
Abstract
Orbital metastases secondary to neuroendocrine tumors are exceedingly rare. We present a unique case of a 30-year-old female initially presenting with fever, chills, periorbital swelling, and painful proptosis. CT orbits revealed two ovoid-shaped ring-enhancing lesions in the right lateral and superior rectus muscles and clear sinuses, atypical for infectious post-septal cellulitis. Further work-up included serologic analysis, auto-immune panel, and MRI. Further imaging showed pseudocystic orbital lesions mimicking orbital cysticercosis. Additionally, given the bilateral nature of the lesions and patient’s country of origin, this parasitic process was highly suspected. A course of albendazole and steroids led to resolution of symptoms. With a presentation at age 30, this is by far the youngest case reported in literature to date.
Case description
Summary of Case Presentation.
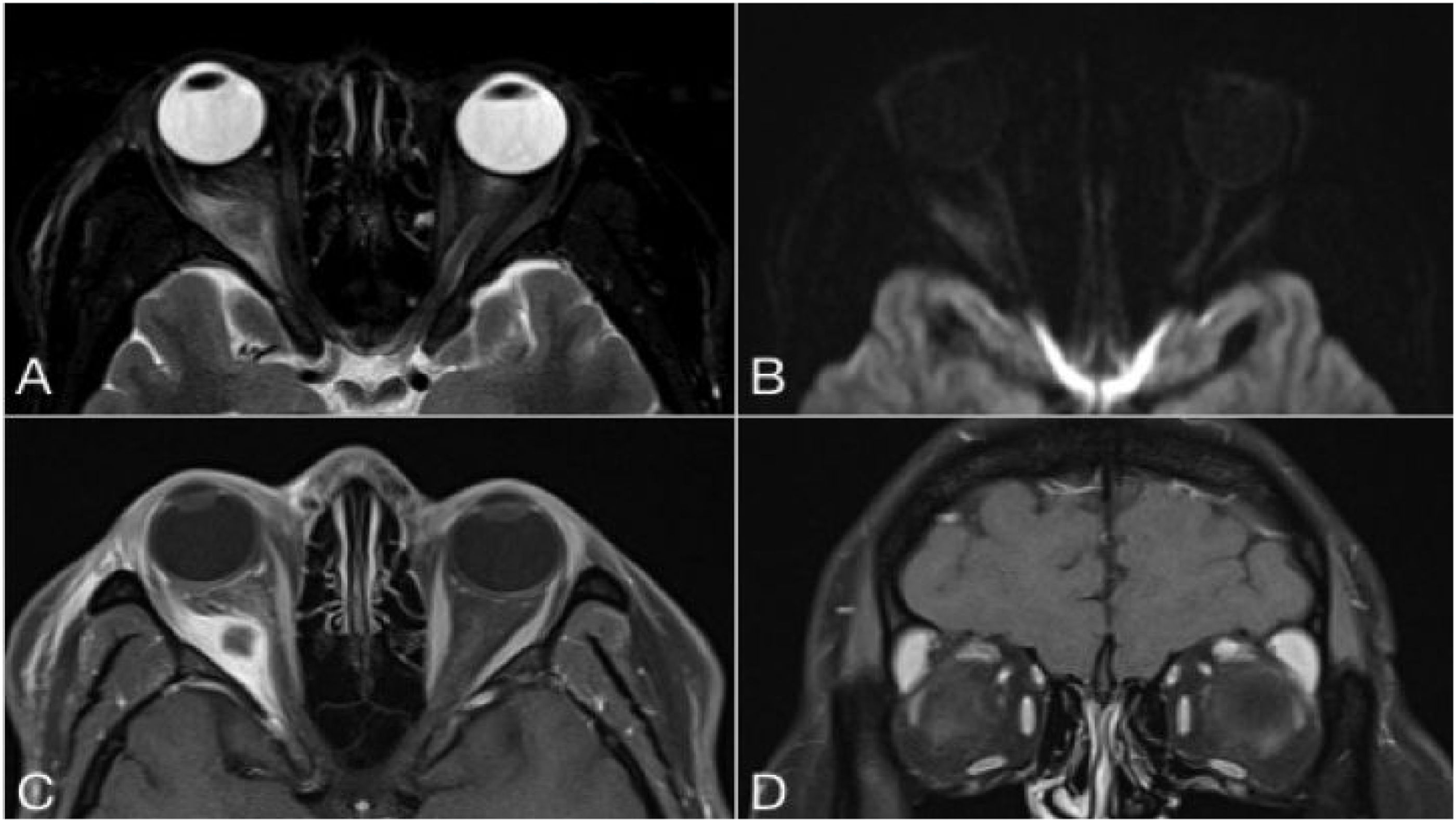
MRI orbits.
Orbital biopsy was discussed but deferred due to non-compliance and accessibility concerns. Differential diagnosis for this presentation included orbital abscess, idiopathic orbital inflammation, granulomatosis with polyangiitis, orbital lymphoma, orbital metastasis, and orbital cysticercosis. Given the bilaterality of the lesions and the patient’s country of origin, a parasitic process, specifically, orbital cysticercosis, was suspected, despite low eosinophil count and negative taenia solium serology. A course of albendazole, along with steroids was initiated, which led to the resolution of her symptoms.
Eight weeks after her initial presentation, she presented to the ER with a 3-day history of nausea, vomiting, diarrhea, fevers, fatigue, and weakness. Abdominal sonography and CT ordered for iron deficiency and elevated liver enzymes showed a 3cm mass, arising from the neck of the pancreas, along with numerous lesions in kidneys, liver, T12 vertebral body, and periaortic/retroperitoneal lymphadenopathy. The hepatic lesions were easily amenable to ultrasound-guided biopsy and three 18-gauge core biopsies of one of the lateral right lobe hepatic masses were obtained. The histopathological sections revealed a metastatic tumor composed of monomorphic cell proliferation, with insular growth pattern and rare mitoses (Figure 2). The neoplastic cells were positive for Synaptophysin, Chromogranin, and CDX2. The proliferative index was low (ki 67 of 4%). In view of these findings, the tumor was diagnosed as a metastatic neuroendocrine tumor, grade 2. Given the upper endoscopic findings of extrinsic compression of gastric antrum/pylorus, this metastatic tumor is in keeping with a primary pancreatic origin. Her clinical symptoms and initial presentation were probably due to a carcinoid paraneoplastic syndrome. Dual-chemotherapy with temozolomide and capecitabine were recommended by the local cancer agency. Sadly, her visitor health insurance refused to cover medical expenses for this treatment. Thus, she was transferred back to India for further care. Diagnostic challenge and delay were driven by the unusual demographic presentation of an extraordinarily rare malignancy and a deferral of orbital biopsy due to health insurance limitations. In terms of time-frame, the patient initially visited a hospital in Surrey, British Columbia, Canada, when her symptoms began on July 2018 where she was worked up for her orbital involvement. After her initial course of treatment, she was discharged and represented in September 2018 where she was seen by internal medicine and had abdominal imaging done. This eventually revealed the metastatic neuroendocrine tumor. As such, the diagnosis took approximately two months from the patient’s initial date of presentation. Histopathology. Low-power views showing the insular growth pattern of the tumor (hematoxylin-eosin, original magnifications x40).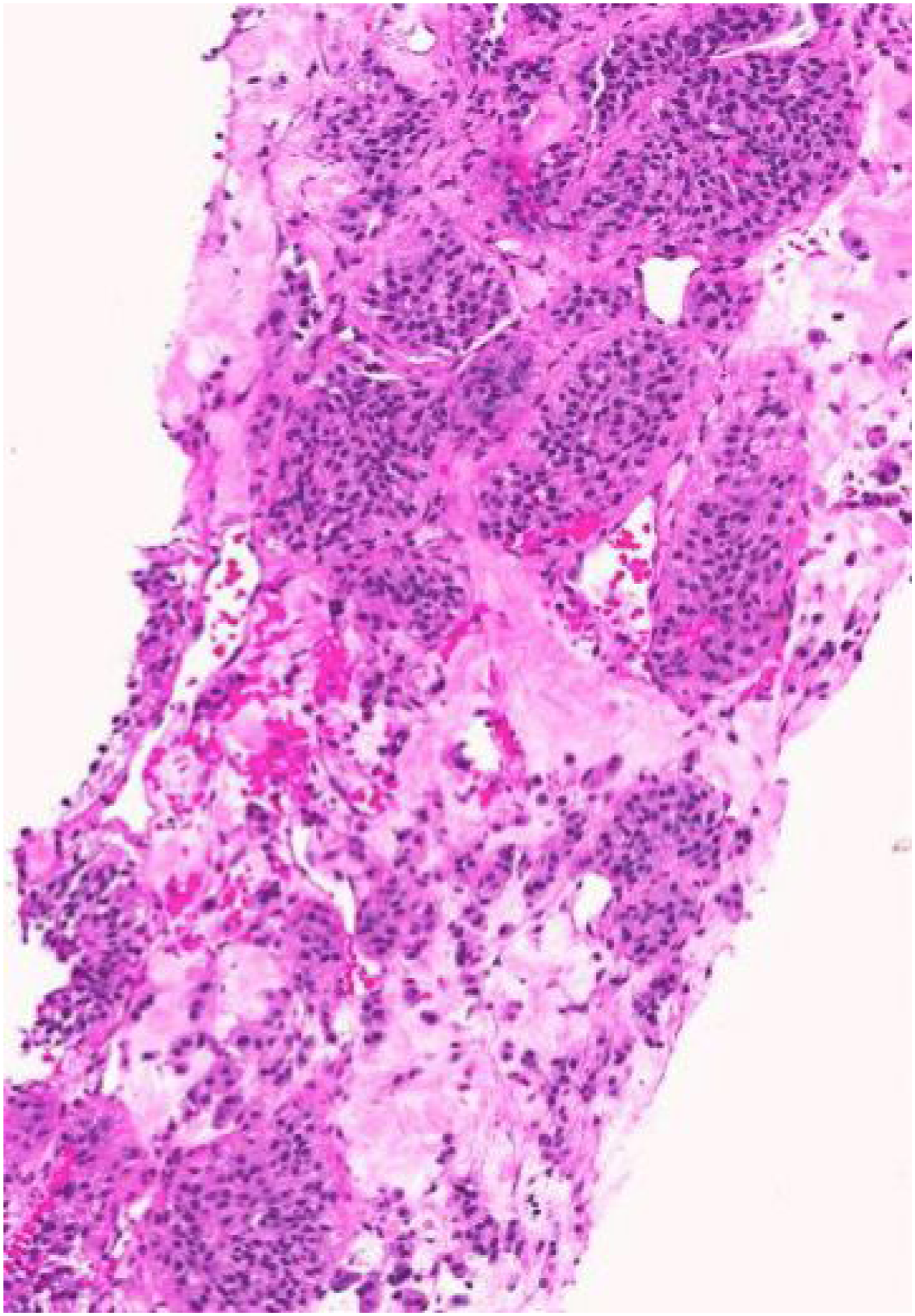
Discussion
Orbital metastases secondary to neuroendocrine tumors are exceedingly rare, with less than 40 cases reported to date. Initial presentation with ocular symptoms is even less common. 1 Average age at diagnosis is 67.5 years (range 42–79).1–3 With a presentation at age 30, this is by far the youngest case reported in literature to date. Similar to previous publications, imaging showed pseudocystic orbital lesions mimicking orbital cysticercosis. 4 Das et al. found that surgical biopsy of the orbital lesion is not necessary for diagnosis in the setting of a previously established diagnosis, systemic metastases, and classic radiologic findings, especially with the use of new imaging modalities such as 68Ga-DOTATATE PET-CT. 2 These novel imaging modalities may lead to a more frequent identification of orbital metastases from neuroendocrine tumors in the near future. In strong contrast to other primary malignancies with orbital metastases, patients with orbital involvement from neuroendocrine tumors carry an excellent prognosis, with 10-year survival rates of close to 40%. 3 In addition to systemic chemotherapy and surgical options, 177Lu-DOTATATE peptide radionuclide receptor therapy has been suggested for patients with symptomatic metastases from orbital involvement.3,5
Das et al. documented five patients with orbital metastases from neuroendocrine tumors and found that four patients had bilateral involvement in the form of extraocular masses seen in the recti or focal thickening of the muscles. 1 One patient had unilateral involvement of a mass found in the left lateral rectus. Mehta et al. investigated 13 cases of patients and found there to be no bias to the side of the presentation as six right eyes and seven left eyes were involved. 6 Our study clinically presented with the patient having the right eye involved (proptosis, epiphora, and swelling), but on imaging was found to have both eyes affected. Based on our study and previous literature, it appears that other orbital structures are typically not involved and it is the recti muscles that are affected. Furthermore, there does not appear to be a predilection in terms of laterality, the muscles affected, or which eye is typically involved. More cases would be needed in order to draw conclusions about a clear pattern.
Orbital involvement as the first clinical presentation of a neuroendocrine tumor is exceedingly rare and highlights the importance of a thorough initial work-up and a comprehensive differential diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.