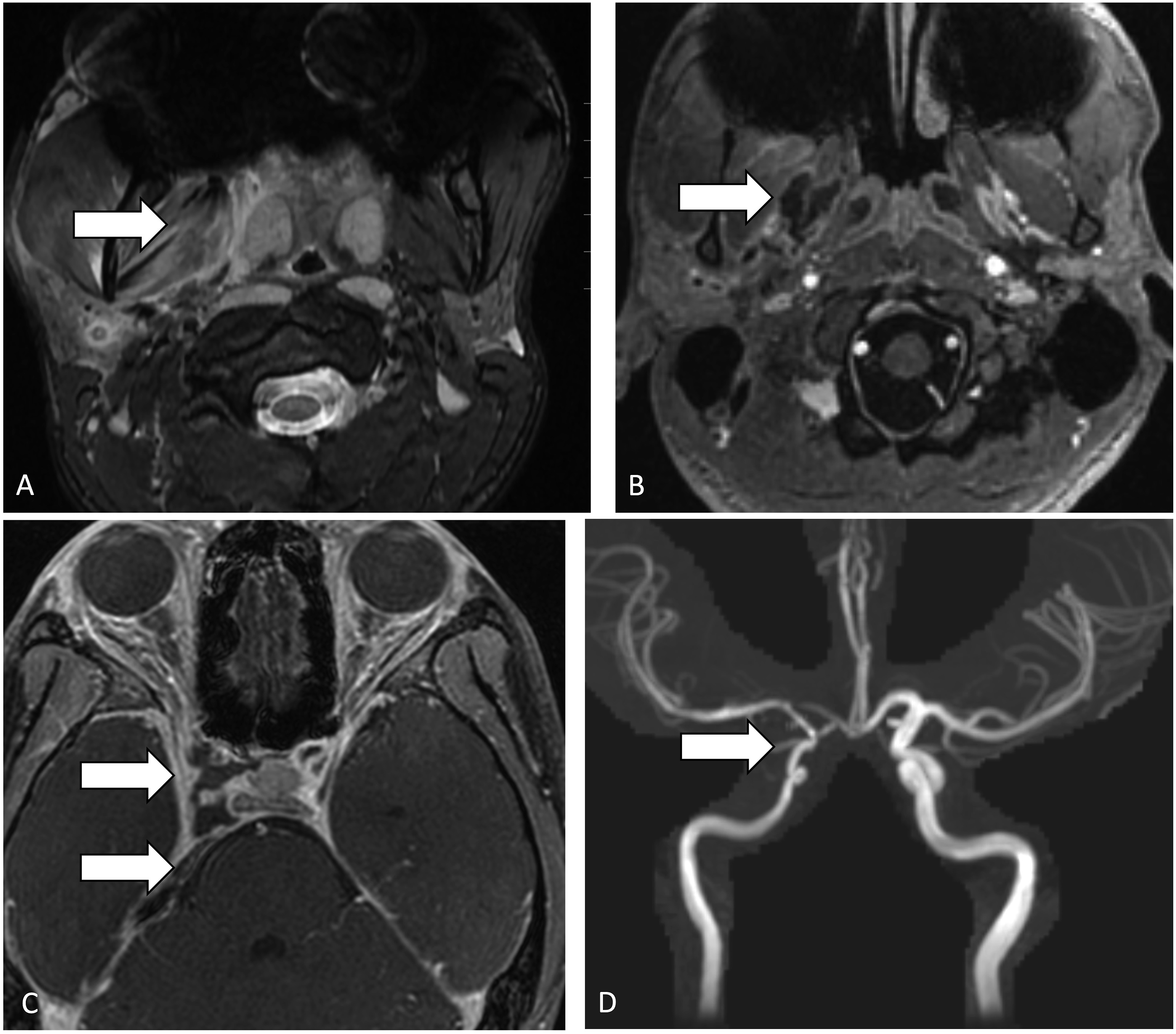
Blood culture and cerebrospinal fluid (CSF) metagenomic next generation sequencing were positive for F. Necrophorum. The patient was started on meropenem and metronidazole with clinical improvement. He completed 4 weeks of antibiotics, short-term anticoagulation with enoxaparin which was later transitioned to aspirin for 1 year. The patient responded well with resolution of ICA irregularity and no residual headaches or ptosis on follow-up.
Case 2
A 23-year-old female with left eye swelling and diplopia for 1 week, then developed headache and neck stiffness and was diagnosed with orbital cellulitis and meningitis. While on antibiotics, the patient developed progressive multiple cranial neuropathies. Neurologic examination revealed decreased visual acuity on the left, left third, fourth, sixth, and right sixth cranial nerve paralysis.
MRI demonstrated left tonsillar abscess (Figure 2) with associated retrograde thrombophlebitis extending through the pterygoid venous plexus to the left greater than right cavernous sinus and left superior ophthalmic vein. The patient was being treated for orbital cellulitis and the oropharynx was not initially recognized as the site of primary infection. There was also narrowing of the bilateral cavernous ICA and associated pseudoaneurysm on the left. This was further complicated by multifocal infarcts in the left ICA territory. The patient additionally had evidence of antegrade propagation of thrombophlebitis with septic emboli to the lung. MRI demonstrates left tonsillar abscess with suppurative retropharyngeal node (Figure 2(a)), retrograde thrombophlebitis to the left greater than right cavernous sinus, and left superior ophthalmic vein (Figure 2(b)). There is associated narrowing of the bilateral cavernous internal carotid arteries with associated pseudoaneurysm on the left (Figure 2(c)) and left caudate head infarct (Figure 2(d)).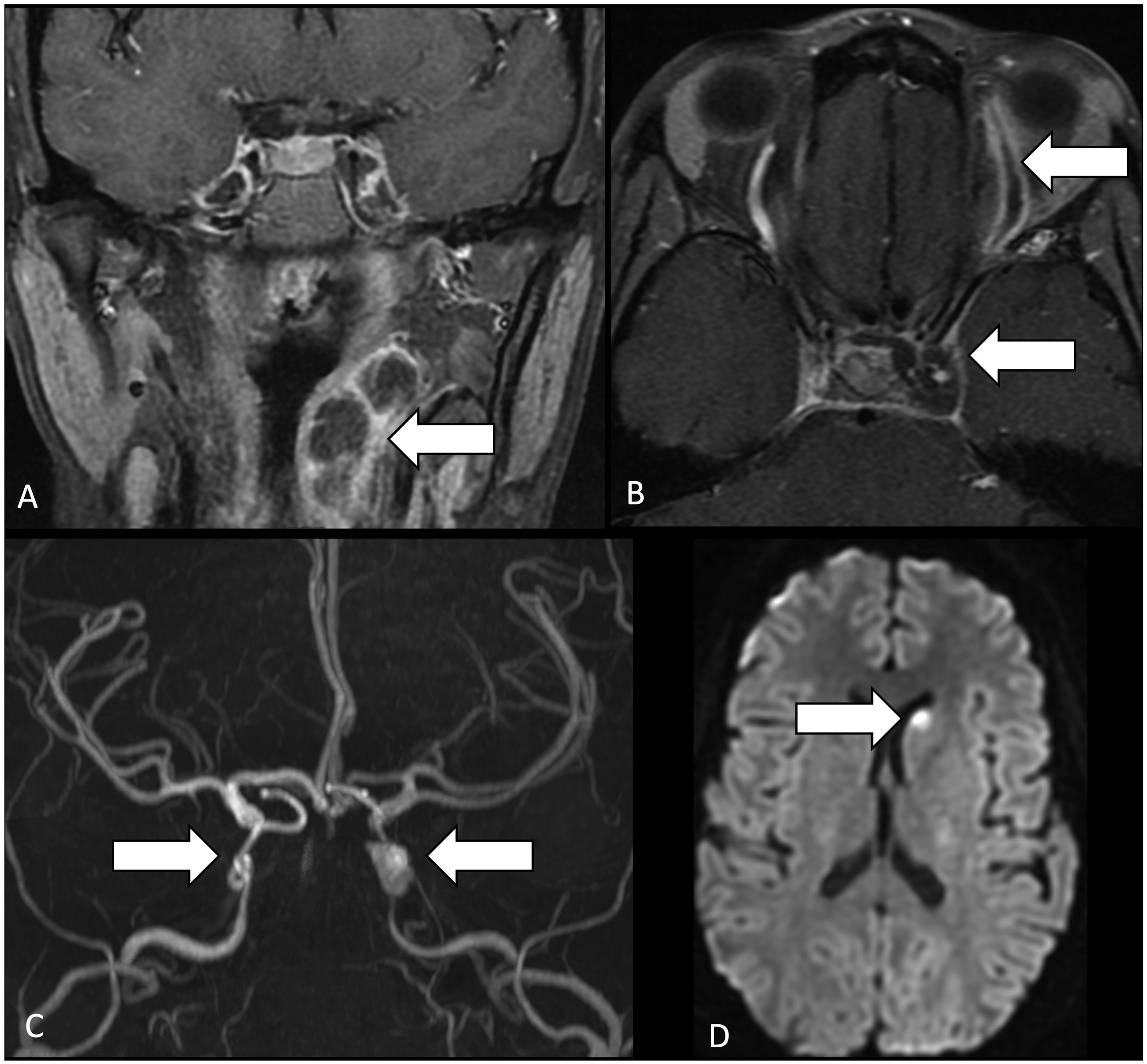
Drainage of the peritonsillar and parapharyngeal abscess was performed with the left tonsil tissue polymerase chain reaction (PCR) positive for Granulicatella adiacens. Blood metagenomic next generation sequencing was positive for F. Necrophorum. The patient was treated with broad spectrum antibiotics for 6 weeks as well as anticoagulation for 3 months. At 2-month follow-up, the patient had slow improvement in vision and improving diplopia.
Case 3
A 17-year-old female with 5 days of fever, sore throat, headache, and episode of syncope. During hospitalization, the patient developed increased submandibular pain and right retroorbital pain. Neurologic examination was non-focal and ophthalmologic examination was normal.
MRI demonstrated inflammatory changes in the right tonsil extending to the deep spaces of the neck, associated thrombosis of the maxillary vein, retromandibular vein, pterygoid venous plexus, right external and internal jugular veins, and cavernous sinus (Figure 3). The patient also developed a pseudoaneurysm of the right cavernous ICA and had evidence of septic emboli to the lung. MRI demonstrates occlusive thrombus of the right external jugular vein and nonocclusive thrombosis of the right internal jugular vein (Figure 3(a)), pterygoid venous plexus, maxillary and retromandibular veins (Figure 3(b)), and the right cavernous sinus (Figure 3(c)). There is associated irregularity, narrowing, and pseudoaneurysm of the right cavernous internal carotid artery (Figure 3(d)). Inflammatory changes in the right tonsil extending to the deep spaces of the right neck are not shown.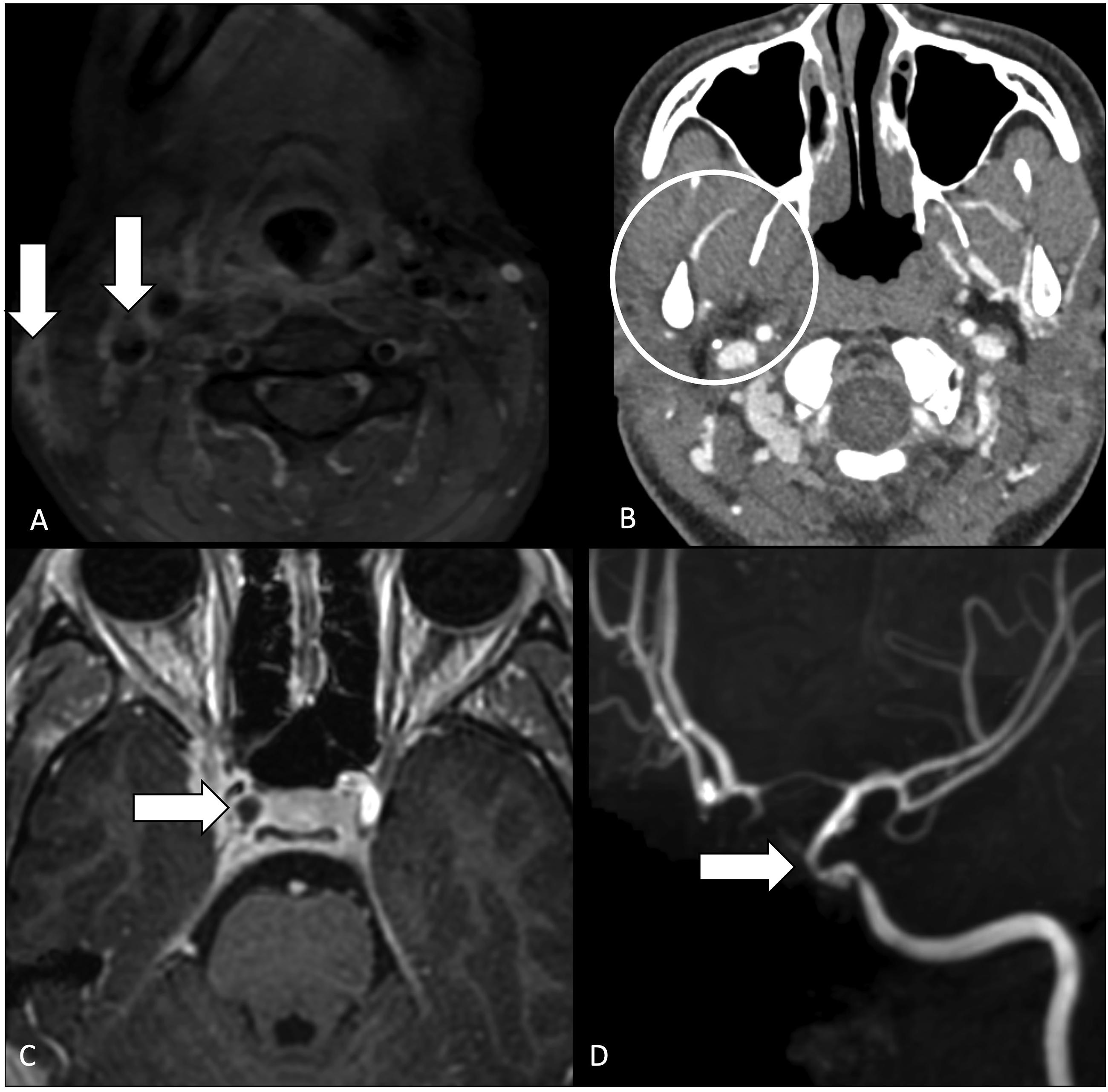
Blood metagenomic next generation sequencing was positive for F. Necrophorum. The patient was treated with metronidazole for 4 weeks and anticoagulation for 3 months. The ICA irregularity and pseudoaneurysm resolved on follow-up imaging. The patient’s symptoms improved with minimal residual headache and dizziness at 2-month follow-up.
Case 4
A 2-year-old previously healthy boy presented with fever and left neck mass. He was started on oral antibiotics, however, neck swelling persisted and was investigated with imaging. Computed tomography (CT) neck (Figure 4) demonstrated suppurative left cervical and retropharyngeal adenopathy. He was then started on intravenous antibiotics and admitted for further management. Two days later, he had persistent fevers and neck swelling and repeat imaging demonstrated worsening cervical abscesses and left internal jugular vein thrombosis extending retrograde to involve the sigmoid sinus (Figure 4). The patient underwent incision and drainage of cervical abscesses, cultures of which grew Staphylococcus Aureus. He improved on intravenous antibiotics, and follow-up imaging demonstrated resolution of abscesses and decrease in thrombus burden. CT neck demonstrates left cervical and retropharyngeal suppurative adenopathy (a) with mass effect on the left internal jugular vein (b), which progresses to thrombosis of left internal jugular vein, extending retrograde to left sigmoid sinus (c).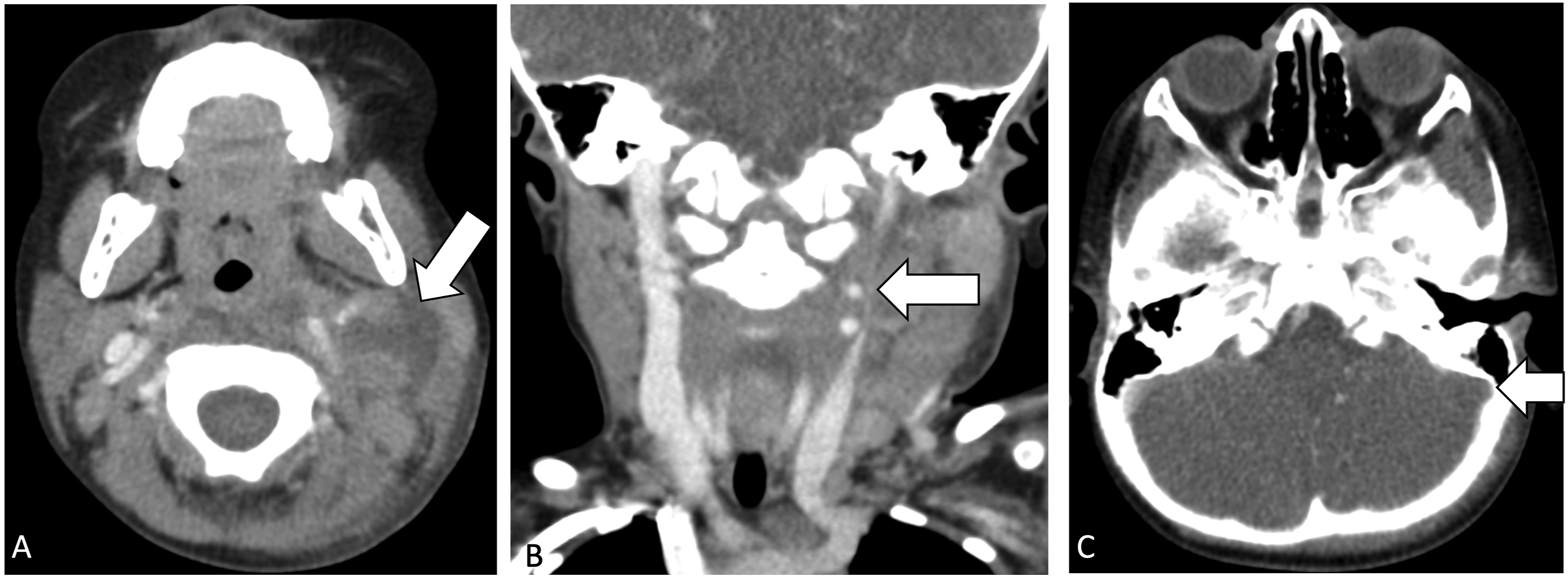
Case 5
A 22-year-old male presented with 5 days of worsening left lower facial pain, chills, and shortness of breath. Clinical exam demonstrated erythema and swelling of the left upper neck, consistent with cellulitis. CT demonstrated thrombosis of the left retromandibular vein with retrograde extension into the left facial vein with surrounding soft tissue stranding (Figure 5). CT chest showed multiple pulmonary infarcts and bilateral pleural effusions requiring chest tubes for drainage. Blood cultures grew F. necrophorum. He was started on intravenous ampicillin-sulbactam with rapid clinical improvement. Axial (a) and Sagittal (b) postcontrast CT demonstrating thrombosis of the left retromandibular vein (arrow) with retrograde extension into the left facial vein (arrow) (c) with surrounding soft tissue stranding.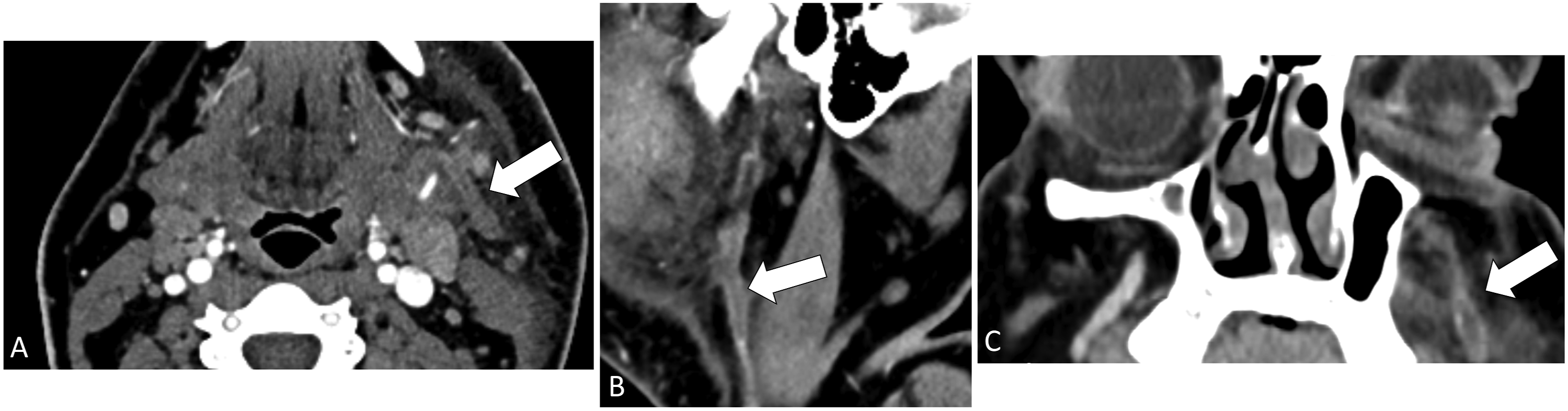
Case 6
A 45-year-old female with history of asthma and dental disease presented with 1 week of worsening dental pain and left facial swelling. CT demonstrated a large odontogenic abscess extending into the parapharyngeal space and thrombosis of the left IJV with retrograde propagation into the left sigmoid sinus (Figure 6). Flexible laryngoscopy demonstrated significant narrowing of the hypopharynx secondary to lateral wall and left arytenoid edema. She was taken emergently to the operating room for incision and drainage and started on intravenous ampicillin-sulbactam, with rapid clinical improvement. Blood cultures grew Streptococcus anginosus, a component of human bacterial oral flora and an unusual but described culprit of septic thrombophlebitis.2,3 Postcontrast CT showing large odontogenic parapharyngeal space abscess (Figure 6(a)) and thrombosis of the left internal jugular vein (Figure 6(b)) with retrograde propagation into the left sigmoid sinus (Figure 6(c)).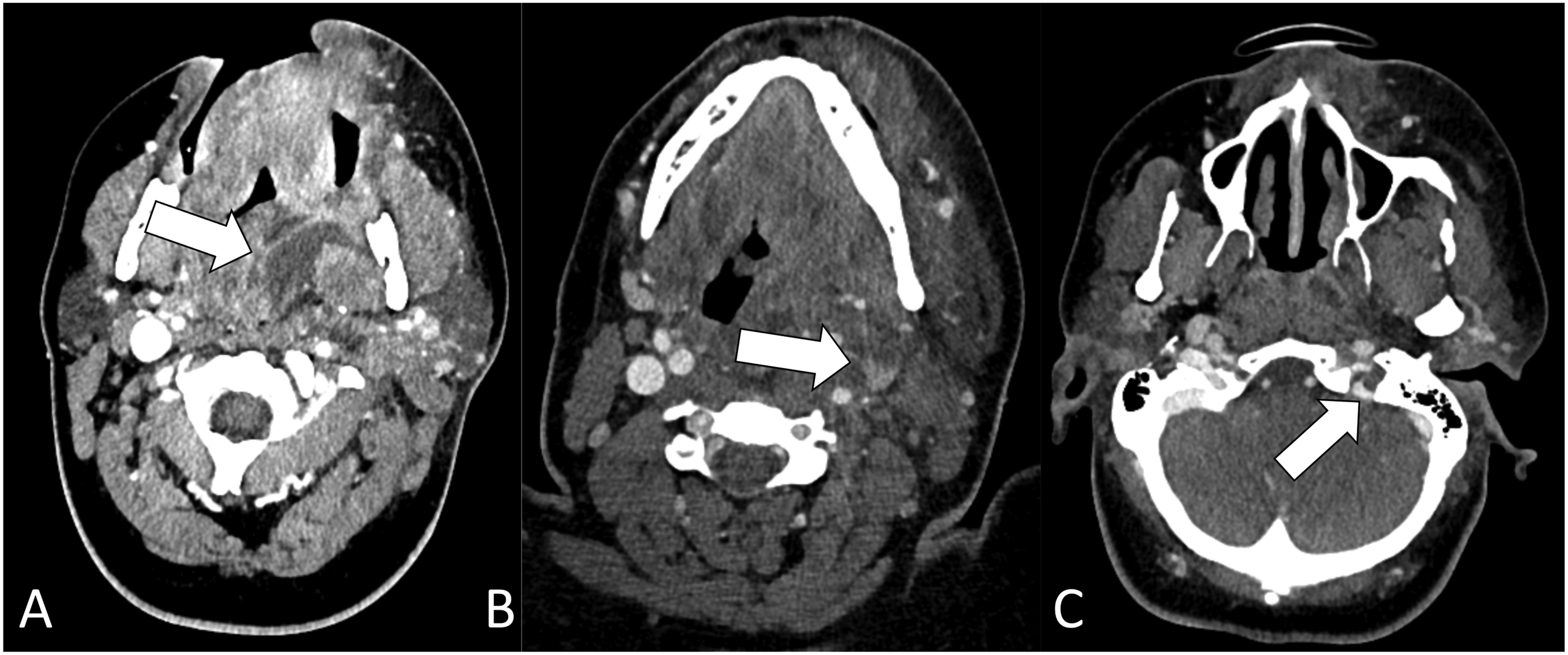
Discussion
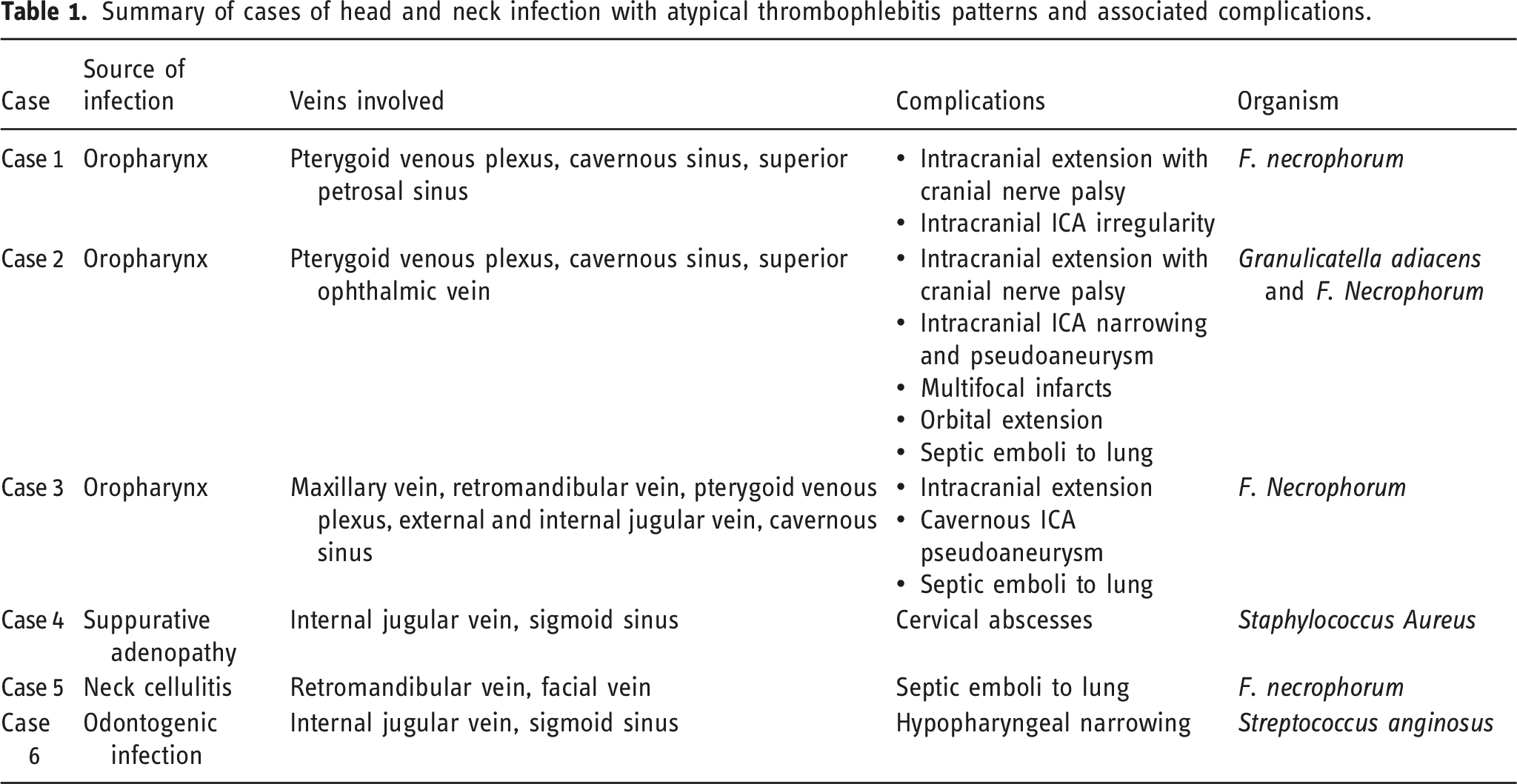
Summary of cases of head and neck infection with atypical thrombophlebitis patterns and associated complications.
There is considerable variation in head and neck venous drainage and multiple pathways exist for intracranial extension of venous thrombophlebitis. 4 Internal jugular vein thrombosis can extend directly to the sigmoid and transverse sinuses. There are complex communications between the facial vein, pterygoid venous plexus, cavernous sinus, external jugular vein and IJV. 4 The facial vein communicates with the pterygoid venous plexus via the deep facial vein. The angular branch of the facial vein drains via the superior ophthalmic vein into the cavernous sinus. 5 The inferior ophthalmic vein drains into both the cavernous sinus and the pterygoid venous plexus, thereby also connecting the two structures. 6 The cavernous sinuses connect with each other via the intercavernous sinuses and ultimately drain via the superior and inferior petrosal sinuses, and emissary veins passing through the skull base foramina to the pterygoid venous plexus. The pterygoid venous plexus drains into the maxillary vein, which joins the superficial temporal vein to form the retromandibular vein. 7 The anterior branch of the retromandibular vein joins the facial vein and drains into the internal jugular vein, while the posterior branch of the retromandibular vein joins the posterior auricular veins to form the external jugular vein. Due to the absence of valves, the direction of flow is determined by pressure gradients which can be reversed in the setting of inflammation or thrombosis resulting in retrograde propagation of thrombosis. 6
The majority of the reported cases of Lemierre syndrome demonstrate descending IJV thrombophlebitis with antegrade propagation of infected thrombi resulting in septic emboli to the lung in 80–90% and septic arthritis in 10–20%. 1 Our case series includes 3 cases of Fusobacterium necrophorum infections of the oropharynx complicated by retrograde thrombophlebitis extending primarily through the pterygoid venous plexus to the cavernous sinus. Oropharyngeal infection causing Lemierre syndrome with retrograde cavernous sinus thrombosis is rare.8–13 Interestingly, as early as in 1912, Long 14 described a patient with fever, chills, and sore throat who developed neck swelling, eye pain, ptosis, and ophthalmoplegia. Long hypothesized the orbital symptoms to be due to “thrombi extended up from the internal jugular vein through the inferior petrosal sinus into the cavernous sinus, possibly higher into the ophthalmic vein, setting up a septic neuritis of the third, fourth, and sixth nerves, the probable point of infection of the nerves being where they traverse the cavernous sinus.” 14
The cases presented here also demonstrate secondary arterial complications of ICA narrowing and/or pseudoaneurysm and orbital complication of superior ophthalmic vein thrombosis. Secondary intracranial arterial complications associated with retrograde venous thrombosis are rare. This can include cavernous ICA narrowing or pseudoaneurysm with or without infarct.15–18 Similarly, orbital complications of Lemierre syndrome are rare. 19 This can include retrograde superior ophthalmic vein thrombophlebitis, ophthalmoplegia from cavernous sinus thrombosis, optic nerve and retinal ischemia,20,21 and orbital abscesses. 22 Other complications of retrograde intracranial extension of thrombophlebitis include venous infarction, cranial neuropathies, and intracranial abscess.
Paranasal sinuses are a well-recognized source of infection resulting in intracranial and orbital complications. Similarly, skull base and mastoid temporal bone infections can also cause intracranial thrombophlebitis. However, retrograde thrombophlebitis can be a mechanism for intracranial extension of remote head and neck infection and these sources might be overlooked. In our series, the initiating oropharyngeal infection was not initially recognized in one case.
In all cases, the mainstay of treatment was source infection control with antimicrobial therapy, with or without surgical drainage of any associated abscess. In three cases with arterial complications, anticoagulation therapy was initiated. Evidence for the role of anticoagulation therapy in Lemierre syndrome is mixed, with some studies suggesting the lack of benefit, while others suggesting benefit provided there is no clinical contraindication to anticoagulation.23,24
Conclusion
This case series highlights several atypical patterns of propagation of thrombophlebitis associated with head and neck infections. Sources of infection beyond the paranasal sinuses and skull base or temporal bone should be considered in patients presenting with intracranial or orbital venous thrombophlebitis and associated complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Elizabeth George was supported by the American Society of Neuroradiology Scholar Award.
Disclosure
This work was presented in part at ASHNR 2020.