
Abstract
Background
Materials and Methods
We retrospectively reviewed records (MRI features, pathology, and survival data) of all patients at our institution with PCNSL who had been seen from, 2007 through 2017, and had undergone pretreatment MRI.
Results
We identified 79 patients (42 men, 37 women) with a mean age at diagnosis of 61.7 ± 10.4 years. The mean OS duration was 44.6 ± 41.7 months. The most common pathological diagnosis (74 patients) was diffuse large B-cell lymphoma. No associations were found between OS time and lesion location, volume, and number; contrast enhancement; necrosis; proximity to the subarachnoid space; or edema. However, a sole patient with non-enhancing PCNSL on MRI was found to have low-grade disease, with prolonged survival (>83 months). Several other patients with leptomeningeal disease had a mean OS time of 80 months. Patients with hemorrhagic lesions had a mean OS of 25.5 months.
Conclusions
The survival time for patients with PCNSL may be longer than previously thought, especially for patients with leptomeningeal seeding and lesions with hemorrhagic components Also, non-enhancing tumors may be less aggressive than enhancing tumors.
Primary central nervous system (CNS) lymphomas (PCNSLs) are aggressive, extranodal non-Hodgkin lymphomas that occur in the brain, eyes, leptomeninges, or spinal cord.1,2 Up to 95% of PCNSLs are classified histologically as diffuse large B-cell lymphoma (DLBCL). 3 Histopathologic diagnosis is determined by biopsy of a CNS lesion, by cerebrospinal fluid cytologic or flow cytometry analysis, or, for intraocular lymphoma, by vitrectomy or chorioretinal biopsy. 2 In most cases, PCNSL is sporadic; however, its incidence increases with age and with immunosuppression, whether iatrogenic after organ transplant or as a result of human immunodeficiency virus infection. 3 Although epidemiologic findings suggest that the prevalence of PCNSL in human immunodeficiency virus–positive patients is decreasing in high-income countries because of the advent of retroviral therapy, the incidence among older people is rising over time, currently at 4.3 per 100,000 for the past decade among patients aged 70–79 years.1,3,4
The mean overall survival (OS) duration of patients with untreated PCNSL, regardless of immune status, is only 1–5 months from diagnosis. 1 The use of chemotherapy and chemoradiotherapy has improved the prognosis for some patients with PCNSL, but disease remissions are brief. 1 One multicenter trial of chemoradiation therapy in 102 patients with PCNSL showed a mean progression-free survival duration of 24 months and a mean OS duration of 37 months. 5 Because the early diagnosis of PCNSL is imperative to optimize treatment outcomes, immediate surgical biopsy is recommended when enhancing brain lesions are found on magnetic resonance imaging (MRI) and when no abnormalities are found on cerebrospinal fluid analysis. 2 The most common differential diagnosis (and closest radiographical mimic) of PCNSL is glioblastoma. Indeed, some patients with PCNSL undergo cytoreductive surgery owing to this mimicry. Although this approach may have a therapeutic benefit in diffuse PCNSL, gross resection is generally not indicated.6–8 Therefore, obtaining intraoperative pathologic findings via frozen section analysis is crucial for excluding PCNSL before continuing with an extensive resection. 8
PCNSL has characteristic findings on imaging. Nearly 90% of lesions are supratentorial and are most often found in the frontal lobe white matter.9,10 PCNSL is often in contact with ependymal or meningeal surfaces, and about 12% of lesions involve the leptomeninges. 9 MRI is the imaging modality of choice for evaluating PCNSL.9,11 On T1-weighted MRI, PCNSL presents as a well-demarcated isointense or hypointense mass relative to gray matter. The appearance on T2 sequences varies, with more than half of tumors being hypointense to isointense relative to the surrounding gray matter. High T2 signal intensity in lesions has been correlated with greater tumor necrosis. 9
PCNSL lesions most often show avid contrast enhancement on T1-weighted contrast-enhanced MRI sequences. However, several case reports have described PCNSL in patients with no enhancement on MRI, 9 and clinical studies have shown that approximately 1% of patients with PCNSL do not have contrast-enhancing lesions.9,12 This observation, plus other similar cases encountered in our clinical practice, prompted us to review PCNSL images at our institution to determine whether survival duration was related to tumor characteristics on MRI (lesion location, volume, and number; contrast enhancement; necrosis; proximity to the subarachnoid space; and edema).
Methods
This retrospective single-institution analysis was approved by the institutional review board, and the need for informed consent was waived. We searched electronic medical records to identify all consecutive patients with PCNSL during the 11-year period from 1 January 2007, through 31 December 2017. Inclusion criteria included having a pathologically confirmed diagnosis of PCNSL, MRI before initiating any therapy, and non-immunocompromised status. Exclusion criteria were having no pathologic verification, being immunocompromised, or having incomplete data in the electronic medical record. All patients underwent MRI before intervention or treatment, and all images were obtained before steroids were administered. All MR images were reviewed by four neuroradiologists.
Images were obtained on MR scanners with field strengths of 1.5 or 3 T. All imaging included T2-weighted and contrast-enhanced T1-weighted scans (0.1–0.15 mmol gadolinium-DTPA per kg of body weight). The MR images were evaluated for lesion location, volume, and number; contrast enhancement; necrosis; proximity to the subarachnoid space; and edema. Enhancement patterns were defined as solid, rim-enhancing, or perivascular. Tumor volumes were measured by using TeraRecon iNtuition software (version 4.4.13.P2; Foster City, CA), which involved auto-segmentation with additional manual contouring in the axial, sagittal, and coronal planes and 3D image overlay to verify segmentation accuracy. Some patients also underwent diffusion-weighted MRI. The survival duration was calculated (in months) between the date of biopsy and the date of death, or, for patients who were still alive at the time of this analysis, from the date of biopsy until the analysis cut-off date. OS was assessed by Kaplan–Meier analysis, and differences were compared with log-rank tests. Comparisons between two groups were conducted with Student’s t tests. Percentages and categorical outcomes were compared by using chi-square tests. Results were considered significant when the p value was ≤0.05. Statistical analyses were done with SPSS and GraphPad Prism 7 software.
Results
Patient, tumor, and imaging characteristics.
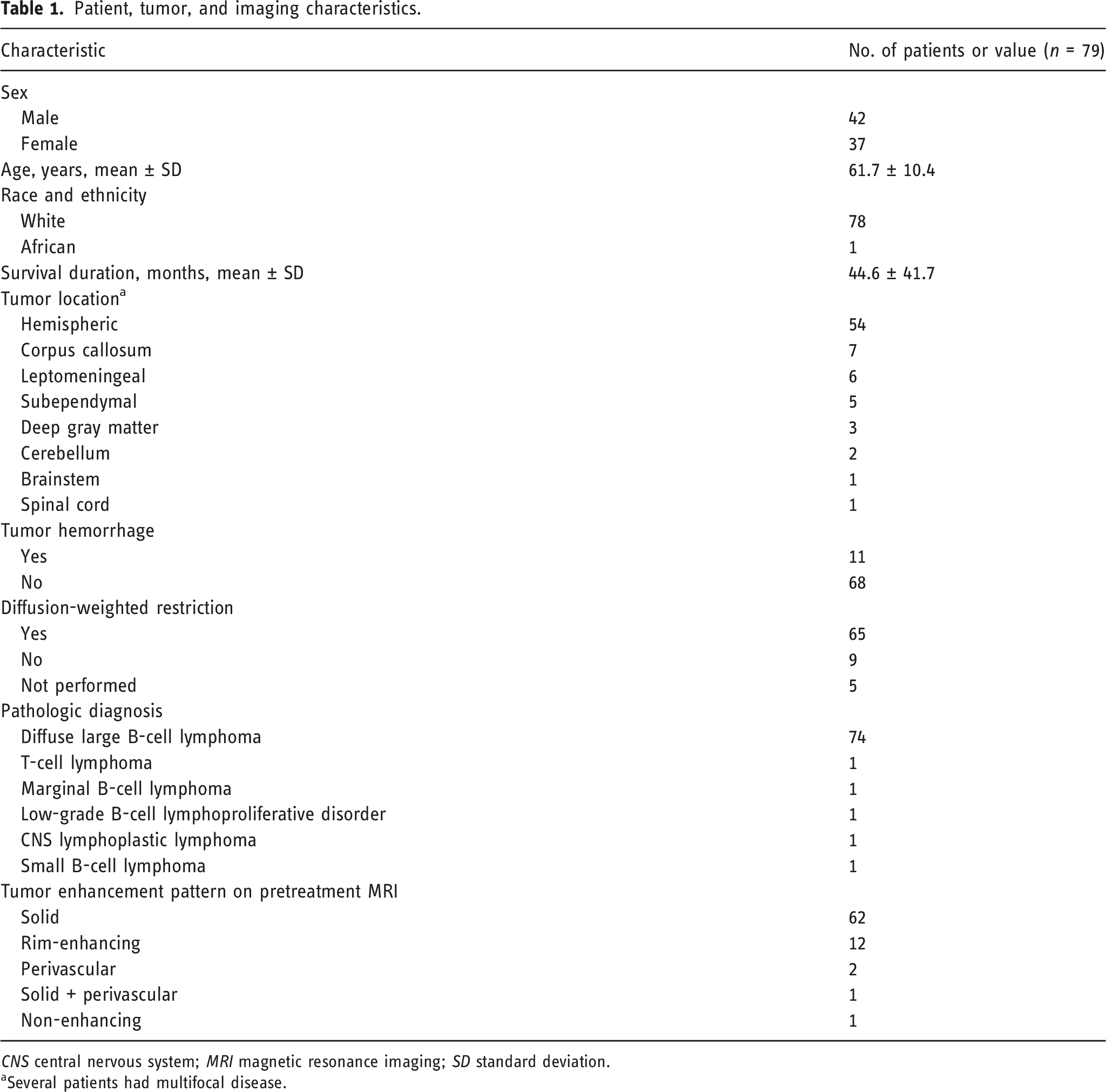
CNS central nervous system; MRI magnetic resonance imaging; SD standard deviation.
aSeveral patients had multifocal disease.
Most tumors were supratentorial; 54 of 79 patients had a hemispheric lesion. Fifteen patients had 39 subcortical tumors, defined as tumors affecting the corpus callosum, basal ganglia, thalamus, subcortical white matter tracts, and insula. Only two patients had solely subcortical tumors, one in the corpus callosum and the other bilaterally in the basal ganglia. Three patients had tumors in the cerebral hemispheres and the corpus callosum. Leptomeningeal tumors were found in six of the 79 patients; six had leptomeningeal disease with focal parenchymal lesions at additional locations. Five patients had subependymal tumors. One patient had an isolated cervical spine tumor, and another had brainstem and third cranial nerve involvement. Most tumors (n = 68 of 79, 86%) did not show hemorrhage, and most (65 of 79, 82%) showed restricted diffusion. In terms of pathologic diagnosis, most cases (74 of 79, 94%) were diffuse large B-cell lymphoma (DLBCL); two were germinal-center-type DLBCL, two were positive for Epstein-Barr–encoded RNA, three were positive for Epstein-Barr virus, and one was low-grade DLBCL. The other 66 DLBCLs were of the non-germinal–center type. Tumors in the other five patients were T-cell lymphoma, marginal zone B-cell lymphoma, low-grade B-cell lymphoproliferative disorder, CNS lymphoplastic lymphoma, and small B-cell lymphoma (Table 1).
The pattern of enhancement on contrast T1 MRI was most often solid-enhancing (62 patients), followed by rim-enhancing (12 patients), perivascular (two patients), and both solid and perivascular enhancement (one patient). Only one patient had CNS disease that did not show contrast enhancement (Figure 1). Magnetic resonance images from a 56-year-old male with a non-contrast–enhancing primary CNS lymphoma. (a) The image is a contrast-enhanced T1-weighted MRI. (b) The image is a corresponding FLAIR image demonstrating a hyperintense signal involving the white matter of the superior right temporal gyrus, extending along the temporal stem to the right periatrial white matter.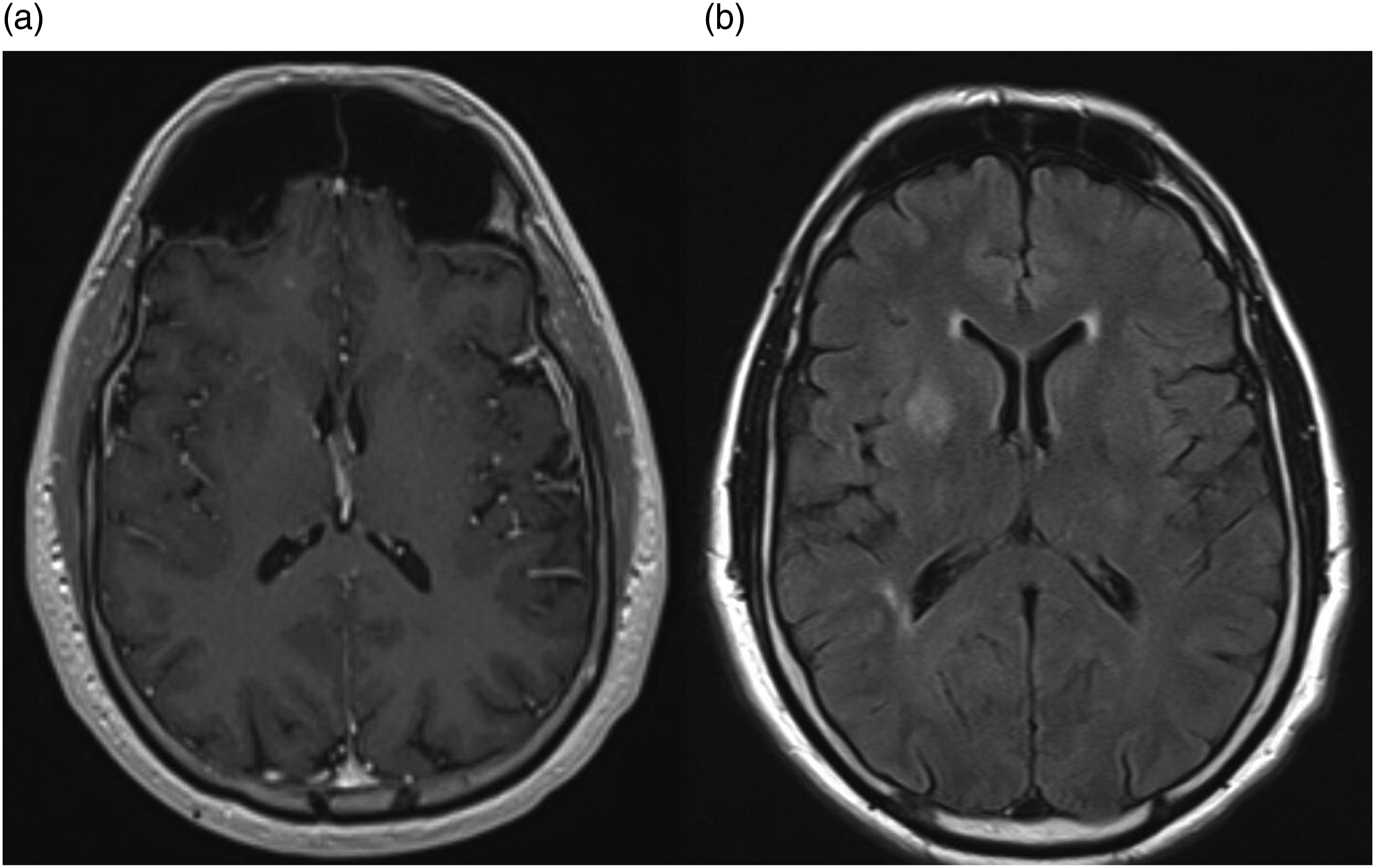
Numbers, volumes a , and locations of primary CNS lymphomas in 76 patients.
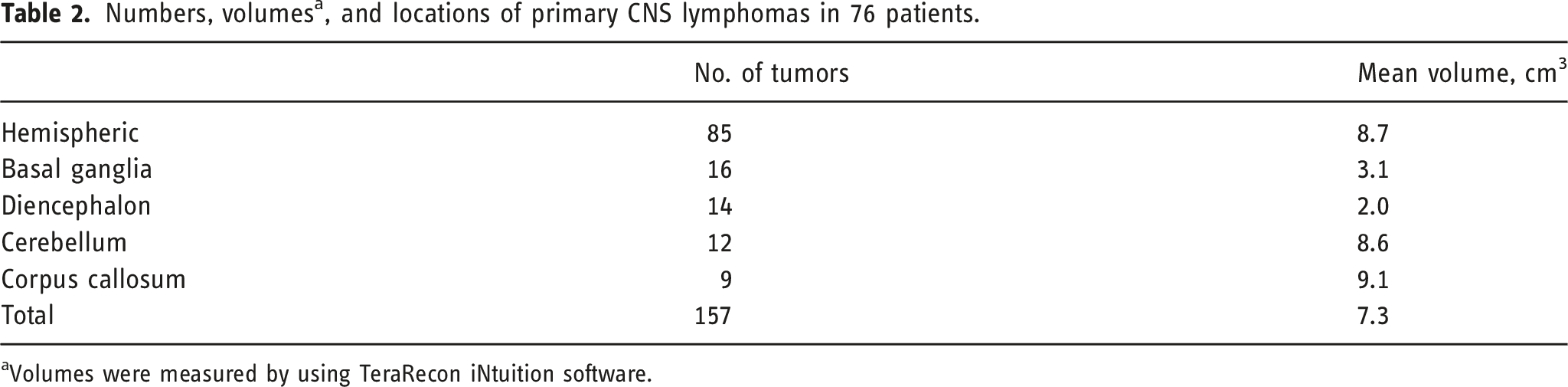
aVolumes were measured by using TeraRecon iNtuition software.
Discussion
Summary of pretreatment imaging findings from the largest published series. Dynamic contrast enhancement (DCE), apparent diffusion coefficient (ADC), progression-free survival (PFS), cerebral blood volume (CBV), F-fluorodeoxyglucose (FDG), susceptibility weighted imaging (SWI), intratumoral susceptibility signal (ITSS), and overall survival (OS).
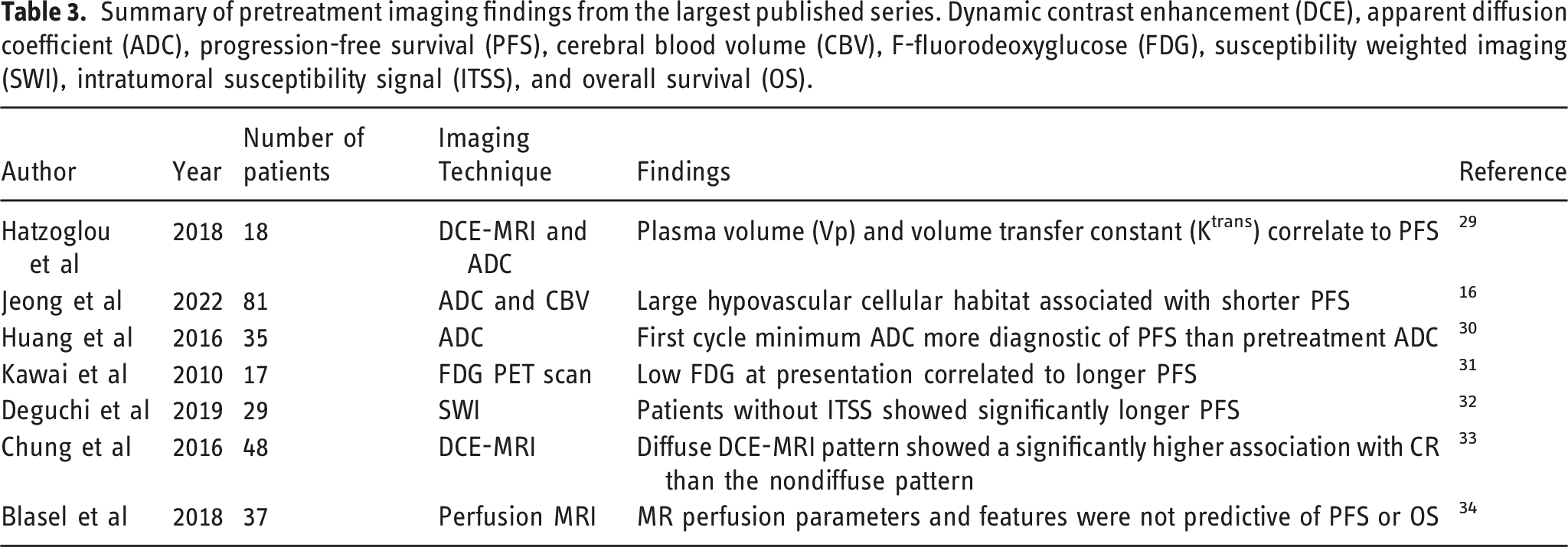
The sole patient with a non-enhancing lesion in our study was still alive, with no visible lesions on MRI, at 83 months’ follow-up and was undergoing surveillance MRI every 3 months. The rarity of PCNSL in general, plus the technological advances in MRI over time, underscores the need for a pooled analysis of additional patients to compare survival duration between contrast-enhancing versus non-contrast–enhancing T1 lesions. Of those that have contrast-enhancing lesions, some studies suggest ADC measurements of PCNSL tumors may provide noninvasive insight into clinical outcome.10,14,15 Recently, larger scale studies have demonstrated that pretreatment hypovascular cellular tumor habitat as defined by ADC and CBV values are predictive of time to progression within this patient population. 16
Our cohort included six patients with leptomeningeal disease, a location that is historically associated with the worst prognosis.
17
All six of these patients had leptomeningeal disease, plus disease in other locations (Figure 2). Four of the six patients were still alive at the time of data analysis, with a mean OS duration of 56.4 months after diagnosis (range 2.3–96.5 months) for those diagnosed with leptomeningeal disease. Historically, patients with PCNSL with leptomeningeal seeding survive for only about 4–5 months,
17
although advances in treatments have extended the survival time in some cases. In a review from the International Primary CNS Lymphoma Collaborative Group, Taylor et al.
17
reported a mean survival duration of 24 months after diagnosis for patients with primary leptomeningeal disease who received treatment (fractionated radiotherapy [36%], systemic chemotherapy [78%], and intrathecal chemotherapy [66%]), with 66% (48 patients) receiving two or more forms of treatment. Our results may be due to early detection and management, but this should be an area of focus of future studies. Magnetic resonance imaging from a 42-year-old male with a contrast-enhancing primary CNS lymphoma. (a) Coronal post contrast-enhanced T1-weighted MRI showing leptomeningeal disease along lateral ventricle. (b) Axial post contrast-enhanced T1-weighted MRI showing leptomeningeal disease along prepontine cistern and third ventricle.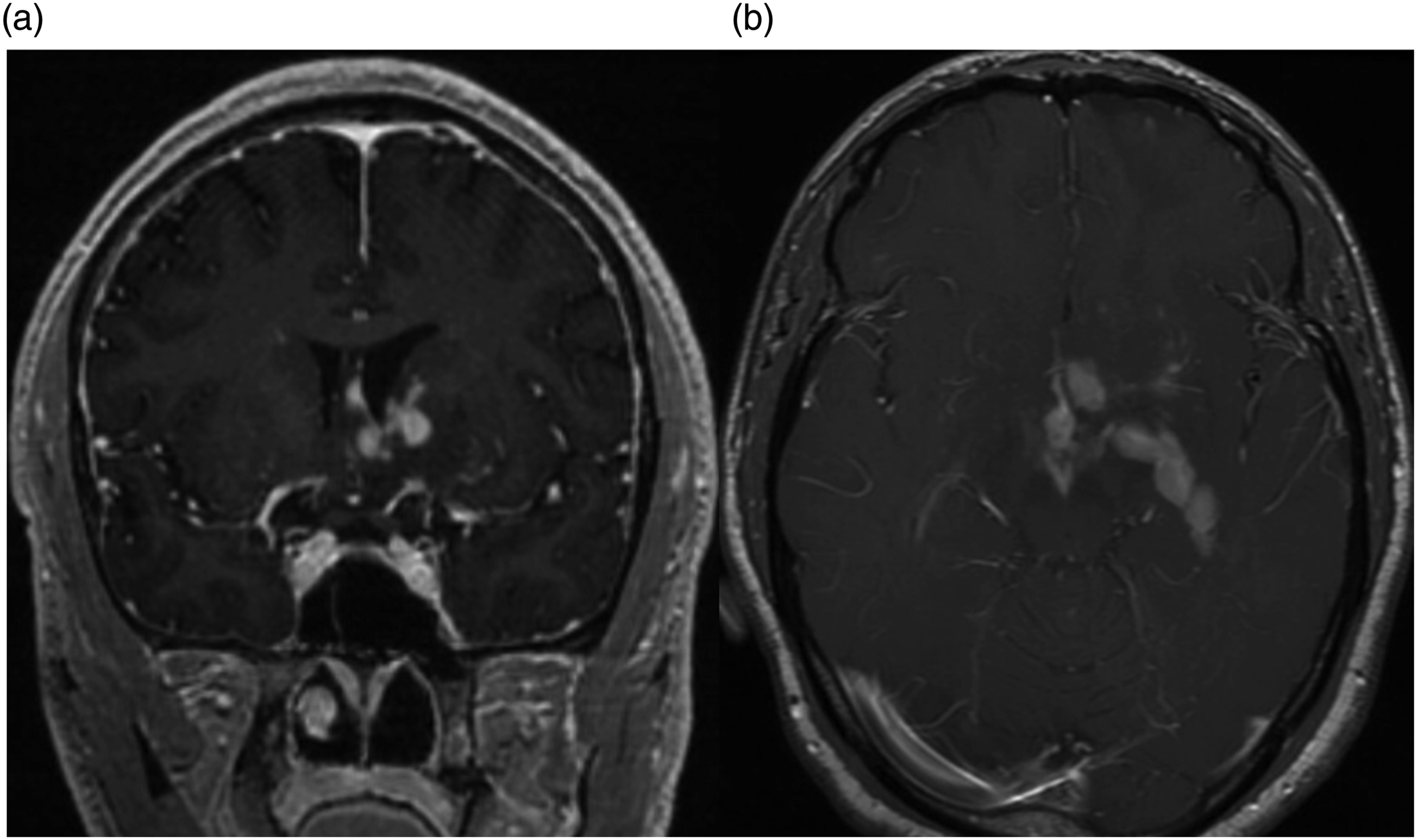
Hemorrhagic lesions, another atypical finding in PCNSL, also occurred more often in our study than in previous reports (in 14% versus 2–8%)18–20 (Figure 3). There was another smaller study showing that small intratumoral hemorrhages occurred in 4 (21%) of 19 lesions.
21
More surprisingly was that the mean OS among of our patients with observed hemorrhages was 25.5 ± 11.0 months (range 2.3–97.2 months) which is much higher than previously reported of 7–10 months.
22
This will be further verified and may be an entity that needs further exploration. Magnetic resonance imaging from a 59-year-old male with a primary CNS lymphoma. Minimal hyperintensity on SWI (a) and T2 hypointensity (b) consistent with hemorrhagic changes within the large lesion. Images demonstrate significant surrounding vasogenic edema which involves the left parietal lobe. (c) MRI images of a contrast-enhancing lesion in the posterior inferior left parietal lobe.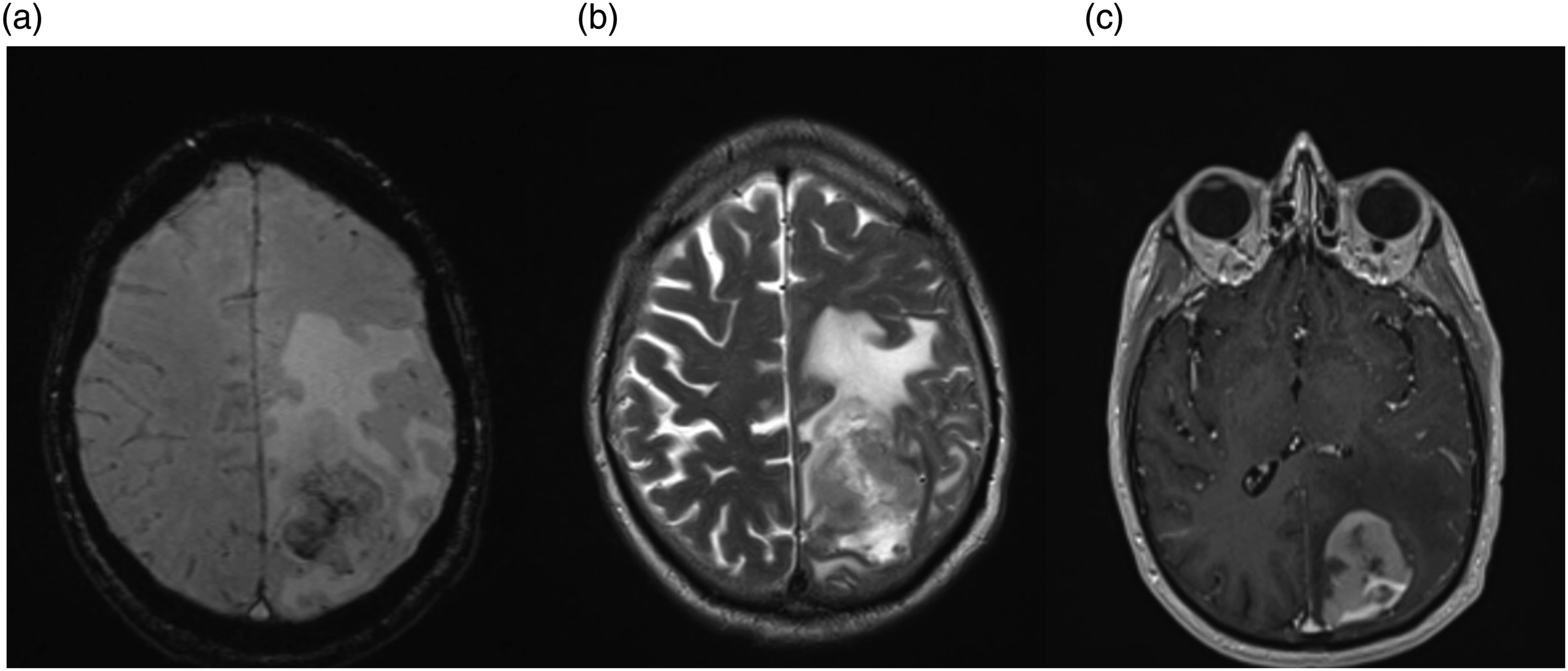
The wide range of OS durations in our study (0.3–151.3 months) likely reflects variations in the course of various subtypes of PCNSL, as well as changes in treatment strategies over time. Most of the information from clinical trials available to date is based on the use of high-dose methotrexate-based therapy for PCNSL (70 patients, 88.6%); this treatment approach seems to extend survival duration, with fewer toxic effects.23–25 Indeed, one clinical trial of high-dose methotrexate-based therapy had an 8-year survival rate of 57%. 23 In our study, OS was longest among patients given chemotherapy only: most patients (n = 67 patients, 84.8%) underwent chemotherapy only, mostly methotrexate-based, and had a mean OS time of 47.9 ± 41.6 months, which is consistent with others’ experience. 26
Another treatment option for PCNSL, autologous stem cell transplantation after induction chemotherapy, was given to six patients in the current study; the mean OS duration for those patients was 10.9 ± 6.2 months. Although the number of patients in this subgroup was too small for a powered survival analysis, one clinical trial had an OS rate of 65% at 4 years, and another had an OS rate of 81% at 2 years.27,28 Further analysis will be needed to define this population.
The current study had several limitations, chief among them being its retrospective nature and the associated biases; it also included a relatively small number of patients. Incomplete data related to imaging, diagnosis, and treatment contributed to the small sample size as those patients were excluded from our analysis. Future studies of rare imaging presentations of PCNSL should consider pooling their data with published findings to reach sufficiently large sample sizes to allow meaningful correlations.
Conclusions
Our findings, obtained over an 11-year period at a single institution, suggest that some patients with PCNSL survive longer than had previously been thought, most likely because of advances in treatment. In addition, the sole patient in the current study with non-enhancing PCNSL was found to have a low-grade PCNSL lesion, raising the possibility that non-enhancing tumors may be less aggressive than enhancing tumors. Lastly, our subset of patients with leptomeningeal disease on MR imaging had a longer survival than previously reported. Further studies are needed to characterize the histologic makeup of non-enhancing PCNSL to further link imaging findings with prognosis as well to have better characterize patient with leptomeningeal disease.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Kristin Huntoon, Mina S. Makary, Varun Shah, Anthony Aquino, and Vijay Pandya. The first draft of the manuscript was written by Kristin Huntoon and Varun S. Shah and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.